
Abstract
Keywords
Introduction
The goal of rotator cuff repair is to achieve high initial fixation strength, minimize gap formation, maintain mechanical stability under cyclic loading, and optimize the biology of the tendon–bone “healing zone” until the cuff adheres biologically to the bone.1,2 The retear rate varies according to the size of the tear and related muscle fatty infiltration (FI). 3
Several alternative procedures to direct rotator cuff repair have been proposed.4–12 Among them, additional biceps augmentation (ABA) using the autologous long head of the biceps tendon (LHBT) as a graft fixed at different fixation points on the supraspinatus footprint and biceps tenotomy intra-articularly,13,14 is appealing because the graft is available locally and the procedure is free of additional costs and potentially time-saving. 15 Barth et al. proposed the biceps superior capsular reconstruction (BSCR), in which the LHBT is kept intra-articularly, with biceps tenotomy at the distal portion inside the bicipital groove. This technique has been proven to provide less infraspinatus retear in massive posterosuperior rotator cuff tears (RCTs). 16 The results of these techniques are similar to those of traditional superior capsule reconstruction (SCR) using iliotibial band autograft or dermal allografts. 17 Chiang et al. demonstrated that in cases with large to massive reparable RCTs, cuff repair combined with BSCR as reinforcement may provide lower retear rates and earlier functional recovery than conventional cuff repair with LHBT tenotomy. 18 The results of the technique were encouraged by an original study, a biomechanical study and a systemic review.18–20 However, LHBT contains a large network of sensory and sympathetic nerve fibers predominantly near its insertion between the joint capsule and labrum.21,22 Leaving LHBT intra-articularly may lead to anteroposterior superior labral lesions around the tendon origin, which could induce pain. 23 Currently, literature comparing the outcomes of these two surgical methods in medium to large posterosuperior RCTs is scarce.
Therefore, this study aimed to compare the outcomes of ABA and BSCR in arthroscopic RCT repair. We hypothesized that ABA and BSCR yielded comparable clinical and radiological outcomes and retear rates at the 2-year follow-up in patients with medium to large RCTs.
Materials and methods
Study design
This study was approved by the ethics committee of our institution and informed consent was obtained from all patients. Patients who underwent ABA and BSCR between January 2019 and May 2020 were included in this retrospective comparative cohort study. All procedures were performed by the same surgeon. The inclusion criteria were patients diagnosed with medium to large RCTs according to the Rodeo classification 24 (medium, 1–3 cm; and large, >3 cm) and less than Patte stage 3 25 tendon retraction with at least 2 years of follow-up, acromiohumeral distance (AHD) >7 mm on the anteroposterior radiograph in neutral rotation, and FI < Goutallier grade 3. 26 Exclusion criteria were previous ipsilateral shoulder surgery, subscapularis tear > Lafosse type 3, 27 fractures, infection-related pathologies, partial or complete tear of LHBT, 28 severe glenohumeral joint osteoarthritis, and deformity of the humeral head on preoperative X-ray. We also classified the treated RCTs according to Collin classification 29 regarding the involvement of cuff tendons. Patients in the ABA group received independent double-row techniques 30 for RCTs repair and augmented with ABA. Patients in the BSCR group were treated with the same technique, while the biceps was used for SCR. The tear size was measured during the surgery by the same surgeon.
Surgical techniques
All patients were placed in a beach-chair position. After general anesthesia and interscalene nerve block, complete inspection of the glenohumeral joint and subacromial space was performed through standard posterior, lateral, and anterolateral working portals. For a subscapularis tendon tear repair, an anterior portal was created. Arthroscopic debridement using a shaver and a radiofrequency device was performed in all patients with rotator interval release. Next, the torn subscapularis was pulled with a grasper after adequate release to determine cuff reparability. All Lafosse type 1 and 2 subscapularis tears were repaired with a suture-based anchor (2.9 mm Juggerknot (Zimmer Biomet, Warsaw, Indiana, USA)).
ABA group
A metallic, bioabsorbable, all-suture, or polyetheretherketone double or triple suture-loaded anchor was inserted through the 5-mm anterolateral portal into the supraspinatus footprint 8 mm posterior to the bicipital groove as a medial-row anchor, recreating the anterior rotator cable.
