
Abstract
Keywords
Introduction
The hallux, or big toe, plays an important role in foot mechanics, significantly contributing to foot movement, weight bearing, and overall balance. 1 Because of this critical role, it is recommended that the surgical treatment of hallux fractures be planned with consideration of the displacement between the fragments, the type of fracture line, and the difficulty of maintaining closed reduction. 2
Since it plays a vital role in foot function, achieving anatomical reduction in the surgical treatment of hallux fractures is recommended for the rapid restoration of normal function.3,4 Various surgical techniques have been described for the fixation of hallux fractures.5–7 Despite developments in surgical techniques and the implants used, these methods are not without complications, including joint stiffness, tendon adhesions or ruptures, decreased range of motion, toe deformities, pseudoarthrosis, and osteomyelitis.4,8,9
In recent years, minimally invasive techniques such as percutaneous plate fixation, nail fixation, and Kirschner wire (K-wire) fixation under fluoroscopy have gained popularity. These methods, frequently used in the treatment of extra-articular hallux fractures, aim to minimize orthopedic complications, shorten hospital stays, and accelerate the return to daily activities.10,11
To further improve the management of these fractures, we conducted a biomechanical evaluation of different configurations of K-wires, which are frequently used in closed reduction and fixation. The literature contains limited biomechanical studies investigating the strength and stability of K-wire applications, a cost-effective and simple method, across various bones and configurations.12,13 This in vitro study focuses on comparing two distinct K-wire configurations parallel (PC) and cross (CC) in the fixation of extra-articular transverse osteotomies of the proximal phalanx of the first toe using a sawbone model. Our objective was to determine the differences in fracture line stability and weight-bearing resistance between these two K-wire configurations.
Materials and methods
In this study, we utilized 30 synthetic composite bone models of the anatomical right 1st toe (Sawbones USA, Forefoot, Solid Foam, Right, Large, SKU: 1122-20). These models, used for fixation with different configurations, were divided into two equal groups. Each model underwent a standard osteotomy to create a transverse fracture line in the shaft of the proximal phalanx.
Osteotomy and fixation
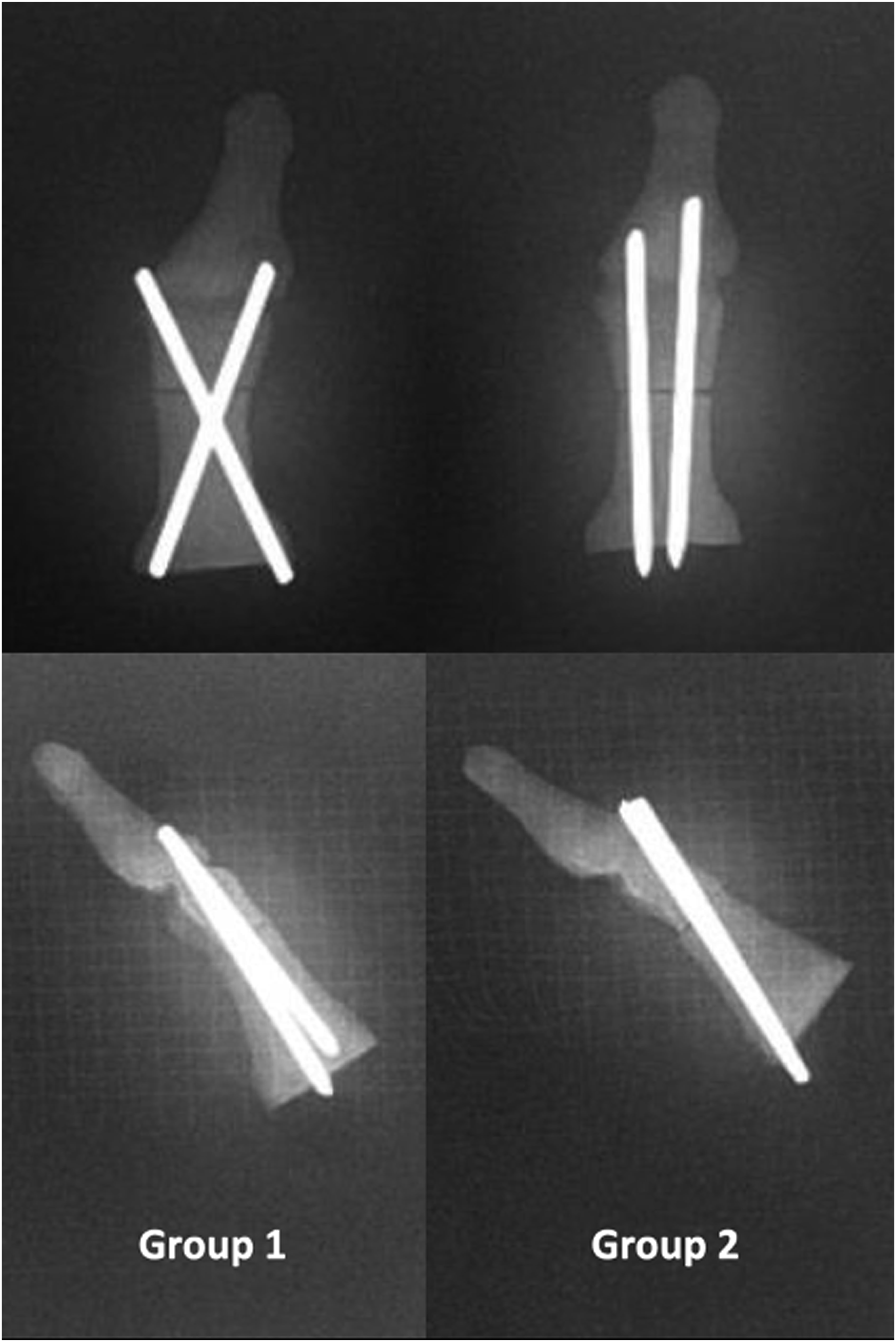
To ensure a standardized and reproducible osteotomy, a transverse line was meticulously marked 1.5 cm proximal to the interphalangeal joint before performing the procedure (Figure 1). A transverse osteotomy was then performed along the marked line using a thin-bladed saw with dimensions of 5 mm in width and 0.5 mm in thickness. To ensure standardized and repeatable fixation, measurements were taken for both cross and parallel configurations of the K-wires. After achieving anatomical reduction of the bone fragments, fixations were planned according to the predefined marks. There were 15 identical specimens in each group. In the first group, a 0.062-inch (1.6 mm) K-wire (TST, Istanbul, Turkey) was placed from the distal medial to the proximal lateral aspect of the proximal phalanx. A second K-wire of the same dimensions was then inserted in a cross configuration, extending from the distal lateral to the proximal medial aspect of the proximal phalanx. In the second group, fixation was achieved using two 0.062-inch K-wires arranged in a parallel configuration, extending from the distal dorsal to the proximal volar side of the proximal phalanx, with a distance of 1 cm maintained between them (Figure 2). Fixations for both groups were verified using radiographs (Figure 3). All of these factors created uniform and standardized conditions for biomechanical comparison. Additionally, osteotomy, fixation, measurement, and all other procedures conducted on composite models were carried out by the same investigators to ensure consistency throughout the study. All specimens were marked transversely 1.5 cm proximal to the interphalangeal joint before the osteotomy. After the standard osteotomy was applied to all specimens, the fragments were reduced, and fixed in a uniform and standardized manner in both parallel and cross configurations over the predetermined marks. All specimens were checked with radiographs to ensure standardization.

