
Abstract
Background
Distal chevron osteotomy is a common procedure for hallux valgus. Alteration of the osteotomy axis and angle can result in excessive change in length of the first metatarsal and hence the increased risk of transfer metatarsalgia. However, many of the Chevron osteotomies were performed freehand without objective guidance.
Method
Two surgeons with different experience levels (Resident trainee, consultant) using two techniques (freehand or with cutting guide) to perform 15 distal chevron osteotomies on 3D-printed identical first metatarsal sawbone models. The medial cutting angle and lateral exit angle and their difference were analysed. The time taken for each osteotomy was also recorded.
Results
The use of cutting guide brought the medial angle significantly closer to the desired angle of 60° (as described by Austin) for both surgeons, regardless of experience. The lateral angle was significantly closer to 60° in the consultant subgroup.
Conclusion
The study demonstrated that the cutting guide improves accuracy in the osteotomy angle of distal Chevron osteotomy in hallux valgus surgery, regardless of level of experience of the surgeon. Precise osteotomy angles are critical for optimising hallux valgus deformity correction in clinical practice. The cutting guide reduces inter-surgeon variability, enabling less experienced surgeons to achieve reliable results. By standardising the technique, it enhances procedural consistency. While these findings suggest improved reliability for hallux valgus correction, further clinical studies are required to evaluate the direct impact on patient outcomes.
Keywords
Introduction
Hallux valgus is one of the most common foot and ankle problems. A recent systematic review and meta-analysis estimated the overall global prevalence of hallux valgus at 19%, with rates increasing with age to 22.7% in the elderly population (age ≥60) and a female predominance (23.7% compared with 11.4% in males). 1 Over 100 surgical procedures for hallux valgus have been described. There has been an increase in publications on hallux valgus surgeries in the past two decades. 2 Commonly performed osteotomies include proximal and distal Chevron osteotomy, proximal crescentic osteotomy, scarf diaphyseal osteotomy. These were usually performed together with soft tissue procedures like McBride procedure. 3
Among the numerous hallux valgus procedures, the distal Chevron osteotomy is one of the most commonly performed procedures. 4 The procedure involves making a V-shaped cut in the first metatarsal head. The bone is then displaced laterally by one-fourth to half of its width, correcting the intermetatarsal angle. The protruding portion at the medial aspect of the first metatarsal is then rounded off. 3
Three-dimensional (3D) printing, also known as additive manufacturing, is an emerging technology that has the potential to produce a wide spectrum of products in the medical field. This revolutionising technology has the advantage of creating parts that are tailored to our patients by importing the patient’s medical imaging as a 3D digital model. After years of development, 3D-printed technology has now been widely applied in different fields in orthopaedics.5,6 For example, the use of 3D-printed anatomic models for surgical planning, custom-made prosthetics and orthopaedics for better fit and patient comfort, patient-specific surgical guides for orthopaedics procedures, etc.7,8 However, despite its extensive application in orthopaedics and numerous benefits, there are currently minimal reports on the use of 3D-printing technology on osteotomy guides for distal Chevron osteotomy for hallux valgus.
Although a sixty-degree bone cut in chevron osteotomy may not be the most optimal angle for stability of the osteotomy, it was the first described angle in the osteotomy design. Regardless of what the most stable angle for the osteotomy is, performing an accurate and consistent osteotomy is one of the important factors in achieving a reliable clinical outcome for the hallux valgus reconstruction. Alteration of the osteotomy angle can result in excessive change in the length of the metatarsal and hence the risk of transfer metatarsalgia. 9 Despite this factor, many of the Chevron osteotomies were performed freehand or with a guidewire. A recent study by a group of medical students and junior residents training in foot and ankle surgeries revealed that there was more divergence between the medial and lateral angles of the distal chevron osteotomies as compared with the experienced podiatric physician counterparts. With the help of a well-designed cutting guide, more consistent osteotomies were obtained with only mild differences between the medial and lateral angles. 10
Materials and methods
This study was approved by the cluster research ethics committee commencement of the study. 60 identical sawbone models were 3D-printed using one patient’s CT image of the foot as the blueprint. Four groups of sawbone cuts were designed, namely, two doctors of different levels of experience (a second-year orthopaedic resident trainee and a foot and ankle consultant surgeon) would perform distal Chevron osteotomy on sawbones either by freehand or with the help of a 3D-printed osteotomy cutting guide. Each doctor performed 15 osteotomies with each technique.
