
Abstract
Purpose
This study compares the clinical outcomes of the Lasso-loop and Jaw-designed suture passer techniques for arthroscopic treatment of chronic lateral ankle instability (CLAI) caused by anterior talofibular ligament (ATFL) injuries. We aimed to assess whether the Jaw-designed technique provides similar outcomes with reduced intraoperative stitch time.
Methods
This retrospective cohort study included 40 patients with CLAI, who underwent arthroscopic ligament repair between February 2019 and February 2022. They were divided into two groups: 20 treated with the Lasso-loop technique and 20 with the Jaw-designed suture passer. Functional outcomes were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) scale, Karlsson Ankle Functional Score (KAFS), Tegner activity scale (TAS), and Visual Analog Scale (VAS) for pain. Intraoperative ligament stitch time was also recorded for both groups.
Results
Both groups showed significant improvement in AOFAS, KAFS, TAS, and VAS scores from preoperative to final follow-up (p < .001). The mean intraoperative ligament stitch time was significantly shorter in the Jaw-designed group (9.1 min) compared to the Lasso-loop group (16.5 min) (p < .001). However, no significant differences in final functional outcomes (AOFAS, KAFS, TAS, and VAS scores) were observed between the two groups (p > .05).
Conclusion
The Jaw-designed suture passer technique for repairing the ATFL in CLAI offers clinical outcomes comparable to the Lasso-loop technique, with the added benefits of a shorter suture time and simpler execution. This technique may be particularly beneficial for novice surgeons and can serve as a reliable alternative to the Lasso-loop suture technique in the arthroscopic repair of CLAI.
Keywords
Introduction
The ankle joint, a crucial weight-bearing structure, is susceptible to sprains during both everyday activities and sports participation. The lateral ankle ligament injury accounts for up to 80% of ankle sprains. The anterior talofibular ligament (ATFL) is the most frequently injured ligament in ankle sprains.1–4 While most patients can regain ankle function with nonoperative treatment following an injury, approximately 30% of patients who do not respond to nonoperative management can develop chronic lateral ankle instability (CLAI).5,6 Surgical intervention becomes the preferred course of action when nonoperative management proves ineffective.
The standard surgical treatment for CLAI involves the Broström operation, emphasizing anatomical restoration of the ATFL, and the Broström-Gould method, which strengthens the stitch of the inferior extensor retinaculum. 7 With the development of minimal invasive techniques, minimally invasive repair surgeries of the ATFL have been performed percutaneously or with arthroscopy. While the Lasso-loop stitch technique is the prevalent choice in arthroscopic repair of ATFL, it poses challenges for novices due to its complexity. 8 Jaw-designed suture passer (Scorpion, Arthrex, Naples, FL) technology is commonly used for rotator cuff tears and has shown excellent clinical results. 9 Guillo and Carvalho et al.10,11 used the Jaw-designed suture passer technique when describing an all-inside endoscopic Broström-Gould method without clinical results.
This study aimed to compare the clinical outcomes between the arthroscopic Lasso-loop and Jaw-designed suture techniques in the treatment of CLAI caused by ATFL injuries. We attempted to determine whether the Jaw-designed suture passer technique could provide sufficient ankle stability and shorten intraoperative ligament stitch time. We hypothesized that both techniques could achieve good clinical outcomes, and the Jaw-designed suture passer technique would accelerate intraoperative ligament stitching.
Materials and methods
The study was carried out in accordance with the World Medical Association Declaration of Helsinki. Fifty-three patients (53 ankles) who underwent the arthroscopic procedure for CLAI between February 2019 and February 2022 were retrospectively analyzed. The inclusion criteria for this study were a preoperative diagnosis of CLAI (based on symptoms of instability, anterior drawer and varus stress tests, and magnetic resonance imaging results), no history of ankle fracture, no neuromuscular disorders, and a failure of nonoperative treatment for a period of at least 3 months.12–14 Thirteen patients (13 ankles) who did not meet the criteria were excluded. This study was approved by the institutional review board of our hospital, and written informed consent was waived by the institutional review board due to the retrospective nature of this study.
Accordingly, the remaining 40 patients (40 ankles) with CLAI were retrospectively assigned into two groups based on the surgical period. From February 2019 to August 2020, the surgeon performed the Lasso-loop technique, and from September 2020 to February 2022, the Jaw-designed suture passer technique was adopted as the preferred method. Thus, group allocation was determined chronologically rather than by patient-specific characteristics or surgeon preference at the time of surgery.
