
Abstract
Background
The suture-bridge technique (SBT), with its various modifications, is frequently utilized in rotator cuff tear repairs. This study aimed to assess and compare the clinical and radiological tendon integrity outcomes of conventional and triple-row SBTs in patients with full-thickness rotator cuff tears (RCTs). Additionally, it evaluated the construct strength of each technique through biomechanical experiments. We hypothesized that the triple-row SBT would yield better clinical and radiological outcomes, as well as superior biomechanical properties, compared to the conventional SBT.
Methods
A retrospective evaluation was conducted on 62 patients who underwent arthroscopic rotator cuff repair using either conventional or triple-row SBT from January to December 2019. The conventional SBT was performed on 26 patients, while the triple-row SBT was used on 36 patients. Clinical evaluations were conducted preoperatively, and at 1 and 2 years post-surgery using the ASES; UCLA; Constant scores; and VAS scores. Magnetic resonance imaging was performed before surgery, and the postoperative rotator cuff integrity was evaluated 6 months after surgery. Mechanical testing on seven pairs of sawbone and allodermal patch models was also performed. These specimens underwent horizontal and vertical axial load tests on a material testing machine, and the ultimate failure load was measured.
Results
Both techniques significantly improved the clinical outcomes at postoperative 1 and 2 years (p < .001), with no significant difference between-group (p > .05). The retear rate was 19.2% in the conventional group and 11.1% in the triple-row group, but the difference was not statistically significant (p = .379). The failure load of the triple-row suture-bridge technique was higher than that of conventional suture-bridge technique.
Conclusion
Both the conventional and triple-row SBT techniques were effective in achieving favorable clinical outcomes in patients with full-thickness rotator cuff tears, with no statistically significant differences between the two groups. Although the triple-row technique suggested a potential for a reduced retear rate, the difference was not statistically significant. However, in our biomechanical study, the triple-row SBT demonstrated superior mechanical stability compared to the conventional technique. Specifically, the triple-row configuration showed greater resistance to displacement under cyclic loading and improved load distribution across the repair site. These findings suggest that the triple-row SBT may offer biomechanical advantages that could contribute to enhanced structural integrity of the repair, especially in challenging cases.
Keywords
Introduction
Rotator cuff tears (RCTs) are a common cause of shoulder pain, and arthroscopic rotator cuff repair (RCR) is a major treatment. 1 The primary goal of RCR is to achieve strong initial fixation and minimize the chances of gap formation, thus promoting effective tendon-bone healing essential for positive functional outcomes post-repair.2,3 With advancements in arthroscopic techniques, various methods have been developed for RCR, including the application of the double-row technique to improve the mechanical strength, reduce gap formation, improve tendon-to-bone contact, and increase footprint coverage. 4 The suture-bridge technique (SBT) has become a popular double-row technique. Moreover, cadaveric studies have shown that the SBT improves the footprint contact area and mean footprint pressure compared to conventional double-row repairs. 5 Nonetheless, tension-free tendon repositioning and optimal footprint coverage are not always achievable with SBT. 6 The retear rates of double-row and SBT have been reported at 10%–30%.2,7,8 In particular, retear rates of 40%–64% have been reported for double-row repair of large and massive tears.2,8
Triple-row SBT was first introduced by Ostrander and McKinney 9 in 2012 and Ostrander et al. 10 in 2016. They provided biomechanical descriptions of triple-row SBT that improved footprint coverage and increased contact pressure, thereby enhancing healing of the tendon to the bone and potentially lowering the retear rate. However, the specifics regarding the knotting sequence of the triple-row method were not detailed. Subsequently, Buckup et al. 11 introduced the triple-row modified SBT and provided detailed reports on the knot sequence and technical aspects. They repaired 82 RCTs with triple-row SBT and showed a retear rate of 4.9% at the 3-year follow-up. They emphasized the advantages of the triple-row SBT, which include more effective tendon alignment, the facilitation of tension-free medial row knotting, an improved tendon-bone interface, and extensive footprint coverage, collectively enhancing the overall stability. However, they also mentioned that additional randomized comparative studies between triple-row SBT and conventional SBT are needed.
To our knowledge, there has been a lack of direct comparison between the clinical and radiological outcomes of conventional and triple-row SBTs. Similarly, the relationship of these outcomes with biomechanical test results has not been explored. Therefore, this study aimed to assess and compare the clinical and radiological tendon integrity outcomes of the conventional and triple-row SBTs in patients with medium- to large-sized full-thickness RCTs, and to evaluate the construct strength of the each techniques using biomechanical experiments. We hypothesized that triple-row SBT repair would provide better clinical and radiological outcomes and superior biomechanical properties than conventional SBT.
