
Abstract
Purpose
The aim is to explore the impact of rotator cuff repair on sleep quality and its correlation with postoperative pain and recovery.
Methods
A prospective cohort study from December 2022 to May 2023 was conducted on 28 patients undergoing arthroscopic rotator cuff repair. Pre- and postoperative sleep quality was assessed using the Korean version of the Pittsburgh Sleep Quality Index (K-PSQI), and pain was measured using the pain visual analog scale (pVAS). Sleep duration was monitored using Fitbit Inspire 2 trackers post-surgery. Statistical analyses were conducted to evaluate the relationship between sleep quality, pain, and postoperative recovery.
Results
The mean preoperative PSQI score (9.5 ± 6.0) indicated sleep disturbances, with elevations in sleep latency and disturbances. Six weeks post-surgery, PSQI decreased significantly to 6.4 ± 3.3 (p = .03), with marked improvements in sleep quality and efficiency. Mean pVAS scores consistently declined post-operation, while sleep duration increased. A statistically significant correlation (p < .05) existed between pVAS score reduction and sleep duration increment. Additionally, preoperative PSQI scores significantly correlated with ‘Daily pVAS decrease’ and ‘Daily sleep duration increase’.
Conclusions
We demonstrate that rotator cuff repair leads to improvements in sleep quality and reductions in pain. However, the persistently high postoperative PSQI scores suggest that sleep disturbances may not be entirely resolved by surgery alone. These findings highlight the need for comprehensive perioperative care in rotator cuff tear patients, incorporating both surgical and non-surgical strategies to manage sleep disturbances and enhance overall patient outcomes.
Level of evidence
Level III, Prospective cohort study.
Keywords
Introduction
A rotator cuff tear is a predominant etiology for outpatient consultations attributable to shoulder pain.1–5 While its direct effects on shoulder discomfort and functional impairment are well-documented, there is less emphasis on its correlation with sleep disruptions.6–10 Sleep disturbances not only impact daily activities and overall quality of life, but also have significant effects on psychological, somatic, and physiological health—potentially intensifying pain sensitivity and guiding surgical treatment decisions.11,12 Previous literature indicates a potential cyclical relationship between sleep disturbance and pain, suggesting that disrupted sleep can amplify sensitivity to pain, while persistent shoulder pain may further exacerbate sleep disorders.8,13
Following arthroscopic repair of the rotator cuff, patients commonly experience a significant improvement in shoulder pain and joint function.14–16 However, despite an initial postoperative reduction in sleep disturbances, long-term studies have indicated a tendency for these symptoms to revert to baseline levels or even worsen over time.7,8 Some studies suggest recurrence of sleep disturbance and its relationship with post-operative analgesics and opioids, 7 while others suggest that early postoperative pain might be the predominant factor causing sleep disturbances during initial recovery periods.6,9,11,12 Most recent studies have shown that postoperative sleep disturbances often persist due to residual pain and positional discomfort.17,18
Psychological factors, including anxiety and depression, further complicate the resolution of sleep disturbances; however, despite these complexities, sleep disturbance remains relatively under-addressed in postoperative analgesic management following rotator cuff repair.11,19,20 Effective management of these sleep disturbances requires an in-depth understanding of specific sleep disorder pathologies, primarily differentiated into “initiation disorder,” characterized by difficulty in sleep onset, and “maintenance disorder,” characterized by interruptions in sustained sleep.21,22 Given the persistent shoulder pain and associated discomfort from rotator cuff injuries, particularly when adjunctive external support such as shoulder slings are applied, it’s hypothesized that patients may suffer from both sleep disorder types at the same time.
To better clarify these gaps in understanding of shoulder pain and sleep disturbance, this study investigated how sleep disturbances manifest in patients with rotator cuff tears and how these disturbances change in short-term after surgical treatment. We hypothesized that (1) as the postoperative pain visual analog scale (pVAS) decrease from its pre-surgical values after surgery, the intensity of sleep disturbances will also decrease, and sleep duration will increase, and (2) patients with severe preoperative sleep disturbances will show slower increases in sleep duration and slower decreases in pain after surgery.