31
Another anchor was implanted in the lateral part of the greater tuberosity as a lateral-row anchor. One suture limb from the medial-row anchor was used for biceps tenodesis in a lasso-loop manner. After fixing the LHBT, a biceps tenotomy was performed intra-articularly, leaving a 5-mm biceps stump around the medial-row suture anchor for anterior-cable augmentation. In the way, LHBT would be rerouted 8 mm posteriorly from bicipital groove, serving as additional soft tissue beneath the repaired cuff. Additionally, one or two limbs of the medial-row sutures were passed through the musculotendinous junction of the torn supraspinatus using a cuff hook suture manipulator (Stryker, San Jose, CA, USA). The sutures from the lateral-row anchor were withdrawn simultaneously using the independent double-row technique developed by Collin et al.
30
This created one or two mattress sutures in the medial row and two sutures in the lateral row. The complete surgical details are shown in Figure 1. (A, B, C) Imaging findings in a 65-year-old woman with a right-sided medium-sized supraspinatus tear with a negative tangent sign. (D) Viewing from the lateral portal, an intact LHBT is seen. (E) A triple-loaded all-suture anchor has been inserted 8 mm posterior to the bicipital groove as a medial-row anchor. (F) After fixing the LHBT, a biceps tenotomy has been performed intra-articularly, leaving a 5-mm biceps stump around the medial-row suture anchor for anterior-cable augmentation. (G) When fixing the sutures from lateral-row anchor, SSP covers the LHBT remnant. (H) After final knot-tying, the SSP footprint covers the LHBT remnant. LHBT: long head of biceps tendon; SSP: supraspinatus.
BSCR group
A medial-row suture-based anchor was inserted at the midpoint of the greater tuberosity of the humerus. One or two suture limbs were passed individually through the intact LHBT in a lasso-loop configuration. The sutures were tied while keeping the arm in 40° flexion, 40° abduction, and neutral rotation, transferring the proximal portion of the LHBT to the supraspinatus footprint. The LHBT was tenotomized in the bicipital groove distal to the sutures, with transverse humeral ligament release. The distal part of the tendon was left free without any additional tenodesis. The glenoid insertion of the LHBT was preserved to serve as an autograft for BSCR, as described by Boutsiadis et al.
32
The sutures were not cut but retrieved from the anterior working portal for further passage. The unused medial-row suture was then retrieved along with sutures from the lateral-row anchor using the independent double-row technique
30
(Figure 2). (A, B, C) Imaging findings in a 65-year-old female patient with a large right-sided supraspinatus tear with a negative tangent sign. (D) Viewing from the lateral portal, the SSP tendon is retracted to approximately the glenoid level. (E) A triple-loaded all-suture anchor has been inserted 8 mm posterior to the bicipital groove as a medial-row anchor. (F) A biceps tenotomy has been performed inside the bicipital groove distal to the sutures with transverse humeral ligament release. (G) The glenoid insertion of the LHBT is intact. The LHBT has been rerouted posteriorly according to the position of the medial-row suture anchor, serving as an autograft for BSCR. (H) After final knot-tying, the SSP footprint covers the LHBT remnant. LHBT: long head of biceps tendon; SSP: supraspinatus; BSCR: biceps superior capsule reconstruction.
The difference between the ABA and BSCR groups was the position of the biceps tenotomy. In ABA group, the LHBT was rerouted posteriorly and tenotomized intra-articularly, leaving a 5-mm stump to augment the repaired supraspinatus. In BSCR group, the LHBT was rerouted 8 mm posteriorly from bicipital groove, too, but tenotomized distal to the sutures, leaving the whole intact LHBT intra-articularly as a BSCR (Figure 3). The difference between ABA and BSCR. In the ABA group, the LHBT was rerouted posteriorly and tenotomized intra-articularly, leaving a 5-mm stump to augment the repaired SSP. In the BSCR group, the LHBT was rerouted posteriorly, too, but tenotomized distal to the sutures, leaving the whole intact LHBT intra-articularly as a BSCR. ABA: additional biceps augmentation; LHBT: long head of biceps tendon; SSP: supraspinatus. BSCR: biceps superior capsule reconstruction.