Materials and methods
Clinical study
Patient selection
Demographic and surgical data of conventional SBT and triple-row SBT.

Data are expressed as mean ± standard deviation (range) or number (percentage).
SBT Suture-bridge technique.
aPaired t test; p < .05, statistically significant.
Surgical procedure (Intervention)
In our study, all surgical procedures were carried out by a single surgeon (corresponding author). Patients were placed in the beach-chair position under general anesthesia and and given an interscalene nerve block for optimal comfort and safety. When indicated, acromioplasty was conducted on those presenting with type III acromial morphology or subacromial spurs, while none of the cases involved biceps tenotomy. While viewing the posterolateral or lateral portal, the distance from the anterior to the posterior end of the RCTs was measured using a calibrated probe through the anterior or posterior portal. Subsequently, the surgeon debrided the rotator cuff tendon and refreshed the footprint.
During conventional SBT, we used one or two Healicoil Peek suture anchors (4.5 or 5.5 mm; Smith & Nephew, Andover, MA, USA) loaded with two No. 2 non-absorbable braided sutures. The medial row anchor was inserted just lateral to the articular surface of the humeral head, and the sutures were passed through the tendon in a horizontal mattress suture. If necessary, two medial row anchors were inserted according to RCT size, and one medial row anchor was used for small RCT. The second medial row anchor was inserted following the identical procedure.
12
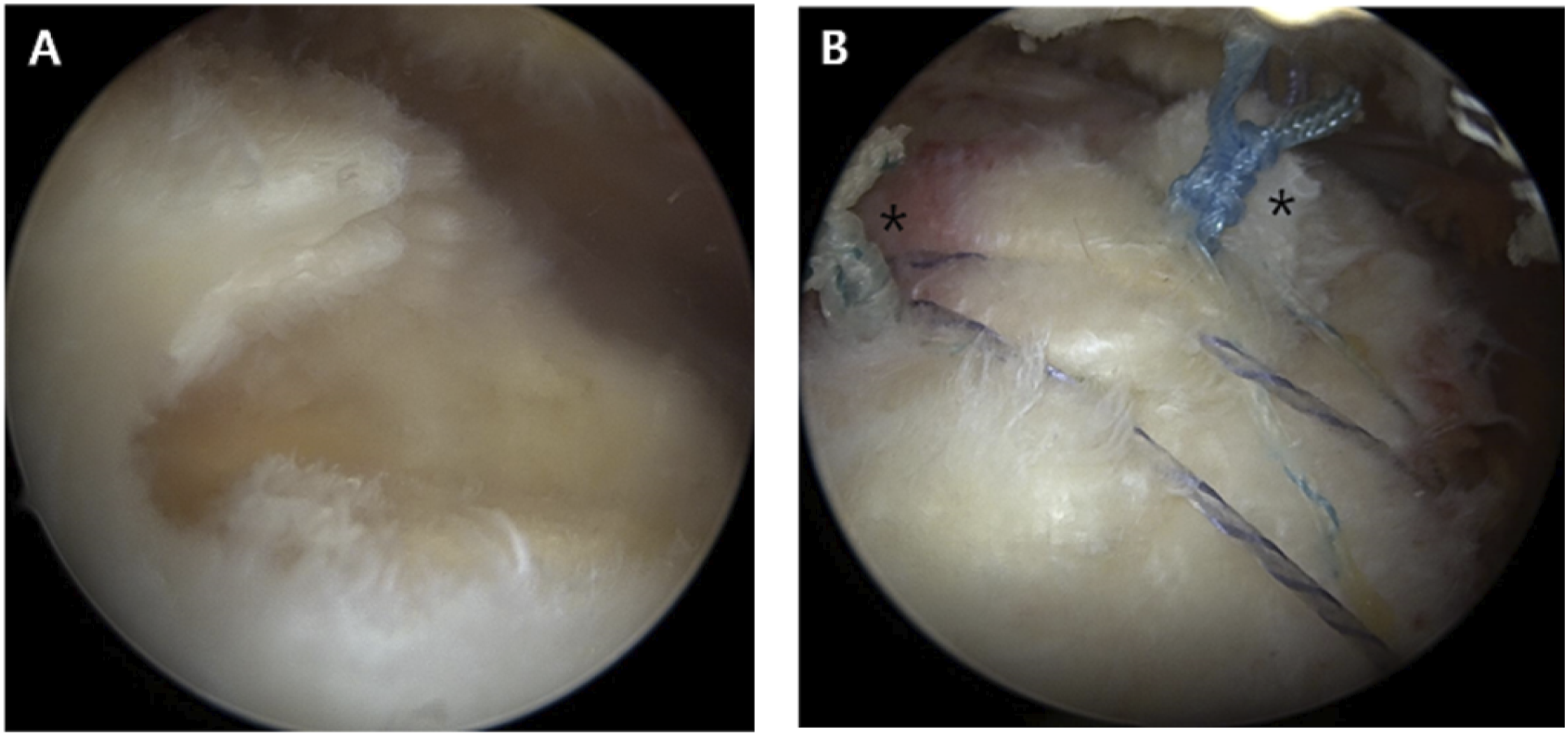
Subsequently, the medial row anchors were mattress knotted to reestablish the rotator cuff footprint. To establish the lateral row, medial row sutured limbs were crossed over the tendon and two knotless 5.5 Footprint Ultra PK anchors (Smith & Nephew, Andover, MA, USA) were inserted perpendicular to the cortical surface of the humerus 5 to 10 mm distal to the lateral edge of the greater tuberosity (Figure 1).