Materials and methods
Study design
We performed a prospective cohort study, conducted from December 2022 to May 2023. This study included patients admitted to and underwent arthroscopic rotator cuff repair in single medical center (Eulji medical center, Daejeon, Republic of Korea). Patients who met the following conditions, as well as the predefined inclusion and exclusion criteria, were considered eligible for this study. A total of 28 patients were included.
The patients included in this study have undergone general anesthesia for surgery and used patient controlled suprascapular nerve block using catheter. Patients were then admitted for an average 4 days post-surgery, and managed their pain using non-opioid oral analgesics (NSAIDs and tramadol/paracetamol) during admission period.
The inclusion criteria for this study were (1) adults age between 25 and 80 years; (2) full thickness rotator cuff tear diagnosed with MRI image; and (3) undergoing arthroscopic rotator cuff repair. The exclusion criteria for this study were (1) patients with irreparable cuff tear and (2) who needed other procedures (e.g., patch augmentation, labral repair). The institutional review board approvals were obtained (EMC IRB No.2022-10-002-002), and informed consent was obtained from every participant.
Variables & outcome measures
Patient’s past medical history, body mass index (BMI), and smoking/alcohol history was recorded. Rotator cuff tear site, size and grade was measured with MRI image and formal reading. MRI images were reviewed and cross-checked directly by the authors of this study using the INFINITT PACS M6 system. During arthroscopic rotator cuff repair, cuff tear size and retraction level, procedures done during surgery were checked and recorded.
Outcome measures
The pVAS scores were assessed based on the patients’ self-reported pain levels in the morning during hospitalization, by designated orthopedic resident and researching nurse. During the outpatient follow-up period, pain scores were recorded using the same time-specific inquiry to ensure consistency in data collection.
For evaluating sleep quality and presence of sleep disorder, the Korean version of the Pittsburgh sleep quality index (K-PSQI) questionnaire was administered. The K-PSQI assesses seven aspects of sleep, and collectively offer a comprehensive view of the patients’ sleep patterns and disturbances: subjective sleep quality (patient’s perception of their sleep quality), sleep latency (time taken to fall asleep), sleep duration (actual amount of sleep), habitual sleep efficiency (percentage of time in bed spent sleeping), sleep disturbances (factors disrupting sleep), use of sleeping medication, and daytime dysfunction (impact of sleep quality on daily activities). The total PSQI score is calculated by summing the scores from the seven components, and a score of 5 or higher is considered indicative of sleep disturbance or disorder.
23
These outcome measures were collected by chief resident of our center. The assessments were also repeated during outpatient visits at 3 weeks and 6 weeks after discharge (Figure 1). Protocol of patient treatment and data collection.
For the assessment of sleep duration and related changes, this study utilized sleep tracker “Fitbit Inspire 2” (Fitbit Inc., San Francisco, CA, USA; https://www.fitbit.com/) which records sleep duration based on changes in heart rate during sleep. Study by Lee et al. 24 and several other studies compared Fitbit’s sleep tracker to sleep actigraphy and polysomnography and showed that Fitbit’s results could be used in medical research alternatives, at a lower cost.