Surgical procedures
All operations were performed by a single foot and ankle surgeon. The procedure was conducted under general anesthesia, with the patient placed in the supine position and the injured ankle slightly off the end of the operating table. The injured ankle was maintained in a neutral position, and a proximal thigh tourniquet was used. Surgical approach used three portals (Figure 1). The first portal (P1) was located 1.0 cm proximal to the ankle joint level and lateral to the tibialis anterior tendon. The second portal (P2) was positioned 1.0 cm distal to the ankle joint level and at the lateral border of the talus, while the third portal (P3) was positioned at the tarsal sinus. Portals (TA tibialis anterior tendon, P1 first portal, P2 second portal, P3 third portal, LM lateral malleolus).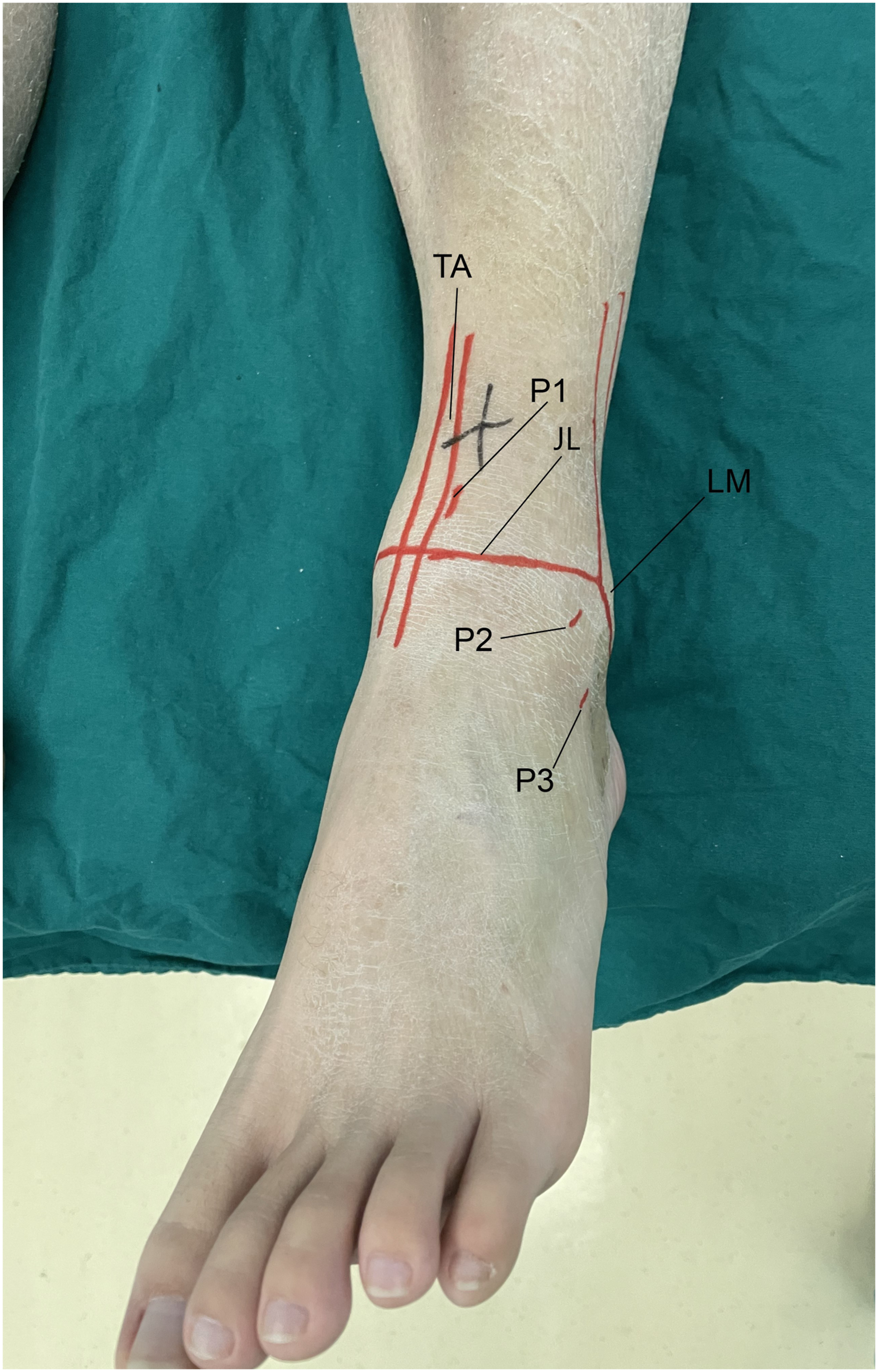