For the triple-row SBT (Figure 2), medial-row anchors were inserted one or two Healicoil Peek suture anchors (4.5 or 5.5 mm; Smith & Nephew, Andover, MA, USA) in the same way as the conventional SBT. Before the sutures were tied in the medial row, one or two Healicoil Peek suture anchors (4.5-or 5.5 mm) were inserted in the middle row (lateral edge of the footprint) for anatomical reduction of the tendon, and the middle-row anchors were initially simple sutures. The mattress suture was performed in the medial row after tying the middle-row anchors. Finally, similar to conventional SBT, it was fixed with two Multifix S Ultra anchors (5.5 mm; Smith & Nephew, Andover, MA, USA) in the lateral row (Figure 3). The triple-row SBT consists of several steps in repairing a model of a rotator cuff tear. 
Postoperative management
All patients underwent the same postoperative rehabilitation at a single hospital. Post-surgery, the shoulder was immobilized for a period of 6 weeks using an abduction brace set to maintain 30-40° of internal rotation and 20° of abduction. Active elbow flexion-extension, forearm supination-pronation, and hand and wrist motions were allowed at immediate postoperative day. The patient performed gentle passive forward flexion at 4 weeks after the surgery. Six weeks after the operation, the abduction brace was removed, and active full-range of motion exercises were recommended. 12 weeks after surgery, gradual active resistance-based muscle-strengthening exercises were initiated using TheraBand equipment (HCM-Hygenic Corp., Batu Gajah, Malaysia). At 3–4 months after surgery, the patients began light physical and sports activities, and approval for heavy labor was obtained at 6 months after surgery.
Clinical and radiological evaluation (Comparison & Outcomes)
Functional clinical assessments were conducted on all participants before surgery, and then again at the 1- and 2-year postoperative intervals. The clinical evaluation included four items: scores from the American Shoulder and Elbow Surgeons (ASES), the Shoulder Rating Scale of the University of California at Los Angeles (UCLA), Constant scores, and pain levels measured using the Visual Analog Scale (VAS). For assessing active range of motion (ROM), a goniometer was used, while passive ROM was not evaluated in this study. ROM measurements were carried out with the patients in a standing position, focusing on external rotation with the arm in an adducted position. The clinical data, collected both before and after the surgery, were sourced from orthopedic surgeons not involved in the execution of this study. Shoulder radiography and MRI were performed preoperatively in all patients. All MRI examinations were performed using 1.5-Tesla or 3.0-Tesla superconducting magnets. The medial-to-lateral length of the RCTs was measured using oblique coronal preoperative T2-weighted MRI. All measurements were performed by the first author.
Clinical and surgical data of conventional SBT and triple-row SBT.

Data are expressed as mean (range) or number (percentage).
SBT suture-bridge technique, MRI magnetic resonance imaging, US ultrasonography.
Test; p < .05 denotes statistical significance.
aPaired t test and χ 2 .