Patients wore the sleep tracker from the day of surgery until discharge from hospital stay, and to account for measurement errors or device malfunctions, a sleep duration questionnaire was simultaneously conducted. Using this approach, the research team recorded the actual sleep duration (Figure 2) and the next morning’s pVAS scores daily for comparison. Example of Fitbit Inspire 2’s sleep-tracking result. One of the sleep duration results for a patient who participated in the study. It shows the total sleep time, the start and wake times, and the number of awakenings during sleep, along with a rough indication of the sleep stages. The sleep stages were not used in the analysis of the results of this study.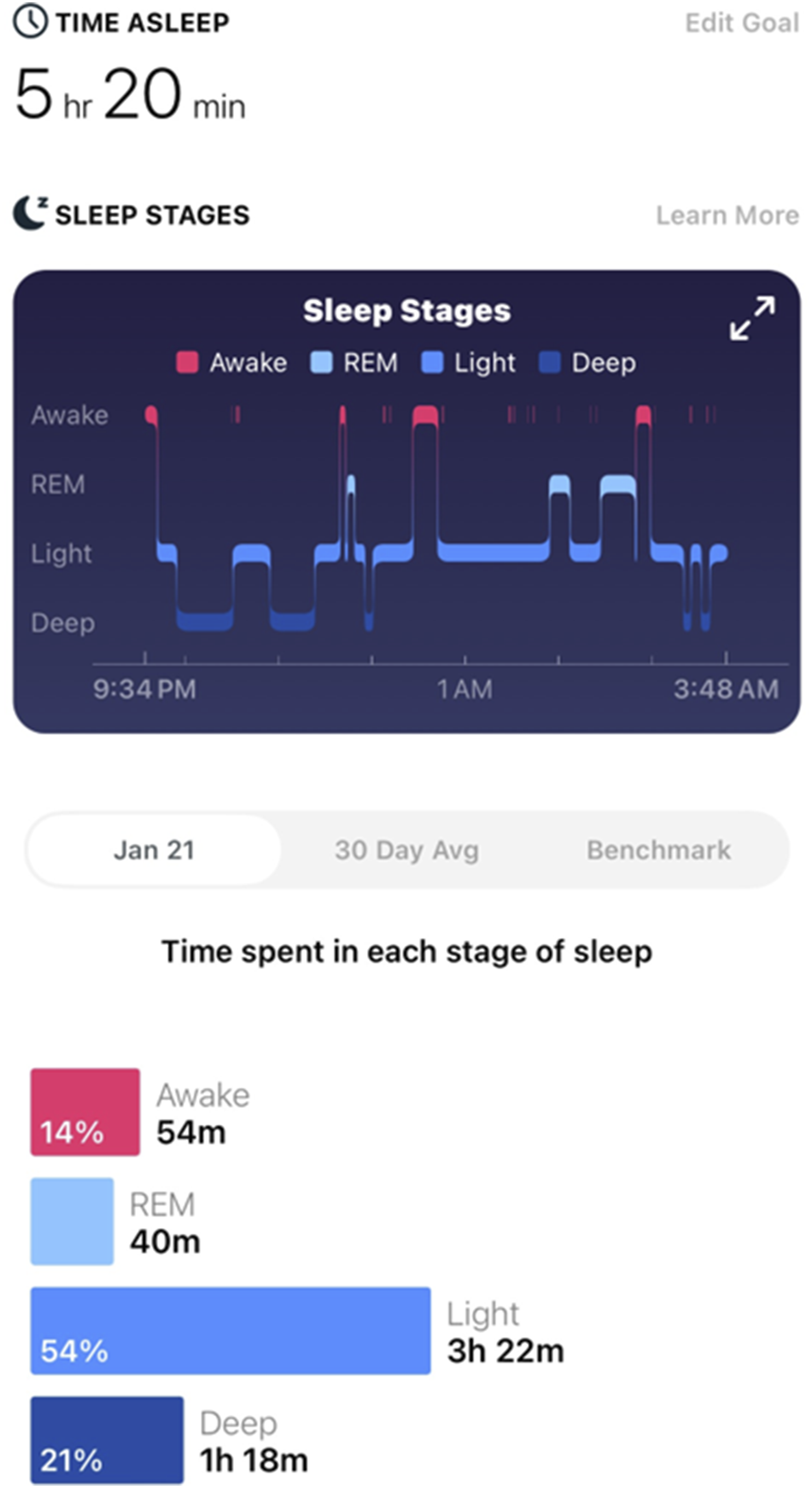
PVAS score was selected as this study’s primary outcome, with its minimal clinically important difference (MCID) of 1.5 suggested from other study. 25 Although sleep quality and its characteristics were our main subject, PSQI score was selected as secondary outcome measure, as it reflects previous month’s sleep quality.