The cutting guide used in the study was designed de novo with our colleagues in the Department of Prosthetics & Orthotics (P&O) and was produced by 3D-printing technique with thermoplastic ABS-M30i. The cutting guide was a one-piece design of 5 mm in thickness. It comprised three regions. The base plate was oval-shaped containing two smooth round holes. The first one was seated at the upper part and close to the centre of the base plate, which was designed for the passage of a 2.0 mm K-wire angulated posteriorly. The second hole was at the inferior position of the base plate angulated anteriorly, allowing the passage of a 1.4 mm K-wire. The tracts of the two holes were divergent from each other by 30° to enhance the stability of anchorage of the cutting guide to the first metatarsal head. The second component of the cutting guide was a long posterior limb which contained a slot for the more horizontal cut of the chevron osteotomy. At the proximal end of the cutting slot, there was a hole that allowed the passage of a 1.4 mm K-wire. The hole indicated the exit of the horizontal bone cut at the first metatarsal shaft. The third component of the cutting guide was a short superior limb that held two cutting slots, one for the conventional V-shaped cut of chevron osteotomy, angulated 60° to the horizontal limb. The other cutting slot was 2 mm posterior to the original one and angulated at 10° to it, to accommodate the possible need of a biplanar chevron osteotomy. The cutting guide was a 3-dimensional structure with the long limb angulated at 15° to the base plate in the sagittal plane to accommodate the contour of the metatarsal head and neck region after cheilectomy. It was this angulation that made the production of left-sided and right-sided cutting guides necessary (Figures 1, 2, 3 and 4). Design for the cutting guide. Top view of cutting guide. Front view of cutting guide. Bottom view of cutting guide.



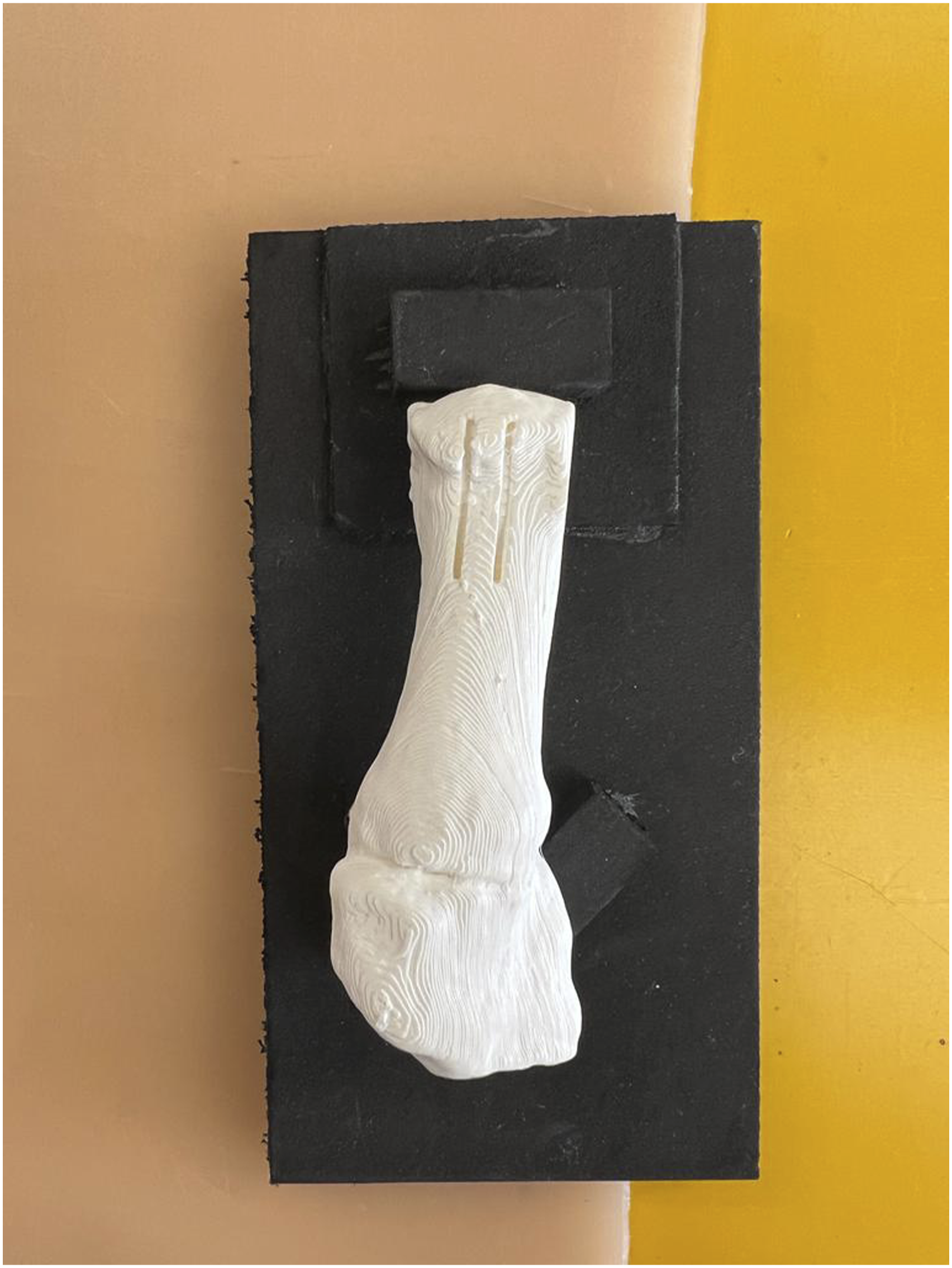