Statistical analyses
Data are shown as mean ± standard deviation or in percentage form. To evaluate differences between the conventional SBT and triple-row SBT, paired t -tests and chi-square (χ 2 ) tests were employed. All statistical analyses were conducted using SPSS software (version 25.0; IBM Corporation, Armonk, NY, USA), with a p-value of less than 0.05 deemed indicative of statistical significance
Experimental biomechanical study
Materials
We devised a uniform model for rotator cuff repair employing sawbones and acellular dermal matrix (ADM) grafts to overcome the limitations noted in prior cadaveric research, particularly those associated with biomechanical testing. When using human and animal tendons or bones, it is difficult to accurately adjust the size and quality of the materials. Therefore, we attempted to reduce bias by using synthetic sawbones and standardized ADM grafts. The test sawbones used in this study were synthetic bones (Humerus, 4th Gen Composite Humerus, 10# solid foam cancellous core, Sawbones, Vashone, WA, USA). The ADM graft used was BellaCell ADM(Hans care. Corporation, Korea), a decellularized dermal graft specifically designed to mimic native tendon properties. ADM graft is composed of extracellular matrix (ECM) components such as collagen and elastin, which promote tissue integration and mechanical stability. For our biomechanical testing, the ADM grafts were standardized to a size of 4.5 cm × 5.5 cm with a thickness of 4 mm, ensuring consistency across all samples. In this experiment, the ADM graft was utilized as a substitute for the rotator cuff tendon, simulating the repair of full-thickness rotator cuff tears. This approach allowed us to evaluate the mechanical performance of the suturing configurations while minimizing variability in material properties typically associated with human or animal tendons. By serving as a uniform surrogate for the native tendon, the ADM graft ensured that observed differences between suture configurations were attributable to the techniques themselves rather than inconsistencies in the repair material. The integration of these materials into our experimental setup is illustrated in Figure 4.
Repair techniques
A solitary investigator executed all suture techniques to ensure consistency across our rotator cuff model study. We divided the rotator cuff models into two groups based on the suture methods: conventional SBT and triple-row SBT.
For the conventional SBT group, medial row anchor holes were drilled along the margin of the articular cartilage within the supraspinatus footprint. Triple-loaded suture anchors (5.5-mm PEEK Healicoil; Smith & Nephew, Andover, MA, USA) were then secured into these holes. These medial anchors were placed at a 45° angle to the footprint’s surface for optimal fixation. Following this, a pair of lateral anchors (5.5-mm Multifix S anchor; Smith & Nephew) were inserted, spaced 20 mm apart and positioned lateral to the medial row at the edge of the lateral footprint. The placement of each lateral anchor was done meticulously to align with the medial anchors, which were spaced 12.5 mm apart in the anterior-posterior direction. For the triple-row SBT group, the procedure for medial row anchors mirrored that of the conventional SBT group. Additionally, middle-row anchors (5.5-mm Healix; DePuy Synthes Mitek, Raynham, MA, USA) were placed 10 mm apart from the medial anchors and inserted at a 45° angle along the lateral margin of the greater tuberosity (GT) footprint. Next, two lateral anchors were inserted, similar to the conventional SBT (placed 20 mm from the medial anchor and 10 mm from the middle anchor).
