
Abstract
Introduction
Proximal femur resection with proximal femoral replacement (PFR) has become the gold standard treatment for primary bone tumours or metastatic disease. This technique allows for precise tumour removal, minimising the risks of tumour progression or non-union, and enables immediate weight-bearing. Beyond oncological indications, PFR is recommended for complex proximal femur fractures with poor bone quality, failed internal fixation, unsuccessful total hip arthroplasty, proximal femur osteomyelitis, and specific congenital skeletal anomalies.
Bipolar hip replacement (BHR) is a widely used procedure for proximal femoral replacement in oncology cases, involving techniques such as bipolar hemiarthroplasty (BHA), proximal femur bipolar replacement (PFBR), and total femur bipolar replacement (TFBR). As patient outcomes improve, concerns about acetabular wear following reconstruction surgery have increased, given their potential impact on patient functionality and quality of life. The possibility of requiring revision surgery with acetabular replacement is a significant concern for patients who have undergone bipolar hip endoprosthesis replacement.
The decision to replace the acetabulum during PFR remains contentious among surgeons. Some advocate for total hip arthroplasty (THA) due to concerns about future acetabular wear necessitating additional revisions. Conversely, others support using bipolar hip replacement (BHR), asserting that post-hemiarthroplasty acetabular wear is minimal and does not warrant exposing patients to more extensive surgical procedures. Furthermore, hemiarthroplasty offers a broader range of motion and poses a lower risk of dislocation than total hip arthroplasty.
Ultimately, the choice of hip articulation is heavily influenced by patient-specific factors, including age, functional demand, activity level, risk profile (underlying medical conditions and cognitive status), and the condition of the acetabulum.1,2 Ogilvie et al. 3 reported no significant difference in functional outcomes between patients undergoing bipolar hemiarthroplasty and THA. However, the rate of hip dislocation was higher in the THA group, with one patient experiencing 11 dislocations. Additionally, they found that trochanteric attachment to the prosthesis did not result in better functional outcomes.
Our study aimed to evaluate the prevalence of secondary osteoarthritis following bipolar hip endoprosthesis replacement, the necessity for revision to total joint replacement after BHR, the functional status of these patients in relation to radiological evidence of joint degeneration, and the long-term success rates of bipolar hip endoprosthesis replacements.
Methodology
This study is a retrospective study of prospectively collected data from clinical and radiological investigations. Using a convenient sampling method, all patients with orthopaedic oncology cases who underwent bipolar hip replacement (BHR) between 2006 and October 2021 were included in the study and evaluated both clinically and radiologically. Before commencing the study, approval was obtained from our institutional ethics committee (MREC ID NO: 202095-9047). We retrospectively examined our oncology surgical database to identify eligible participants and pinpoint patients who received BHR. The types of BHR procedures considered in this study encompassed bipolar hemiarthroplasty (BHA) for oncology indications, proximal femur bipolar replacement (PFBR), and total femur bipolar replacement (TFBR). The study included patients diagnosed with primary bone tumours, soft tissue sarcomas involving the bone, or metastases affecting the proximal femur with a minimum of 6 months post-BHR. Exclusion criteria comprised patients with underlying rheumatological disorders (such as rheumatoid arthritis and gouty arthritis), neurological disorders (like stroke and Parkinsonism), prior hip surgeries, and pre-operative peri-prosthetic fractures.
A total of 258 patients underwent lower limb endoprosthesis replacement during the study period. 55 patients underwent bipolar hemiarthroplasty, proximal femur and total femur replacements. However, 15 individuals were unreachable, and their clinical records were incomplete, leading to their exclusion from the study. Therefore, the final cohort for analysis consisted of 40 patients. Among these participants, eight individuals had deceased by the time of assessment, rendering them ineligible for the questionnaire-based functional score evaluations. Following bipolar hip replacement (BHR), patients underwent a comprehensive review that encompassed the evaluation of symptoms, functional scores, and radiological imaging.
The medical records were thoroughly scrutinised, and patients were surveyed using questionnaires to detect symptoms of acetabular erosion and ascertain the requirement for analgesics. Symptoms indicative of acetabular erosion or degenerative alterations included mechanical hip pain, anterior groin pain, or anterior thigh pain.