A set of identical medial cuneiform together with first metatarsal sawbones with pre-cut medial cheilectomy of the metatarsal head were 3D-printed. The apex of the osteotomy was marked to minimise variation among each osteotomy. For the freehand group, the apex mark was the point of reference for the osteotomy by freehand. For the cutting guide group, a 2.0 mm K-wire was inserted through the apex slot of the cutting jig. Another 1.4 mm K-wire was inserted into the lower K-wire slot to secure the cutting jig. The bone cuts were made by inserting the oscillating saw along the designated slot. The small gap between the cutting jig slots was then completed by joining the two bone cuts with the oscillating saw. The first metatarsal head was then laterally shifted by 5 mm. The osteotomy was then fixed with a 1.4 mm K-wire from superior to inferior and proximal to distal (Figures 5, 6, 7 and 8). Sawbone used in study. Sawbone with cutting guide overlying. Top view of the sawbone. Top view of sawbone with cutting guide overlying.


To minimise the effect of learning, each doctor was assigned to perform an osteotomy either freehand or with the cutting guide by random order. The medial and lateral angles of the osteotomies were measured with a protractor by a blinded individual investigator who was not present at the time of sawbone cutting and was unaware of the technique or surgeon identity for each sawbone. The time required for each osteotomy defined as the time from creating the first osteotomy cut to the time completing the K-wire fixation, was also recorded. Any complications during the osteotomies were also recorded. All data were unblinded and sorted into groups. Statistical analysis was performed with SPSS version 26.0 (International Business Machines Corporation, Armonk, NY, USA). To compare groups for significant differences, a two-sample unpaired t test was performed. Significance was defined as p < .05.
Results
Overall analysis including both cuts made by trainee and consultant
Overall analysis including both cuts made by trainee and consultant.

Bold indicate statistically significant results.
Subgroup analysis for cuts made by trainee
Subgroup analysis for cuts made by trainee.

Bold indicate statistically significant results.
Subgroup analysis for cuts made by consultant
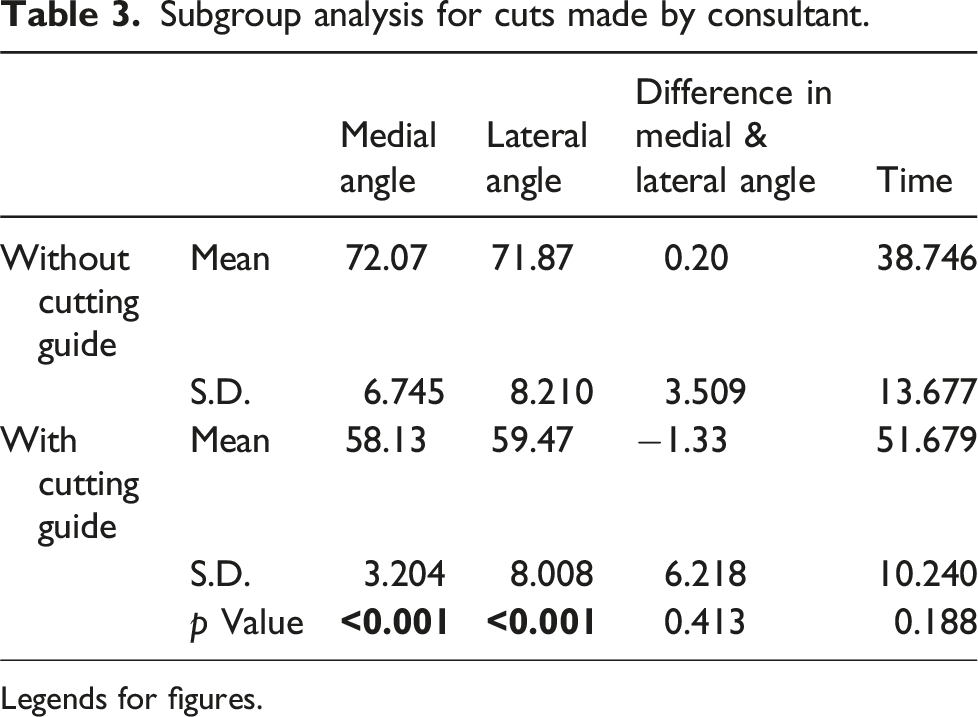
Subgroup analysis for cuts made by consultant.