Study variables
The outcome of interest was the 2-year functional and radiological results of ABA. The secondary objective was to compare the results with those of BSCR. The following baseline characteristics were assessed: age, sex, shoulder side, limb dominance, size of the rotator cuff lesion, and type of lesion according to the Collin et al. classification. 29 At the final follow-up, we evaluated the number of patients with minimal clinically important differences (MCIDs) for each score to compare patients before and after the surgery.
Clinical and radiographic evaluation
Clinical assessment
All patients underwent a detailed physical examination at the outpatient department preoperatively and at the 2-year follow-up by an independent orthopedic surgeon including (1) Constant–Murley shoulder score (CMS), 33 (2) American Shoulder and Elbow Surgeons (ASES) score, 34 (3) subjective shoulder value (SSV), 35 (4) visual analog scale (VAS, 10-point grading system) pain scores, and (5) active range of motion (ROM). We measured forward flexion (FF), external rotation by the side (ER1), and internal rotation (IR). 36 The active ROM, FF, and ER1 were measured in the outpatient department with a goniometer. IR was measured by recording the highest vertebral body the patient could reach using the thumb. 36
Radiological assessment
Standard anteroposterior radiography was performed to assess the AHD, 37 superior capsular distance (SCD), 37 and Hamada classification 38 of the glenohumeral joint before surgery and at the 2-year follow-up. In all patients, rotator cuff integrity was evaluated before index surgery using magnetic resonance imaging (MRI). The Goutallier classification, as modified by Fuchs et al. 26 was used to assess supraspinatus and infraspinatus muscle FI (grade 0, no FI; grade 1, some fatty streaks; grade 2, less fat than muscle; grade 3, as much fat as muscle; and grade 4, more fat than muscle). The presence of the tangent sign, retraction, thickness, and length of the supraspinatus tendon, and integrity of the LHBT were assessed.39–41
Rotator cuff tendon retear was evaluated in consensus by two independent observers, one musculoskeletal radiologist and one orthopedic surgeon, different from the operating surgeon, using ultrasound. 42 Tendon healing was assessed using an M-Turbo ultrasonography system (Fujifilm Sonosite; Tokyo, Japan). The ultrasound protocol consisted of (1) axial and longitudinal evaluation of the supraspinatus tendon, (2) axial and longitudinal evaluation of the infraspinatus tendon, and (3) evaluation of subacromial or subdeltoid bursal fluid. Structural integrity was evaluated at the 2-year follow-up based on the Sugaya classification. 43 Grades 1, 2, and 3 were considered to indicate a healed tendon, and Grades 4 and 5 were considered to indicate a retear. 44
Rehabilitation
Patients in both groups received identical rehabilitation protocols, including wearing an abduction brace for 6 weeks following surgery. During the first 6 weeks, all patients only performed active hand, wrist, elbow, scapular-retraction exercises, and passive ROM. During the second 6-week period, active-assisted elevation in the plane of the scapula was initiated, followed by progression to active elevation. Formal physical therapy and a home exercise program were continued for 3 months postoperatively. 24
PICO of this study
P – patient, population, or problem
• Patients: Individuals with medium to large posterosuperior rotator cuff tears (RCTs). • Problem: Rotator cuff repair and the associated retear rate after surgery.
I – intervention
• Procedure: Additional Biceps Augmentation, • Uses the long head of the biceps tendon (LHBT) as a graft, fixed at different fixation points on the supraspinatus footprint with intra-articular tenotomy.
C – comparison
• Procedure: Biceps Superior Capsular Reconstruction (BSCR) • Uses the LHBT intra-articularly as an autograft for superior capsular reconstruction with distal tenotomy.
O – outcomes
• Primary Outcomes: Functional scores (CMS, ASES, SSV, VAS) Range of motion (ROM) Pain improvement Retear rate at 2-year follow-up • Secondary Outcomes: Radiographic evaluation (AHD, SCD) Structural integrity of the repaired tendon (by ultrasound) Complications (e.g., infection, nerve injury)
Statistical analysis
Statistical analyses were performed using SPSS software (version 25.0; IBM, Armonk, NY). The means, standard deviations, and ranges were calculated. Pearson’s chi-square or Fisher’s exact test was used to compare categorical variables. A t test or Wilcoxon rank sum was performed to analyze the difference in pre- and post outcome scores for ROM, CMS, ASES score, SSV score, and VAS score. Two-tailed p values of less than .05 were considered significant. We calculated the MCID for CMS, ASES, SSV, and VAS scores using pre- and post-treatment data. Relevant variables were extracted and paired t-tests were conducted. Cohen’s d was computed for each variable to determine effect size. The MCID was then calculated by multiplying Cohen’s d with the pre-treatment standard deviation of each variable. The resulting MCIDs were 10.4 for CMS, 13 for ASES, 12 for SSV, and 1.6 for VAS. These values represent the threshold for clinically significant changes in each respective score.