The functional status of the patients was gauged through the utilisation of several assessment tools, namely the Musculoskeletal Tumor Society System (MSTS), Toronto Extremity Salvage Score (TESS), and modified Harris Hip Score (mHHS). The MSTS evaluation comprises six parameters: pain, functional activity, emotional acceptance, use of supports, walking ability, and gait. Each parameter is rated on a scale from 0 to 5, with a higher score denoting superior function. The TESS assessment is a disease-specific metric for patients undergoing limb-preserving surgery for extremity tumours. It evaluates physical disability based on patients’ self-reports regarding their functionality, with a score ranging from 0 to 30 and a higher score indicating better function. The mHHS is divided into two domains: pain and function. This assessment can be administered via a phone interview, and the maximum score achievable is 91. To convert this score into a final score out of 100, it is multiplied by a factor of 1.1. mHHS scores are categorised as follows: <70 (poor result), 70–79 (fair result), 80–89 (good result), and >90 (excellent result). Radiological evaluations included obtaining a plain anteroposterior view of the pelvis focusing on the operated hip (Figure 1). Acetabular erosion was assessed using the grading system developed by Sakr Mazen et al., which classifies erosion into four grades: • Grade 0: No evidence of erosion. • Grade 1: Narrowing of the articular cartilage without bone erosion. • Grade 2: Presence of acetabular bone erosion and early signs of migration. • Grade 3: Protrusion of the acetabulum (protrusio acetabuli). Grading of radiological assessment
11
(Sakr Mazen et al, 2010).

Results
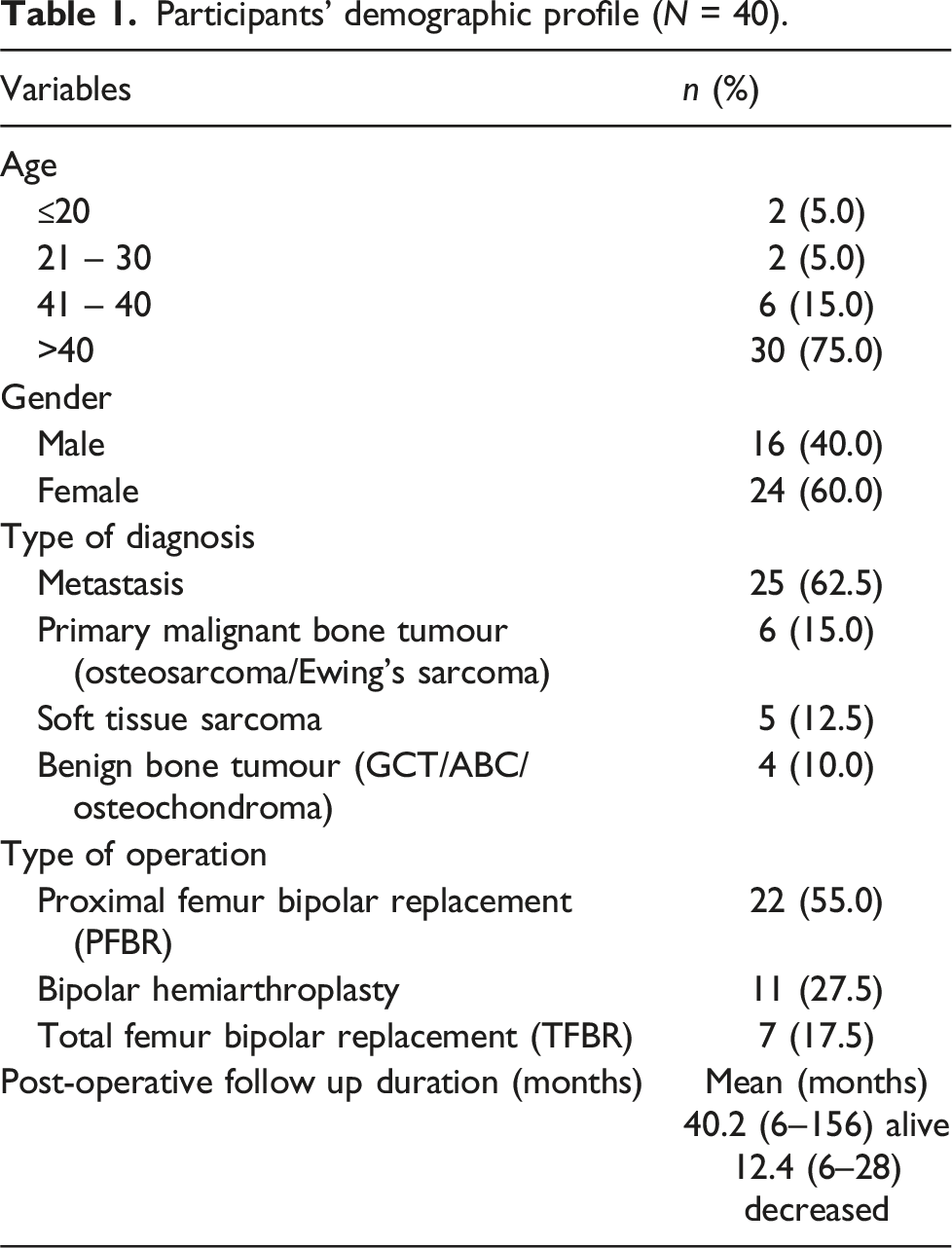
Participants’ demographic profile (N = 40).