The number of anchors was standardized across both techniques to ensure consistency and minimize bias. In the conventional SBT group, 2 anchors were used for the medial row and 2 anchors for the lateral row, making a total of 4 anchors. In the triple-row SBT group, 1 anchor was used for the medial row, 1 anchor for the middle row, and 2 anchors for the lateral row, also totaling 4 anchors. This deliberate standardization ensured that the observed biomechanical outcomes reflected differences in the suturing configurations rather than variations in anchor usage.
For all models, suturing was standardized using a proprietary sliding knot technique known as the Samsung Medical Center (SMC) knot, which was further reinforced with three alternating half-hitches on alternating posts for added security. The ADM grafts were incorporated into both suture configurations, allowing the biomechanical properties of the techniques to be assessed under consistent conditions.
Mechanical tests
Mechanical testing in our study was conducted using a robust mechanical tensile-testing machine (MTS Exceed Material Test System, Model E43.104; USA). Configured to allow testing in both vertical and horizontal orientations. The allodermal graft was secured by using grasping clamps pulled parallel to the transverse plane of the tendon. The prepared model was tested in tension by pulling 90° ‘and 180’ ° to the shaft of the humerus separately, simulating the position of the patient’s arm at their side (Figure 5). During the testing process, we set the models to be loaded at a consistent extension rate of 40 mm/min. The point of failure for each specimen was meticulously recorded, utilizing data captured and processed by a standard computer system. The specific modes of failure for each test subject were carefully documented for thorough analysis. Experimental test setup. 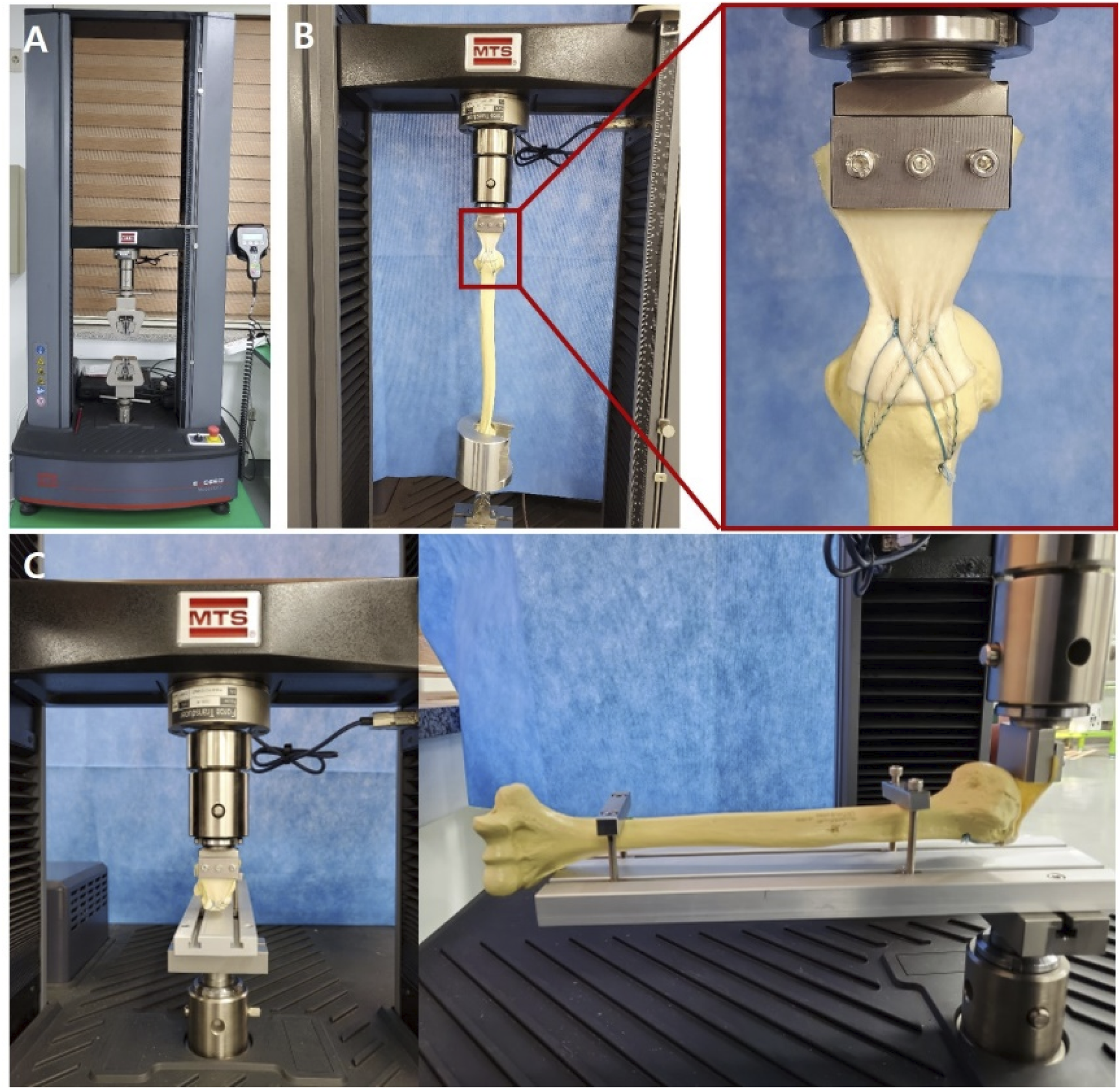
Statistical analyses
Before designing the study, we determined the necessary sample size to ensure adequate statistical power. Aiming for a power of 0.8 and an effect size of 1.2, 15 we based our calculations on data from previous studies16–18 for a paired comparison of failure load. A power analysis was performed with a beta error set at 0.2 (power = 0.8). To achieve this, we conducted a power analysis with a beta error set at 0.2, indicating a power of 0.8. According to this analysis, each group needed a minimum of seven shoulder samples to detect a 20% difference in specimen load to failure between the groups. The results are presented as mean values ± standard deviation.
For statistical analysis, we employed SPSS software (version 25.0; IBM Corporation, Armonk, NY, USA). Given the small sample sizes and the likelihood of skewed distributions, nonparametric tests, specifically the Mann–Whitney U test, were utilized for the experimental analysis. The level of significance was set p < .05.