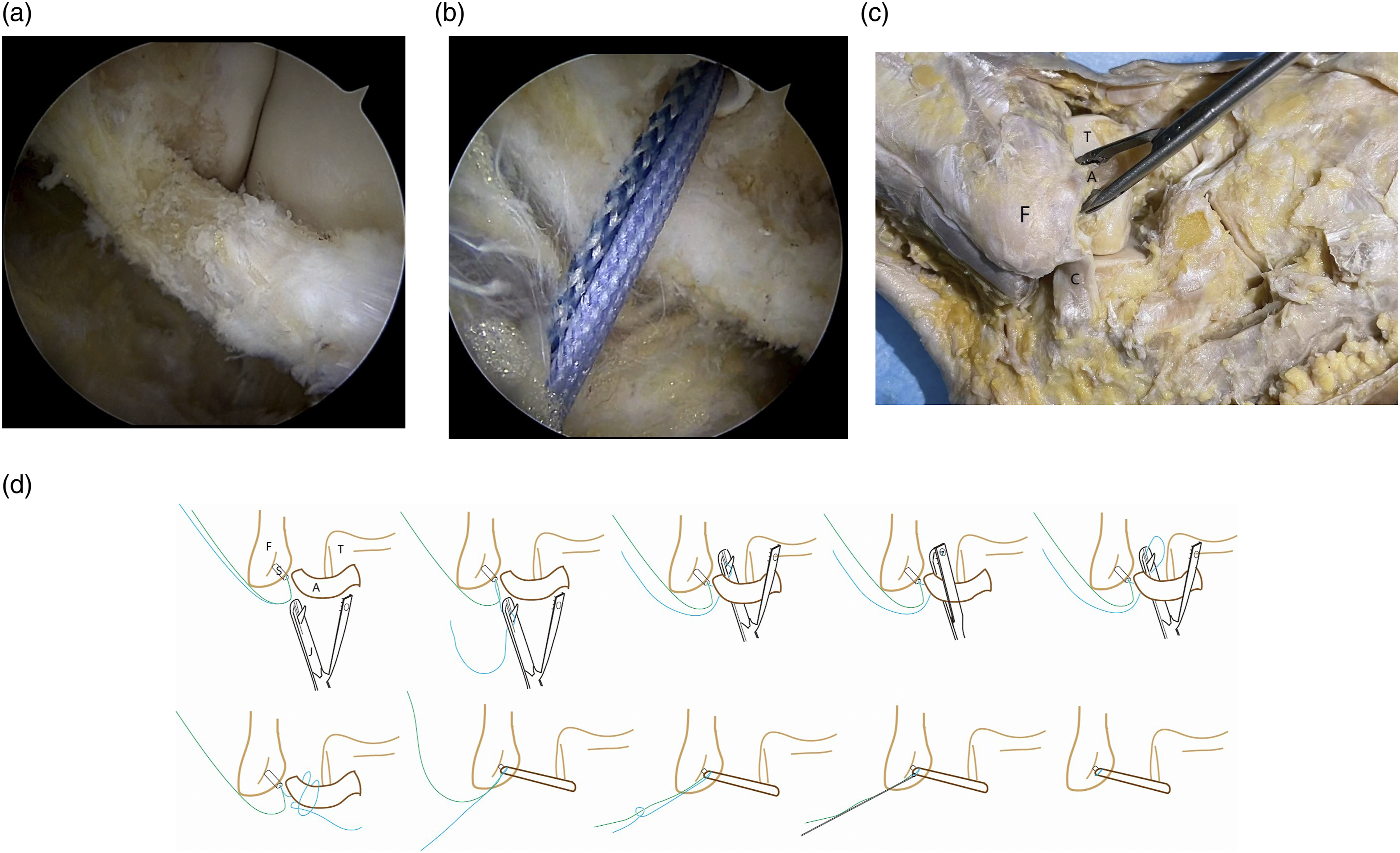
Initially, the P1 portal was set as a viewing portal, and intra-articular synovial debridement was performed through the P2 portal as a working portal. Subsequently, a banana knife was used to expose the ATFL through the P2 portal, and the residual ATFL stump was debrided using an arthroscopic shaver (Figure 2(a)). After identifying the ATFL footprint on the fibula, a 3.0-mm bioabsorbable suture anchor (Smith & Nephew) was introduced into the fibular tunnel (Figure 2(b)). The Lasso-loop and Jaw-designed techniques were then employed separatively to repair the ATFL. 1. Lasso-loop group: The procedure follows the arthroscopic method detailed by Takao (2015).