Statistical analysis
Sample size for this study was calculated using the statistical method suggested by Lee et al., 26 using standard deviation, MCID of pVAS, standard deviation of pVAS from population of our study, and desired power of 80%. Calculated sample size was 25, but regarding 10% drop-out rate, our study needed 28 patients for statistically significant results.
Descriptive statistical analysis was performed on the collected data for study population demographics. For observing change in sleep disturbance level, we compared PSQI before and after operation, paired t test was done. Correlation analyses also was used to examine the relationship between the reduction in daily pVAS scores and the increase in daily sleep duration. Additionally, the correlations between the pre-operative PSQI score and the decrease in pVAS, as well as the increase in sleep duration was investigated. Multivariate regression analyses were performed to control for potential confounding factors such as age, BMI, etc. All statistical analyses were performed by authors of this study, with significance levels set at p < .05 and using IBM statistics SPSS version 28.
Results
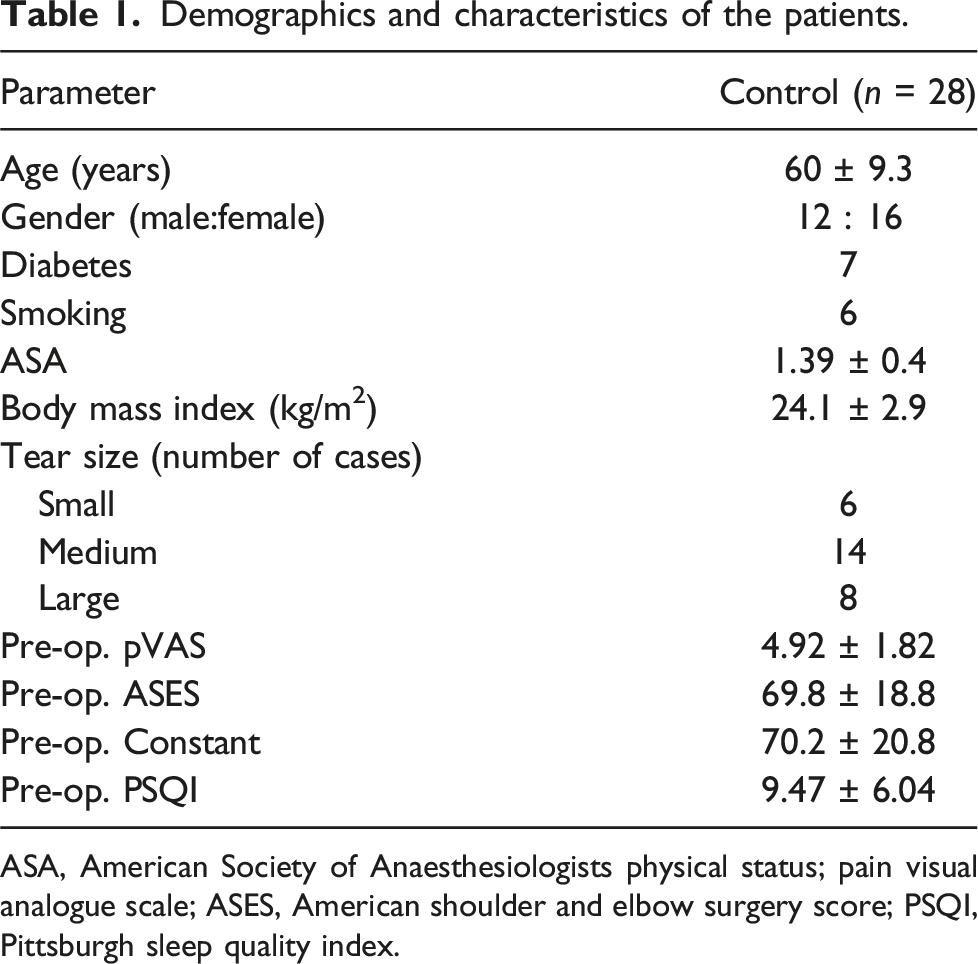