Radiological assessment of the acetabular erosion grading post-operatively.

Radiological assessment of the acetabular erosion grading and the presence of hip osteoarthritis pre-operatively. a

aOne patient with no pre-operative pelvis x-ray available in the system.
Within the scope of this study, one patient (2.5%) necessitated revision surgery transitioning from proximal femoral bipolar replacement to total hip replacement because of recurrent hip dislocation post-operation. This revision procedure took place 2 years following the initial surgery. Moreover, two additional patients underwent revision surgeries; however, acetabulum replacement was not required in these cases. One of the patients underwent revision surgery, switching from a hip bipolar hemiarthroplasty to proximal femur bipolar endoprosthesis due to tumour recurrence. The other patient was revised to total femur bipolar endoprosthesis as a result of a periprosthetic fracture.
During the patient interviews with questionnaires, it was observed that eight patients had passed away by the time of the assessment, precluding the performance of functional score assessments on them. Interestingly, among the surviving patients, none displayed grade 2 acetabular erosion.
The median MSTS and TESS score for each acetabular erosion grading.

Significant: *p < 0.05.
The mHHS grading for each acetabular erosion grading.

The Kaplan-Meier curve indicates a noteworthy ten-year survival rate of 77.8% for implant survivorship for bipolar hip endoprosthesis replacement. (Figure 2). Conversely, the same curve illustrates a slightly lower ten-year survival rate of 72.1% when considering overall patient survivorship (Figure 3). There are no differences in the implant survival rate by age groups of 20 – 29, 30 – 39, 40 – 49 and 50 – 59 (p = 0.296). As for patients 60 years old and above, the median implant survival is less than 50%. However, in this study, only three (events) were reported. None were due to acetabulum erosion, leading to symptomatic osteoarthritis (Figure 4). Implant survivorship of bipolar hip replacement (BHR). Overall patient survivorship post bipolar hip replacement (BHR). Implant survival by age category.


Discussion
The study by Henderson et al. 4 aimed to determine the mode, frequency, and timing of endoprosthesis failure. It involved a sample size of 1774 patients who underwent lower limb endoprosthesis replacements. Within this cohort, 403 patients (22.7%) underwent proximal femoral replacement. Similarly, at our centre, a comparable proportion of lower limb endoprosthesis replacement patients, specifically 21.3%, underwent proximal femoral replacement.
Our study found that none of the patients with pre-existing hip osteoarthritis experienced worsening grade 3 acetabular erosions during the review. Among the 16 patients (41%) with grade 1 acetabular erosion, five had pre-existing hip osteoarthritis classified as Tonnis grade 1. Similarly, the two patients (5.1%) with grade 2 acetabular erosion also had pre-existing Tonnis grade 1 hip osteoarthritis. The majority of patients (53.9%) showed no acetabular wear. Post-operatively, it was observed that most patients had adopted a more sedentary, low-physical-activity lifestyle, which most likely contributed to a reduced likelihood of exacerbating the hip degenerative process.
In the study by Stevenson et al., 1 84% of patients exhibited no acetabular wear, while 12% developed grade 1 acetabular erosion and another 12% developed grade 2 acetabular erosion during a follow-up period exceeding 1 year. These findings are consistent with our observation that most patients showed no acetabular wear or deterioration in those with pre-existing hip degeneration. In contrast, a study by Drexler et al. 5 reported that only 4.6% of patients developed hip degenerative changes following bipolar hemiarthroplasty, with all requiring acetabular revision surgery at various intervals postoperatively—at 24, 34, and 47 months.