Results
Demographic characteristics of patients.
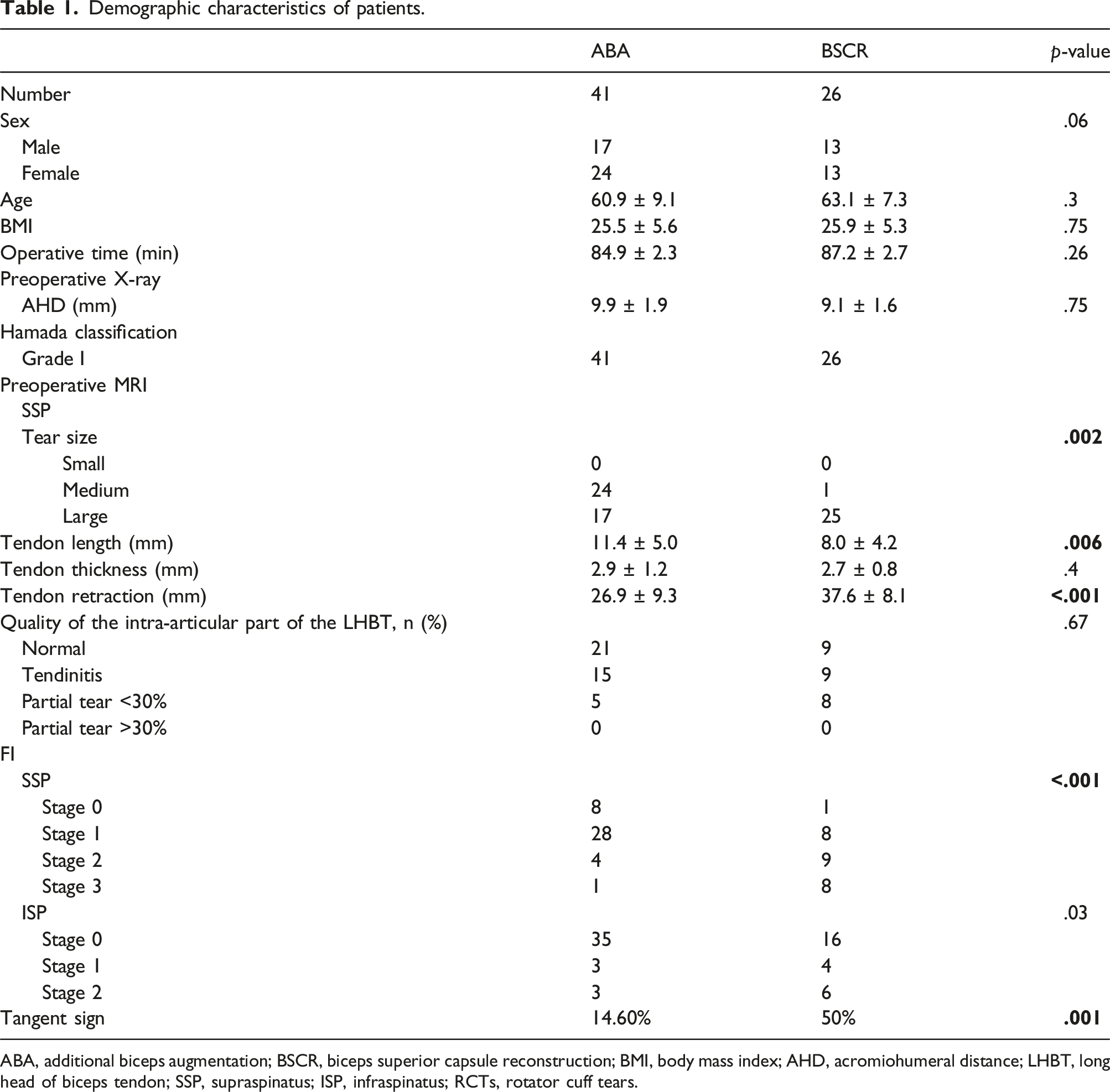
ABA, additional biceps augmentation; BSCR, biceps superior capsule reconstruction; BMI, body mass index; AHD, acromiohumeral distance; LHBT, long head of biceps tendon; SSP, supraspinatus; ISP, infraspinatus; RCTs, rotator cuff tears.