Results
Clinical results
A total of 62 patients were included in the study, with 26 undergoing the conventional SBT and 36 treated with the triple-row SBT. The mean age at surgery was comparable between the two groups (58.4 ± 8.0 years for conventional SBT vs 59.4 ± 7.9 years for triple-row SBT), with male patients accounting for 46.2% and 52.8%, respectively. The duration of symptoms prior to surgery was slightly longer in the conventional SBT group (8.0 ± 9.0 months) compared to the triple-row SBT group (7.0 ± 7.7 months), but this difference was not statistically significant (Table 1). Subacromial decompression was performed in nearly all patients (96.2% in conventional SBT and 97.2% in triple-row SBT), and the mean operation time was similar between the groups (55.6 ± 14.7 minutes vs 57.1 ± 19.2 minutes). The number of medial or middle row anchors used was determined based on the tear size. The number of middle row anchors was 1.1 ± 0.2 for the triple-row SBT. The total number of anchors used during the operation was 4.08 ± 0.62 for the conventional SBT and 5.06 ± 0.66 for the TR-SBT, demonstrating significantly more anchors used in the triple-row SBT (Table 2).
Comparison of clinical outcomes between preoperative and postoperative at 1- and 2-year follow-up.

Data are expressed as mean ± standard deviation.
Paired t test is compared preoperative and follow-up data at 1 year and 2 years, respectively.
SBT suture-bridge technique.
aPaired t test; p < .05, statistically significant.
Comparison of clinical outcomes between conventional SBT and triple-row SBT at 1-year follow-up.

Data are expressed as mean ± standard deviation.
SBT suture-bridge technique;, UCLA Shoulder Rating Scale of the University of California at Los Angeles, ASES American Shoulder and Elbow Surgeons score;, VAS visual analog scale pain score.
aPaired t test; p < .05, statistically significant.
Comparison of clinical outcomes between conventional SBT and triple-row SBT at 2-year follow-up.

Data are expressed as mean ± standard deviation.
SBT suture-bridge technique;, UCLA Shoulder Rating Scale of the University of California at Los Angeles, ASES American Shoulder and Elbow Surgeons score;, VAS visual analog scale pain score.
aPaired t test; p < .05, statistically significant.