Legends for figures.
Discussion
The objective of the study was to evaluate whether the use of a 3D-printed cutting guide improves the accuracy of the osteotomy angle in distal Chevron osteotomy. The results of this study indicated that the use of the cutting guide brought the medial angle significantly closer to the desired angle of 60°, which was the osteotomy angle described by Austin in his original paper, regardless of the level of experience of the operating surgeon. The lateral angle was also significantly closer to 60° in the consultant subgroup and in the overall analysis.
Although the time taken for the cutting guide group was statistically significantly longer, the mean time difference of 13 seconds (consultant subgroup) to 23 seconds (trainee subgroup) is likely clinically insignificant in relation to the entire operative time for the hallux valgus surgery. The advantage of a more accurate cut also outweighed the disadvantage of the slightly longer time required. An accurate osteotomy angle is crucial for a successful clinical outcome in hallux valgus reconstruction. Deviation of the osteotomy angle may lead to an unwanted change in the length of the first metatarsal. Shortening of the first metatarsal is often thought to be one of the major causes of transfer metatarsalgia. Nakagawa et al. reported that the preservation of relative metatarsal length during first metatarsal osteotomy was important in preventing postoperative metatarsalgia. 9 While the optimal osteotomy angle of the distal Chevron osteotomy is still debatable, with a wide range of osteotomy angles being advocated, the results of this study demonstrated that the use of a cutting guide improves the accuracy of the osteotomy angle to the desired angle planned pre-operatively. This principle holds true regardless of the specific angle chosen by the surgeon. This 3D-printed cutting guide surgical technique may help reduce unwanted changes in the length of the first metatarsal and thereby reduce uncertainties in the clinical outcome.
Furthermore, this study demonstrated that the cutting guide enables surgeons with varying experience levels to achieve improved accuracy of the osteotomy cut as compared with the freehand technique. This finding is also consistent with a growing body of evidence on the use of 3D-printed cutting guides, which suggests the use of such guidance systems can improve the operative time and blood loss. 11 A recent scoping review with a pooled total of 932 participants showed that the operating time (p < .001), blood loss (p < .001), fluoroscopy times (p < .001), bone union time (p < .001), pain (p = .040), accuracy (p < .001), and functional scores (p < .001) were significantly improved with 3D printing compared to the control group with no significant increase in complications. 12
The enhanced accuracy would also reduce inter-surgeon variability. By standardising the osteotomy technique, the cutting guide also appeared to facilitate reliable performance among less experienced surgeons, potentially reducing the duration of the learning curve of the procedure. While the findings of the study indicate that cutting guides could contribute to more reproducible surgical outcomes, direct evidence linking improved accuracy in sawbone models to enhanced clinical outcomes, such as better deformity correction, lower rates of complications, or improved patient satisfaction, remains to be established with future studies. Nevertheless, the increased accuracy of the osteotomy angle lays a compelling foundation for future clinical studies to explore whether these technical advantages translate to better clinical outcomes.
The major limitation of the study was the sawbone model. This was an ex vivo study involving the use of sawbones. While this model was necessary to isolate the effect of the guide on the technical execution of the osteotomy by eliminating confounding patient-specific variables like bone density and soft tissue constraints, it has inherent differences from clinical practice. Despite the great effort to create a realistic sawbone, differences in the texture of the materials still exist when compared to the bone of patients. It was observed during the study that some of the sawbones slightly melted under the heat generated during the simulation of bone cuts, potentially affecting the time recorded for osteotomy. Furthermore, hallux valgus reconstruction in patients involves soft tissue dissection while no soft tissue handling was needed in sawbone cuts.
Conclusion
The results of the study demonstrated that the use of a 3D-printed cutting guide improves accuracy in the osteotomy angle of distal Chevron osteotomy in hallux valgus surgery, regardless of the level of experience of the surgeon. In clinical practice, precise osteotomy angles are critical for optimising the correction of hallux valgus deformity. Furthermore, the study showed that the cutting guide enables surgeons with different experience levels to achieve improved accuracy. By standardising the technique, the cutting guide enables less experienced surgeons to perform the procedure with greater reliability. While these findings suggest promising implications for improving the reliability of hallux valgus correction with the use of a 3D-printed cutting guide, further clinical studies are required to evaluate the direct impact on patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.