Our study recruited a prospective cohort (Figure 3) and data from a total of 28 patients were obtained. The mean preoperative PSQI score was 9.5 ± 6.0, significantly higher than the cutoff of 5 for defining sleep disorders, with prevalence of sleep disorder of 71% (20 of 28, Table 1). High scores were observed in both sleep latency and sleep disturbance (Table 2). No patients included in the study have other causes for sleep disturbance such as sleep apnea, urinary frequency, etc. Inclusion & Exclusion criteria and design of prospective cohort. Demographics and characteristics of the patients. ASA, American Society of Anaesthesiologists physical status; pain visual analogue scale; ASES, American shoulder and elbow surgery score; PSQI, Pittsburgh sleep quality index. Comparison of pre-operative and post-operative PSQI. SD, standard deviation; PSQI, Pittsburgh sleep quality index.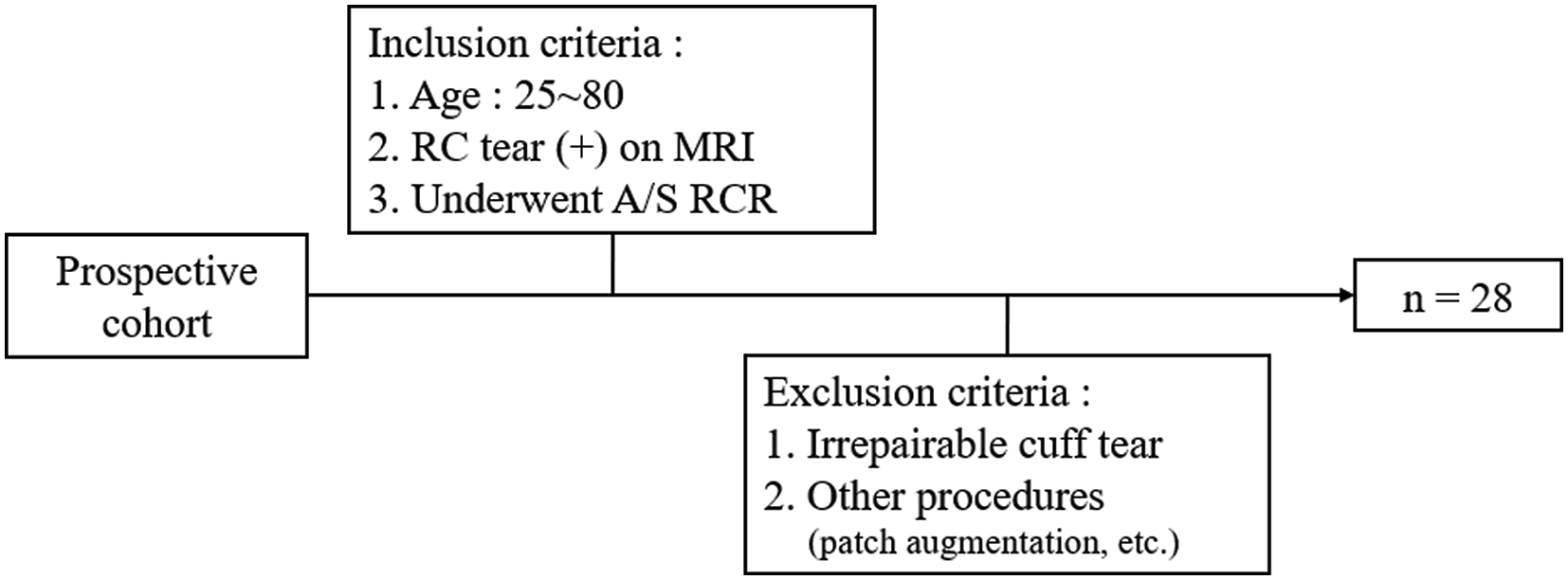

At the 6-week follow-up after surgery, the PSQI score significantly decreased to 6.4 ± 3.3 (p = .03) compared to the preoperative score. Specifically, statistically significant reductions (p = .01) were observed in the Sleep Quality and Efficiency components (Table 2).