The re-tear rate after RCR was 19.2% (5/26 patients) in the conventional SBT group and 11.1% (4/36 patients) in the triple-row SBT group, with no clinical significance (p = .379) (Figure 6). In the conventional SBT group, the retear rate was 15.4% (2/13 patients) in Pattern stage I and 23.1% (3/13 patients) in Pattern stage II; this difference was not significant (p = .635). In the triple-row SBT, the retear rate was 8.3% (2/24) in Patte stage I and 16.7% (2/12) in Patte stage II; this difference was also not significant (p = .468). There was no significant difference in retear rates between conventional SBT and triple-row SBT in patients with Patte stages I and II (p = .523 and .811, respectively). Also, the results of the type I re-tear pattern showed 60.0% (3/5 shoulders) in conventional SBT and 50.0% (2/4 shoulders) in triple-row SBT, respectively. Type II re-tear pattern was 40.0% (2/5 shoulders) in conventional SBT, and 50.0% (2/4 shoulders) in triple-row SBT, respectively ; different rate of re-tear pattern was statistically insignificant (p = .472). The operation time of conventional SBT and triple-row SBT was 55.58 ± 14.65 minutes and 57.08 ± 19.21, respectively, and the p value was 0.739, which was not statistically significant.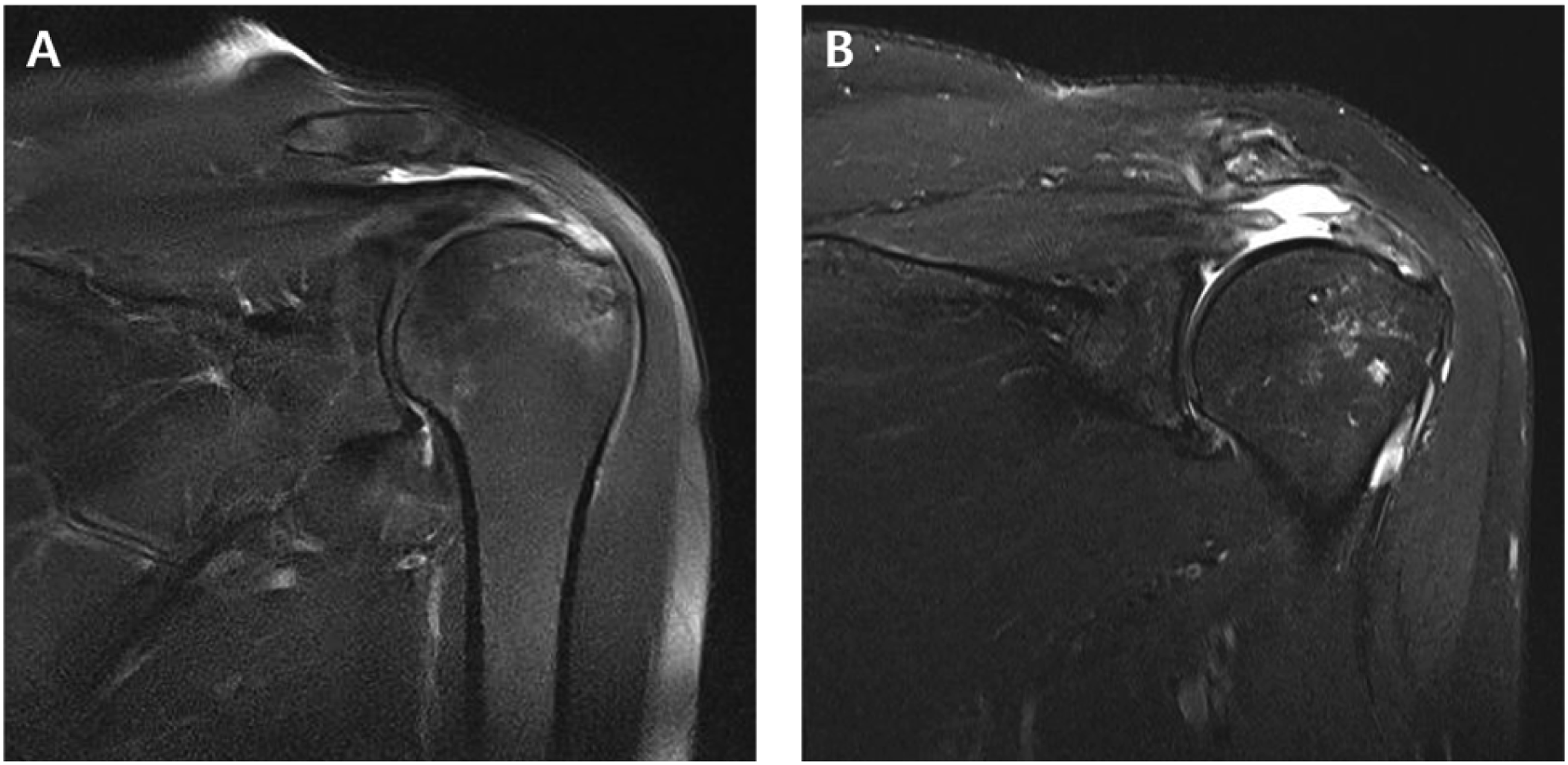
Biomechanical results
A total of 28 models (each of the seven specimens for the conventional SBT and TR-SBT of the vertical and horizontal axes) were properly loaded, and all tests were completed. The majority of the specimen load failures were attributed to anchor pullout, as depicted in Figure 7. Notably, there was a single instance where failure occurred due to the slippage of the allodermal graft through the clamp. When comparing the vertical and horizontal axes, the horizontal axis was higher for all repair techniques. (Table 6) The horizontal axis failure load of conventional SBT and TR-SBT was 360.60 ± 13.29, 456.51 ± 59.35 respectively, and the p value was 0.012 in Mann-Whitney U test, this difference was statistically significant. The vertical axis failure load of conventional SBT and TR-SBT was 327.92 ± 61.83, 412.18 ± 56.00 respectively. The vertical axis failure load was significantly different between the groups (p = .038). When comparing the load tests across the vertical and horizontal axis, the horizontal axis consistently showed higher load values for both techniques. Regarding the failure mode, most specimen load failures were primarily due to the anchor pulling out. Comparison of load failure between conventional SBT and triple-row SBT at horizontal and vertical axis. Data are expressed as mean ± standard deviation. aMann-Whitney U test; p < .05, statistical significance.