8
Initially, a 20G needle with a 2-0 PDS (polydioxanone) suture is introduced into the distal ATFL remnant through the P3 portal. The needle is rotated multiple times in one direction and then in the opposite direction, expanding the PDS loop. The loop of the PDS is retrieved through the P3 portal with a grasper, and the 20G needle is then withdrawn. Subsequently, one end of the suture anchor is passed through the loop of PDS. Then, use the PDS loop to thread the mid-portion of the anchor suture through the ATFL, forming a loop of suture in the ATFL. Finally, thread the tail end of the anchor suture through this loop and tighten it. 2. Jaw-designed group: Pass one end of the anchor suture through the Jaw-designed. Then, clamp the Jaw-designed suture (Johnson MEDICAL (CHINA) Ltd) device onto the entire ATFL and withdraw the anchor suture to form a loop. Finally, thread the tail end of the anchor suture through this loop and tighten it. (Figure 2(c) and (d)). The Jaw-designed suture passer technique for repairing the ATFL. (a) Depicts the ATFL damage and the area available for repair. (b) Shows the placement of the fibular tunnel with anchor suture. (c) Provides a schematic representation of the anatomy involved in Jaw-designed repair of ATFL (F: fibula, T: talus, A: anterior talofibular ligament, C: Calcaneofibular Ligament). (d) Diagrammatic sketch of the Jaw-designed suture passer suturing the ATFL (F: fibula, T: talus, A: anterior talofibular ligament, S: suture anchor, J: Jaw-designed suture passer).
Postoperative management
Postoperatively, a short leg cast was applied and maintained for 2 weeks, during which non-weightbearing gait exercises were performed. The cast was then discontinued, and an elastic ankle support brace was applied. Patients were then directed to engage in mild active range of motion exercises for the ankle, peroneal strengthening, and proprioception exercises, and weightbearing was gradually progressed. At 3 months postoperatively, patients could freely ambulate, and participate in physical exercises at 6 months postoperatively.
Clinical outcome evaluation
Patients completed outcome measures preoperatively and at last follow-up. Functional outcomes were evaluated using the American Orthopaedic Foot and Ankle Society ankle-hindfoot scale (AOFAS; 0-100 points) total score; Karlsson Ankle Functional Score (KAFS 0-100 points); Tegner activity score (TAS: 0-10 points); 10-point visual analog scale for pain; Additionally, intraoperative ligament suture time was meticulously recorded for both groups.
The data analysis was conducted using the statistical software SPSS version 26.0. The data are presented as mean ± standard deviation (SD). All outcome scores were compared between the preoperative and at last follow-up using the Wilcoxon signed rank (paired) test, and scores were compared between the Lasso-loop and Jaw-designed groups using the t test. Statistical significance was set at p < .05.
Results
Demographic chronic lateral ankle instability of the patients.

Comparison of outcome scores between preoperative and the last follow-up in the Lasso-loop and Scorpion groups.

Comparison between the 2 groups.

Discussion
This study demonstrated that both the Lasso-loop and Jaw-designed suture passer techniques achieved favorable clinical outcomes for patients with CLAI. While functional improvements were comparable between groups, the Jaw-designed technique notably required less intraoperative stitching time. These findings suggest that the Jaw-designed suture passer offers a more efficient and technically accessible alternative for arthroscopic ATFL repair without compromising clinical efficacy.
Operative treatments for CLAI include a variety of procedures, from simple repairs to intricate reconstructions. Among these, the modified Broström operation stands out as the most prevalent and the gold standard surgical management for treatment the lateral ankle ligament complex.7,15,16 Various clinical studies have consistently reported favorable outcomes for patients undergoing the arthroscopic modified Broström technique.1,17–19 In a follow-up study involving 24 patients who had undergone this procedure for CLAI, the mean follow-up duration was 34.7 months. Remarkably, these patients were found to have high-functioning ankle joints with a mean AOFAS score of 97. 20 However, biomechanical research has repeatedly demonstrated that repairs are significantly weaker than the intact lateral ankle ligaments. 21 Therefore, significant research has been dedicated to optimizing and strengthening repair. Most of the operators attempted to reinforce the construct by using the inferior extensor retinaculum (IER). However, there are still controversy over whether reinforcement of the ATFL using the IER is necessary and reliable.22–24 Takao et al. 8 introduced a simplified technique, repair of the lateral ligament alone using a Lasso-loop stitch. The specific surgical procedure has been explained in the method. Qin et al. 25 conducted a follow-up study involving 39 cases of CLAI treated with the fully intra-articular Lasso-loop technique. The outcomes revealed a significant enhancement in ankle function scores. For our retrospective study, the Lasso-loop stitch technique was found to be reliable and safe, with good clinical outcomes. However, it is emphasized that the Lasso-loop technique was not easy to perform and would increase suture time significantly. Furthermore, ATFL could be avulsed for constant rotation. The Lasso-loop stitch technique could be challenging for novices.