Clinical outcomes
Clinical and radiological outcomes at the 2-year follow-up.

ABA: additional biceps augmentation; BSCR: biceps superior capsule reconstruction; ROM: range of motion; FE: forward elevation; ER1: external rotation 1; IR: internal rotation; Preop: preoperative; Postop: postoperative; SSV: subjective shoulder value; ASES: American shoulder and elbow surgeons; AHD: acromiohumeral distance; SCD: superior capsule distance.
Radiological outcomes
Radiographic evaluation at the 2-year follow-up revealed no significant difference in AHD and SCD in both groups compared with those preoperatively. Both groups showed no significant difference in preoperative AHD because all patients included in our study were classified as Hamada Class I. The retear rates in the ABA and BSCR groups were 0% and 7.7%, respectively (p < .001). Among them, the ABA group had 35 Sugaya 1 and 6 Sugaya 2, whereas the BSCR group had 14 Sugaya 1, 9 Sugaya 2, 1 Sugaya 3, and 2 Sugaya 5, respectively (Table 2).
Complications
No major surgical complications, such as nerve injury, suture anchor loosening, or deep infections, were observed in either group.
Discussion
This retrospective comparative study confirmed our hypotheses that both ABA and BSCR provided comparable clinical and radiological outcomes at the 2-year follow-up. However, the BSCR group had a higher retear rate than the ABA group, probably due to differences in tendon tear size, retraction, residual tendon length, presence of tangent sign, and muscle FI.
Arthroscopic rotator cuff repair with LHBT tenotomy is commonly performed to improve clinical outcomes.45–47 In the ABA group, we made an effective use of the LHBT with intra-articular tenotomy, leaving a 5-mm biceps stump around the medial-row suture anchor for anterior-cable augmentation, as the anterior rotator cable is the primary force-transmitting structure at the proximal humerus. 31
Park et al. biomechanically proved that anterior-cable reconstruction using autologous LHBT with preservation of its superior labrum attachment decreased proximal humerus superior migration and subacromial contact pressure without limiting ROM. 20 Our study utilized a technical modification of SCR using an LHBT autograft, which supposedly prevents superior humeral head migration and restores the anteroposterior shoulder muscle force couples. In the BSCR group, we divided the LHBT in the bicipital groove distal to the knot from the medial-row suture anchor and rerouted it posteriorly while preserving the superior labrum attachment. This configuration may provide a spacer effect in SCR. The average LHBT thickness was comparable with that of the autologous fascia lata graft, and the tendon properties were close to those of the superior rotator cuff. 48 Additionally, we released the transverse humeral ligament because rerouting of the LHBT posteriorly results in significant elongation of the biceps muscle-tendon unit. Over-tension of the biceps muscle tendon unit may cause clinical symptoms and put the fixation at a high risk of failure. The release of the transverse humeral ligament partially decreased this elongation. 49
Both ABA and BSCR can be performed for medium to large-size RCTs as both groups had comparable (p = .08) tear tendon involvement classified according to Collin et al. 29 with comparable clinical outcomes. However, patients in the BSCR group had a higher retear rate than those in the ABA group.