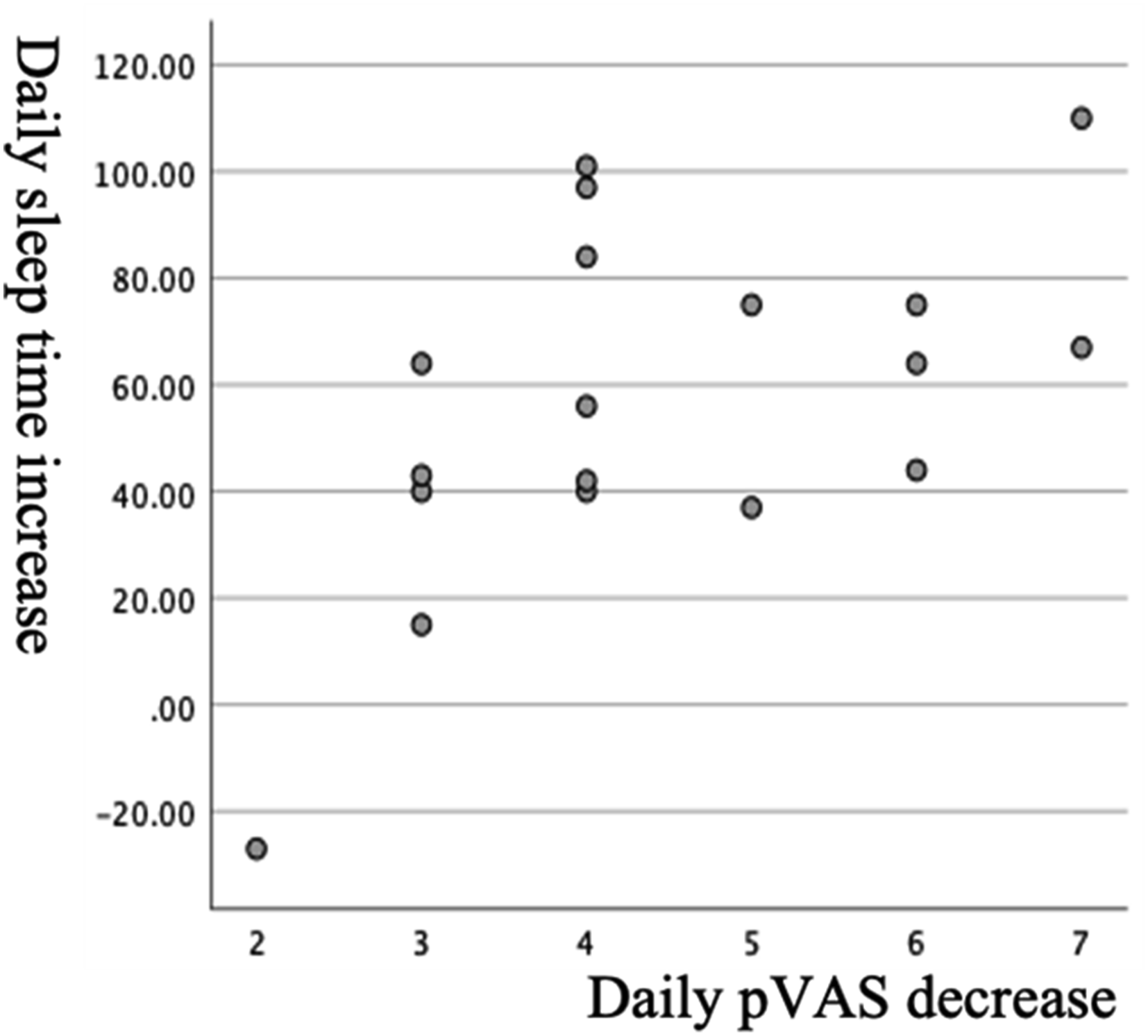
The mean pVAS scores progressively decreased during the postoperative hospital stay, with scores of 8.3 ± 1.6 (POD 1), 6.4 ± 1.7 (POD 2), 4.0 ± 2.0 (POD 3), and 1.9 ± 1.6 (POD 4) from the morning after surgery to the fourth morning after surgery, respectively (Figure 4). Conversely, sleep duration recorded with sleep tracker showed an increasing trend, with 4.2 ± 1.0, 4.7 ± 1.7, 5.3 ± 1.4, and 6.3 ± 1.5 hours from the night of surgery to the third night after surgery, respectively. A correlation analysis revealed a statistically significant relationship (p = .02) between the extent of pVAS decrease and the increase in sleep duration (Figure 5). Preoperative PSQI scores exhibited a significant negative correlation with ‘Daily pVAS decrease’ and ‘Daily sleep duration increase' (Figure 6). Daily sleep duration and pVAS change after surgical treatment. Correlation between daily pVAS and sleep duration change. The X-axis represents the decrease in pVAS, while the Y-axis represents the increase in sleep duration. Positive correlation is shown as the decrease in pVAS becomes larger, the increase in sleep duration also becomes more significant. Regression analyses of daily pVAS and sleep duration with pre-operative PSQI. The X-axis represents the preoperative PSQI, while the Y-axis represents the daily pVAS decrease and the daily sleep time increase, respectively. Each graph shows a negative correlation between the preoperative PSQI and the respective values. This indicates that patients with severe preoperative sleep disturbances experience slower decreases in pain and slower increases in sleep duration after surgery.

Correlation analyses did not reveal any statistically significant correlation between collected data of PSQI, sleep time after surgery and comorbidities, cuff tear size.
Discussion