To simplify surgical procedures and enhance the strength of ATFL, we utilize the Jaw-designed Suture-Passer technique for the treatment of CLAI, which initially was employed for repairing rotator cuff injuries, this technique has been adapted by researchers in recent years to address ramp lesions in the posterior horn of the medial meniscus.9,26 The results have demonstrated that the Jaw-designed suture technique is simple, easy to reproduce, and does not cause additional lesions, making it a cost-effective alternative to conventional methods. It has consistently produced satisfactory clinical outcomes. Previous studies have reported on the application of the Jaw-designed suture passer technique to repair the lateral ligaments of the ankle joint. Guillo and Carvalho et al.10,11 used the Jaw-designed suture passer technique when describing an all-inside endoscopic Broström-Gould method. Goyonnet et al. 27 also applied this technique when describing the arthroscopic acute double-row repair for proximal disinsertion of the collateral lateral ligament of the ankle. However, most of these reports lacked clinical outcome data. Our study adds to the literature by providing comparative clinical evidence supporting its use in arthroscopic ATFL repair. Although functional outcomes were similar between groups, the Jaw-designed technique significantly reduced suture time, highlighting its practical advantage in surgical efficiency.
The ATFL originates at the anterior margin of the lateral malleolus and runs anteromedially to the insertion on the talar body. 28 Numerous anatomic descriptions of the ATFL have been given, varying from a single up to three bands.28–31 However, this ligament most commonly compromises a double-banded morphology.28,32,33 In our experience, for repairing the double-banded ATFL, the Lasso-loop technique could only catch the upper band of ATFL to be tightened. However, the Jaw-designed technique has a much wider range of stitches to catch both the upper and the inferior bands of ATFL, as our anatomical schematic illustrates. This is another advantage of this technique.
This study has several limitations. First, the sample size was relatively small, and future multicenter studies with larger cohorts are needed to confirm our findings. Second, although all procedures were performed by a single experienced surgeon, the lack of randomized group assignment introduces the potential for selection bias. Third, as a retrospective analysis, this study is subject to information bias and lacks control over confounding variables that may influence outcomes. Additionally, the mechanical strength of the repaired ligaments was not objectively assessed during follow-up.
Conclusion
In conclusion, the Jaw-designed suture passer technique offers a simplified and time-efficient approach to arthroscopic ATFL repair, achieving clinical outcomes comparable to the Lasso-loop technique. Its ability to address the double-banded structure of the ligament, along with ease of use, makes it a practical and reliable option for treating chronic lateral ankle instability, particularly for surgeons seeking to reduce operative complexity.
Footnotes
Author note
ICMJE forms for all authors are available online.
Authors contributions
Weiwei Mao and Zhigao Jin contributed equally to this work and should be considered co-first authors. Ying Wang and Jianzhong Qin conceived and supervised the study. Weiwei Mao and Zhigao Jin participated in the design of this study and wrote the manuscript. Yong Zhang and Wei Li analyzed the data. Ying Zhu and Weiqi Kong performed and analyzed the experiments. Ying Wang and Jianzhong Qin also reviewed and substantially revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Open Research Fund of the State Key Laboratory of Biotherapy, grant No. (SKLB202409); the Project of Suzhou Sports Bureau, grant No. (TY2024-103); the Project of State Key Laboratory of Radiation Medicine and Protection, Soochow University, grant No. (GZK1202303); the Project of Second Affiliated Hospital of Soochow University 'Resident Standardized Training Capacity Building Support Program', grant No. (ZPTJ-TD202405); the Project of 2023 'Four-Party Co-Construction' Special Project on Education and Teaching Reform of Suzhou Medical College, grant No. (MX12301923).
Ethics statement
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.