Discussion
In this study, we conducted a comprehensive comparison of the clinical, radiological, and biomechanical outcomes between conventional SBT and triple-row SBT. Conventional SBT reportedly improves biomechanical outcomes by increasing footprint coverage, reducing gap formation, and evenly distributing footprint pressure.5,12,13,19 The key feature of conventional SBT is its facility for direct fixation to the footprint via a medial suture knot. In addition, it has been observed that the conventional SBT significantly increases contact pressure between the tendon and the bone footprint when compared to the traditional double-row technique.5,19,20 For this reason, the conventional SBT has low structural failure owing to its biomechanical excellence. 21
However, the conventional SBT or the double row technique can be difficult to obtain anatomic position of the lateral portion in large and highly retracted tendons. 11 Clinical studies have shown that retear rates for rotator cuff repairs using conventional SBT range from 28.9% to 42.4%.22–25 Particularly for larger tears, aligning the lateral portion of the rotator cuff anatomically proves challenging with conventional SBT. This difficulty arises primarily because the medial row suture, performed first, tends to pull and bunch the rotator cuff medially. 11 Consequently, there are concerns regarding the rotator cuff footprint contact area, and using this technique in larger tears can make it difficult for the lateral portion of the rotator cuff to enter the anatomic position. It is therefore hypothesized in this study that by restoring the anatomy and securing fixation, triple-row repair would significantly improve footprint contact area, mechanical strength, and contact pressure compared with conventional SBT and double-row techniques. The triple-row SBT, introducing a middle row of fixation between the standard medial and lateral rows, aims to enhance the rotator cuff footprint contact area by positioning the cuff anatomically before tying the medial anchors. 10 Technically, the middle-row anchor presents several advantages. As discussed above, the middle-row anchor anatomically reduces the cuff and covers the tuberosity. Therefore, it prevents the lateral edge of the rotator cuff from being pulled and bunched medially, making the medial row suture easier. Subsequently, when the medial row anchors were tied against this fixed middle row position, initial compression was achieved. Finally, sutures placed through the lateral row anchors supplied the final compression against the rotator cuff. This is difficult to achieve using conventional SBT, particularly for larger tears that are often retracted. With the conventional SBT, the rotator cuff tended to bunch medially near the anchors. This clearly limited the contact area between the rotator cuff and greater tuberosity. In the double-row technique, the cuff is reduced over the tuberosity; however, there is no final compression by the sutures placed through the lateral row anchors. This also limits the footprint contact area compared to the triple-row technique. Triple-row SBT slightly increased the operating time. Buckup J et al. 11 demonstrated that by reducing the middle-row anchor, the rotator cuff is reduced to a footprint, visualization is much better, and it is easier and faster to tie the medial row. Therefore, it was reported that triple-row SBT did not differ from conventional SBT in terms of operation time. In this study, there was no significant difference in the operation time between the two techniques. From our biomechanical tests, we concluded that the triple-row SBT is more robust. Although direct measurement of contact pressure was not performed, we were able to indirectly assess the structural strength by comparing the intensity of load failure.
This research had some limitations. The first limitation of the biomechanical test is the small sample size. We utilized sawbones paired with allodermal grafts. Theoretically, this approach has the benefit of minimizing the variability in biological properties that often arises when using cadavers. Nevertheless, cadaver-based experiments are generally more representative of true biological behavior. A key challenge was our inability to precisely mimic the natural quality of tendons, their blood supply, the process of fatty degeneration, and the healing dynamics. Moreover, our assessment focused primarily on the strength of load failure rather than evaluating the contact area or pressure between the tendon and bone. This approach rendered our biomechanical experiment somewhat indirect. Consequently, to bridge these gaps and provide a more comprehensive understanding, both biomechanical experiments and clinical studies were undertaken. These combined efforts aimed to provide a more holistic view and address the shortcomings inherent in the biomechanical testing alone.
In clinical aspects, this is a retrospective analysis of the number of cases that are not the same and the number of cases is not the same. This was a retrospective analysis in which the number of patients was not the same, and the number of cases was small. Furthermore, not all patients underwent MRI during their postoperative radiological assessment. MRI is considered the most accurate method for evaluating tendon integrity. In contrast, the sensitivity and specificity of ultrasound (US) examinations in determining post-surgical rotator cuff integrity have been reported to be 91% and 86%, respectively, with an accuracy of 89%. 26 However, based on these findings, ultrasound was utilized in cases where MRI was not feasible. Another limitation of this study was the variance in the number of medial and middle row anchors used in the two techniques being compared. In addition, detailed classifications of rotator cuff tear types and tendon quality—such as preoperative muscle atrophy—were not evaluated. These factors may have influenced clinical outcomes and should be addressed in future research. To address these issues and enhance the validity of the findings, there is a need for prospective randomized studies. Such studies should ideally use an equal number of anchors and involve similar-sized randomized controlled trials to ensure more balanced and reliable outcomes.
In conclusion, both triple-row and conventional SBT exhibited favorable results in short-term follow-up by comparing the UCLA, ASES, Constant, and VAS scores of medium-to-large full-thickness RCTs. Triple-row SBT is an appropriate treatment option with favorable clinical outcomes. Moreover, triple-row SBT was more superior than the conventional SBT in terms of the biomechanical properties. Triple-row SBT reduced the retear rate compared to conventional SBT, although this difference was not statistically significant.
Footnotes
Author contribution
All the athors have been actively involved in the planning and enactment of the study and have also assisted with the preparation of the submitted article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the National Research Foundation of Korea (NRF) grants funded by the Ministry of Science and ICT (MSIT) (No. NRF-2018R1A5A1025224), and supported by the Chungnam National University Hospital Research Fund, 2022.
Ethical statement
Data Availability Statement
Data is available on an as-requested basis. Majority of the data has already been provided in the table of the manuscript.