The reparability of RCTs can be predicted based on several criteria. In 1990, Hamada et al. proposed a radiographic classification of massive RCTs based on AHD, which is a measurement of the subacromial space. 38 Studies have shown that AHD is positively correlated with the size of the RCT and degree of FI of the rotator cuff muscles,50,51 and is a predictor of both short-term disability 52 and functional status. 53 In this study, AHD at the 2-year follow-up was not significantly different compared to that preoperatively in both groups. This indicated similar satisfactory outcomes in the ABA and BSCR groups. Brolin et al. proposed that Hamada Grade 1 or 2 may be amendable to joint-preserving operations. 54 In our series, all 67 patients were Hamada Grade 1 without significant differences between the groups. Regarding muscle FI and the associated retear rate, Godeneche et al. reported that at the 10-year follow-up, shoulders with supraspinatus FI stages 0, 1, and 2 had retear rates of 10%, 22%, and 31%, respectively. 55 Meyer et al. reported that not only the muscle FI but also the remnant tendon length impacts the retear rate of the repaired supraspinatus. 40 In their series, patients with preoperative Goutallier stages 2–3 and a tendon length <15 mm had a failure rate of 92%; however, the failure rate was only 33% in patients with tendon length >15 mm. For Goutallier stages 0–1, the corresponding failure rates were 57% and 25%, respectively. 40 In our series, only one patient in the ABA group had Grade 3 supraspinatus muscle FI, and the average remnant tendon length was 11.4 ± 5.0 mm. In contrast, 30.8% (8 out of 26) patients in the BSCR group had Grade 3 supraspinatus muscle FI with an average remnant tendon length of 8.0 ± 4.2 mm, which rendered the RCTs irreparable, and additional augmentation such as an LHBT graft was required instead of direct cuff repair. Although preoperative demographics such as muscle FI and residual tendon length differed significantly between the groups, both groups improved after surgery and showed comparable functional outcomes such as VAS scores, IR, ER1, and FF, and radiological outcomes such as AHD and SCD.
SCD is a measurement of the actual restoration of superior stability postoperatively, as it reflects anatomic recentering of the humeral head within the glenoid. It helps quantify the degree of maintenance of superior capsular stability provided by SCR. 37 Superior capsular stability provided by concomitant SCR and rotator cuff repair plays an important role in decreasing failure rates in massive rotator cuff repairs. This may be due to decreased tension on the repair after SCR and maintenance of superior capsular stability. In our study, the 26 patients who underwent concomitant BSCR and rotator cuff repair for medium-to-large RCTs showed favorable 2-year clinical and radiographic outcomes, which were comparable to those in the ABA group.
Regarding the tangent sign, Sheean et al. reported that a positive tangent sign indicates the possibility of incomplete repair of the supraspinatus (30% irreparable), whereas a negative tangent sign indicates the possibility of a complete repair (6.3% irreparable, odds ratio = 6.3, p = .0102). 56 In our series, the tangent sign was positive in 14.6% and 50% of patients in the ABA and BSCR groups, respectively. However, the surgical results were comparable between both groups. This finding implies that patients should be treated individually according to the disease severity.
Limitations
This study had several limitations. First, it was a retrospective study with patients with different preoperative severities of RCTs (e.g., RCT size, remnant tendon length, rotator cuff muscle FI, and presence of the tangent sign) treated using two different surgical techniques. Although partial repair of massive cuff tears historically provides good clinical outcomes,57,58 one-half of the patients in a retrospective study of 31 patients had worse symptoms after partial repair of a massive rotator cuff defect at a minimum follow-up of 2 years, despite the initial improvement in pain and functional outcomes. 59 Therefore, we maintained LHBT intra-articularly during rotator cuff repair in the BSCR group. Second, complete postoperative MRI evaluation was lacking. We used ultrasound alone to evaluate the integrity of the repaired cuff, which might have some inherent limitations because of operator dependency. 60 However, the sensitivity and specificity of ultrasound for identifying postoperative rotator cuff integrity were reported to be 91% and 86%, respectively. 61 Moreover, the follow-up ultrasound was performed by one musculoskeletal radiologist and one orthopedic surgeon different from the operating surgeon. In fact, a well-trained office staff and an experienced orthopedic surgeon can effectively utilize ultrasonography to accurately diagnose the extent of RCTs. 60
Conclusion
Both ABA and BSCR provided similar clinical and radiological outcomes in patients with medium to large RCTs. The BSCR group had a higher retear rate than the ABA group.
Footnotes
Author contributions
MT wrote the manuscript. PC performed the statistics. AL developed the surgical technique. CY, YC, and CH provided professional opinions regarding the surgery. JC provided all study cases and reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully thank Department of Orthopedic Surgery, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan, CMRPG5K0092, CMRPG3M2032, CLRPG3D0045, CMRPG5K021, SMRPG3N0011, SMRPG3P0011; Minister of Science and Technology, Taiwan, MOST 111-2628-B-182A-016, NSTC112-2628-B-182A-002.