In our study, one patient (2.5%) required acetabular revision surgery to transition to a total hip replacement 2 years after undergoing proximal femur bipolar replacement. This revision was prompted by recurrent postoperative hip dislocation in the patient’s early twenties, despite the absence of noticeable degenerative changes at the acetabulum prior to the initial replacement surgery. Additionally, two other patients underwent revision surgeries: one transitioned from a hip bipolar hemiarthroplasty to proximal femur bipolar endoprosthesis due to tumour recurrence, and the other revised to a total femur bipolar endoprosthesis following a periprosthetic fracture in a proximal femur endoprosthesis.
Notably, in our observations, no instances necessitated acetabular revision surgery due to mechanical pain or acetabular wear. Stevenson et al. 1 reported clinically insignificant acetabular degeneration within a short to medium-term follow-up, with no cases of acetabular protrusion. In their study, revision surgeries were required for stem fracture, aseptic stem loosening, and local recurrence, which highlight different reasons for revision compared to our findings.
Longer-term studies have indicated revision rates for total hip replacements ranging from 4.6% to 8% in oncology patients. Chandrasekar et al. 6 suggested avoiding unipolar proximal femoral replacement in younger patients or those with a life expectancy exceeding 5 years, citing a higher rate of acetabular revisions in patients younger than 21 years compared to older patients. Inggul et al. 7 observed a higher incidence of acetabular erosion in unipolar (20%) versus bipolar hemiarthroplasty (5%) within the first year of follow-up; however, this discrepancy lessened between the two groups by the two- and four-year marks.
Matthew et al. 8 reported a 5% conversion rate (6 patients) from bipolar hemiarthroplasty to total hip arthroplasty (THA) in his 10-year follow-up of 148 patients, mostly due to symptomatic acetabular erosion. Additionally, 13% (19 patients) developed acetabular cartilage erosion of more than 2 mm, with 5 patients experiencing protrusion. Drexler et al. 5 found that 4.6% of the population underwent conversion to THA due to symptomatic degenerative changes.
Cannon et al. 9 concluded that total hip arthroplasty is unnecessary in patients with proximal femur tumours unless the patient has osteoarthritis, a tumour involving the acetabulum, or instability requiring a constrained component. In his study, only 1.6% (7 of 447 patients) needed conversion to THA, primarily for non-pathologic acetabular fracture (one patient) and two cases each for instability, acetabular metastatic disease, and groin pain. The median time to conversion was 13 months, with two cases of groin pain occurring in obese patients due to proximal migration of the implant.
Feinstein et al. 10 reported none of the tumour-related bipolar proximal femur replacement (PFR) patients required conversion to THA secondary to acetabular wear. In his study, one patient complained of groin pain due to local recurrence, but no major acetabular wear was observed on radiographs. However, 12 patients (19%) underwent PFR revision within a mean of 5.4 years post-implantation. Revisions were performed for 6 cases of aseptic loosening, two cases of periprosthetic fracture, two cases of recurrent dislocation, and one case each of pathological fracture and infection. He also noted slightly higher dislocation and deep infection rates in tumorous PFR cases compared to non-tumorous PFR cases.
Henderson et al. 4 categorised endoprosthesis reconstruction failures into mechanical or non-mechanical causes, further dividing them into five modes of failure: Type 1 - Soft-tissue failure, Type 2 - Aseptic loosening, Type 3 - Structural failure, Type 4 - Infection, and Type 5 - Tumour progression. Henderson’s study identified infection (Type 4) as the most prevalent mode of failure, particularly associated with the anatomic location of the endoprosthesis reconstruction, with a higher incidence observed at distal humeral replacements. 4 In our observations, the modes of failure for three revision surgeries included one instance of Type 1 (hip dislocation), one of Type 3 (periprosthetic fracture), and one of Type 5 (tumour recurrence).