In our research, we noted a significant impairment in preoperative sleep quality of rotator cuff tear patients as evaluated through PSQI scores, surpassing the threshold indicative of sleep disorders. At the 6-week postoperative assessment, we observed a notable improvement in sleep, particularly in the aspects of sleep quality and efficiency. Directly after surgery, the pain scores (pVAS) progressively decreased from 8.3 to 1.9 over the course of 4 days, while daily sleep duration increased. Additionally, we identified a meaningful correlation between the reduction in pain scores and the extension of sleep duration. It’s worth noting that preoperative PSQI scores exhibited a negative correlation with both ‘daily pVAS decrease' and ‘daily sleep duration increase,’ highlighting the significance of addressing sleep-related concerns in perioperative care.
The results of our study showed the occurrence of sleep disturbance in RCT patients higher than general population, which was in line with results of other studies.1,9,13,14,27 Recent literature reported pre-operative PSQI to be three to six times higher than general population.28,29 Also, our results showed high scores in sleep latency and disturbance component of PSQI, which can be interpreted as RCT patients having both sleep initiation and maintenance disorder at the same time. 30
Negative correlation between higher pre-operative PSQI score and the degree of postoperative pain decrease or sleep duration increase was also aligned with recent study by Wu et al, arguing that those with poorer preoperative sleep quality experienced more pain a month post-surgery, and suggested that better management of sleep disorders prior to surgery could enhance pain outcomes postoperatively 28 . This supports our suggestion that addressing sleep quality in RCT patients is crucial, not only in the surgical context but also when managing conservative treatments over extended periods, since many patients often spend a lot of time on nonsurgical treatments before considering an operation.