Our observations suggest that the radiological grading of hip osteoarthritis does not significantly correlate with functional scores. Specifically, while the Musculoskeletal Tumor Society (MSTS) score and modified Harris Hip Score (mHHS) did not show statistical significance in patients with acetabular erosion grades 0 and 1, there was a notable difference in functional outcomes between these groups based on the Toronto Extremity Salvage Score (TESS). The median TESS score was 89.83 for grade 0 and 81.41 for grade 1, with a statistically significant p-value of 0.045. In the evaluation of the TESS, it was observed that items related to sports participation and kneeling activities were among the lowest-scored elements. This difference might be because TESS is a patient-reported outcome measure that focuses on patients’ perception of their ability to perform daily activities. It may be more sensitive to the nuanced, subjective functional limitations that patients experience with acetabular erosion, which could explain why it showed a significant difference. The TESS emphasises how patients perceive their function in daily life, which could be more affected by changes in the hip joint over time, even when more objective measures like pain and mobility are less obviously impacted. Therefore, the TESS score might be more sensitive to the subtle, patient-perceived functional limitations caused by acetabular erosion. In contrast, the MSTS and Modified Harris Hip Score might not capture those changes as effectively, focusing more on pain and mechanical aspects of hip function. Matthew et al. 8 reported no difference in the Musculoskeletal Tumour Society (MSTS) score between patients with more than 2 mm acetabular erosion and those without.
Functional scoring inherently involves subjectivity as it reflects a patient’s perception of their quality of life and activity levels. Postoperatively, patients may have different pain thresholds and activity preferences. Interestingly, mechanical pain did not significantly limit functional activity, as most patients could resume their activities after brief rest periods or with pain relief medication. In a retrospective clinical and radiological study on patients who underwent cemented bipolar hemiarthroplasty for a neck of femur fracture by Venkatesh et al., 2 it was observed that acetabular erosion grade worsened with the follow-up interval. However, the modified UCLA score did not show clinical significance when correlated with acetabular erosion grade, with a p-value of 0.71.
In implant survivorship for bipolar hip endoprosthesis replacement, the Kaplan-Meier curve suggests a notable ten-year survival rate of 77.8%. Drexler et al. 5 concluded that cemented bipolar proximal femur replacement (PFR) is a long-lasting implant for reconstructing tumours involving the proximal femur, with a limb salvage rate of 97%. Bernthal et al. 11 reported a 5.8% conversion rate to total hip arthroplasty (THA) from cemented bipolar PFR in patients with primary tumours (3 for aseptic loosening, one for deep infection, and one for implant mechanical failure). All five patients experienced groin pain, which resolved following THA. He stated that cemented bipolar PFRs are a durable reconstruction for proximal femur tumours with a 99% limb salvage rate (Bernthal et al., 2010). Menendez et al. 12 concluded that bipolar hemiarthroplasty generally outlasts the patient with neoplastic disease, showing greater implant survivorship than total hip articulating head segments and should be considered the gold standard for treating proximal femur tumours. Dislocation rates in THA are three times higher than those in bipolar hemiarthroplasty patients, as a larger bipolar femoral head provides greater stability. The implant survival by age showed no difference between all age groups below 60. However, for those above 60, there was a 50% implant failure rate. This is probably biased as the number of patients above 60 is small. Furthermore, none of the three revisions were related to symptomatic osteoarthritis of the acetabulum secondary to the bipolar articulation.
Several limitations need to be acknowledged in our study. Firstly, the study has a relatively small sample size, a short observation period, and a retrospective design. A longer follow-up could reveal more significant hip degenerative changes and associated symptoms. The small sample size is because these are orthopaedic oncology cases, and they can not be compared to those who undergo these surgeries for trauma or degenerative joint disease.
Secondly, due to the retrospective nature of the study, patients were assessed at varying postoperative durations. A standardised assessment time frame for all patients would allow for a more precise comparison of radiological assessments and functional statuses at specific postoperative intervals.
Thirdly, it is important to consider that a patient’s baseline functional status and overall health condition can significantly impact their functional scores during interviews. Patients with poorer initial functional statuses will likely display lower functional assessment scores. This potential bias could be addressed by evaluating patients’ preoperative functional statuses, grouping them based on these scores, and analysing postoperative data accordingly.
In conclusion, our study reveals a low incidence of acetabular erosion in cases of bipolar hip endoprosthesis replacement. Despite hip degenerative changes detected in radiological assessments, they do not have a notable impact on patient’s functional status. These findings suggest that bipolar hip endoprosthesis replacement is a resilient limb-saving reconstruction technique capable of lasting beyond patients’ lifespans and is generally well-received by oncology patients.
Footnotes
Author contributions
OOI YING JING: Carried out the study and wrote the draft of the manuscript. Rupini Devi Santharalinggam: Carried out the statistics for the study. Vivek Ajit Singh: Conceptualization, Supervision and Review and editing. Nor Faissal Yasin: Project administration, Review and Editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.