Other studies have also reported reductions in PSQI after rotator cuff repair. Cho et al. 31 and Glogovac et al. 32 noted decreases in PSQI from 6.6 to 5.8 and from 9.50 to 7.10, respectively at 6 months post-surgery, indicating that sleep disturbances persist to some extent even after a long period. Similarly, systematic reviews examining the relationship between sleep disorders and RCT have shown that sleep disturbances persist to some extent at 6 months, and even up to 12 months post-surgery. In this study, the PSQI measured at the 6-week post-operative follow-up showed a statistically significant decrease but remained higher than the threshold for sleep disturbances (PSQI >5). Specifically, while improvements were noted in sleep quality and efficiency, high values persisted in sleep latency, duration, disturbance, and daytime dysfunction (Table 2). This suggests that at 6 weeks post-surgery, factors such as pain at the surgical site and discomfort from wearing a brace may still be contributing to longer sleep latency, frequent awakenings, and insufficient total sleep time. 15 Considering the persistence of long-term sleep disturbances reported in other studies and the lack of reduction in latency and disturbance in our study, further research is needed to understand these issues better. Additionally, it underscores the necessity for the treatment of sleep disturbances along with surgical treatment and pain control, which the authors of this paper plan to undertake in future studies.
In our study, we only investigated the sleep duration among the sleep result indicators provided by Fitbit. There were about 2-3 cases in this study where sleep duration was not recorded midway. Although we adjusted for these missing values using statistical methods, there might have been minor differences in the results due to this. Furthermore, since the Fitbit device operates using algorithms based on movement and heart rate decrease during sleep, the possibility exists that it was less accurate than polysomnography, which is considered the gold standard in sleep analysis. 17 We could not use the sleep stages and the duration of each stage as shown in Figure 2. While there is still a lack of research on the suitability of these for medical studies in other research, if future additional studies include comparisons of trends in this regard, it might lead to a deeper understanding of post-surgery sleep in patients.
Interestingly, some studies have suggested an association between sleep disturbance and long head of the biceps (LHB) tendinopathy in patients undergoing rotator cuff repair. Kelly et al. 33 demonstrated that sleep disturbance was significantly more common in patients with LHB pathology, suggesting that inflammation and pain originating from the biceps tendon could contribute to the deterioration of sleep quality. Although our study did not specifically assess LHB pathology, its potential impact on postoperative sleep should not be overlooked. Future studies incorporating detailed assessment of biceps involvement may provide further insight into this relationship.
Several limitations need to be acknowledged in this study. First, our study did not compare the results of our cohort with those of the general population regarding key parameters such as the K-PSQI, pVAS, and daily sleep time. Second, although our sample size of 28 patients raises concerns regarding statistical power and potential Type II errors, this limitation was due to strict inclusion criteria and the prospective design over an 8-month period. A larger cohort in future studies will be necessary to validate these findings and improve generalizability. Third, the assessment of sleep duration was limited to the immediate postoperative period (first 4 days), which could be significantly influenced by acute postoperative factors such as surgical pain, brachial plexus block effectiveness, and heightened pain sensitivity. Fourth, the 6-week follow-up period may not be sufficient to fully evaluate long-term sleep recovery. Previous studies, such as by Li et al. 17 and Mozes et al., 18 have shown that sleep disturbances can persist for several months or even longer postoperatively, particularly due to persistent stiffness or ongoing rehabilitation. Future research incorporating extended follow-up intervals (e.g., one, two, and 4 weeks postoperatively) is essential to robustly validate observed correlations. Lastly, we did not explore the relationship between sleep quality and detailed patient and disease characteristics, such as specific rotator cuff tear attributes and muscle composition. Further investigation of these aspects in future studies may provide deeper insights into personalized perioperative management and patient outcomes.
In spite of these limitations, this study has the advantage of demonstrating that pain and sleep recovery during the early post-operative period when pain is most severe, vary depending on the severity of pre-existing sleep disturbances. Additionally, it highlights the potential use of sleep trackers as a cost-effective tool for monitoring sleep health in hospitalized patients.
Conclusion
We found that rotator cuff tear significantly impairs sleep quality, which improves post-surgery. The correlation between decreased pain and increased sleep duration postoperatively indicates the importance of sleep management in RCT treatment. Despite this improvement, the persistently high postoperative PSQI scores suggest that sleep disorders may not be entirely resolved by surgical intervention. This underlines the importance of a comprehensive approach to managing sleep disturbances in RCT patients, which should encompass both surgical and non-surgical treatment strategies to enhance overall patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by Eulji University in 2023.