Biomechanical tests
Mechanical tests, similar to the flexion test at three support points used by Ibanez et al. (2015) and Unal et al. (2010), as well as the bending tests conducted by Chacon et al. (2012) and Witkowski et al. (2021), were performed to simulate the normal physiological loads on the proximal phalanx of the first toe, both at rest and under load.14–17 These tests were carried out on Sawbone models that simulated transverse fractures of the proximal phalanx in specimens from groups 1 and 2. The experiments were conducted by an engineer with over 10 years of experience in biomechanics and bioengineering at the Department of Biomechanics, Dokuz Eylul University.
In the bending test, each specimen was secured 1 cm proximal to the osteotomy line at a 15-degree inclination angle to the testing machine. This setup simulates the position of the hallux relative to the ground during normal posture.
15
A gradual load was applied from the plantar surface, 1 cm distal to the osteotomy line (Figure 4). In the flexion test at three support points, the first toe was positioned on the experimental setup with its dorsal surface parallel to the ground. Support was provided at two points on the dorsal surface: 1 cm proximal and 3 cm distal to the osteotomy line. At the third point, located 5 mm distal to the osteotomy line, a progressive load was exerted from the plantar surface (Figure 5). The load was applied to the bone models perpendicularly to the ground using a mechanical testing machine (Shimadzu AG-I 10KN, Japan). As in the related studies, a compression rate of 100 mm/min was applied using the test device, simulating physiological loading.
17
Data such as the amount of displacement, applied force, and stiffness were recorded by the computer connected to the test device. In the bending test, the specimens were fixed to the testing machine at a 15-degree angle to the ground plane, 1 cm proximal to the osteotomy line. A gradual load increase was applied from 1 cm distal to the osteotomy line and from the plantar surface. In the flexion test at three support points, the toe was placed on the testing machine from the dorsal surface, parallel to the ground. The support points were located 1 cm proximal and 3 cm distal to the osteotomy line. A gradual load increase was applied from 5 mm distal to the osteotomy line and from the plantar surface.

In similar studies, a displacement of 2 mm was associated with nonunion.18–20 For this reason, the load was progressively increased using the test machine until a displacement of 2 mm was reached, and the force required to achieve this displacement was recorded. Additionally, as in similar studies, the deterioration of the specimen structure, such as cortical fractures and implant failures in bone models due to increased loads, was considered a failure.15,17 The amount of force and displacement at the point of failure was documented. All procedures performed on the samples were documented through photographs and videos.
Statistical analysis
The findings of the study were analyzed using IBM SPSS Statistics 22 (IBM SPSS, Turkey). The Shapiro-Wilk test was conducted to assess the normality of the data distribution. To compare quantitative data and non-normally distributed parameters between the two groups, the Mann-Whitney U test was applied. Statistical significance was determined at a p-value threshold of <0.05.
Results
In this study, we utilized two distinct experimental setups involving a total of 30 samples, evenly divided into 15 CC fixations and 15 PC fixations. The flexion test at three support points, achieved successful results across all samples in the setup with 8 CC and 8 PC fixations. Conversely, in the bending test setup, which included 14 samples, we experienced some challenges. Specifically, 2 samples one CC and one PC were lost during testing. Nonetheless, the bending test was successfully completed with the remaining 12 samples.
Values from the bending test.

Values from the flexion test at three support points.

Evaluation of bending test parameters between groups.

Mann Whitney U Test *p < 0.05.
Evaluation of flexion test at three support points parameters between groups.
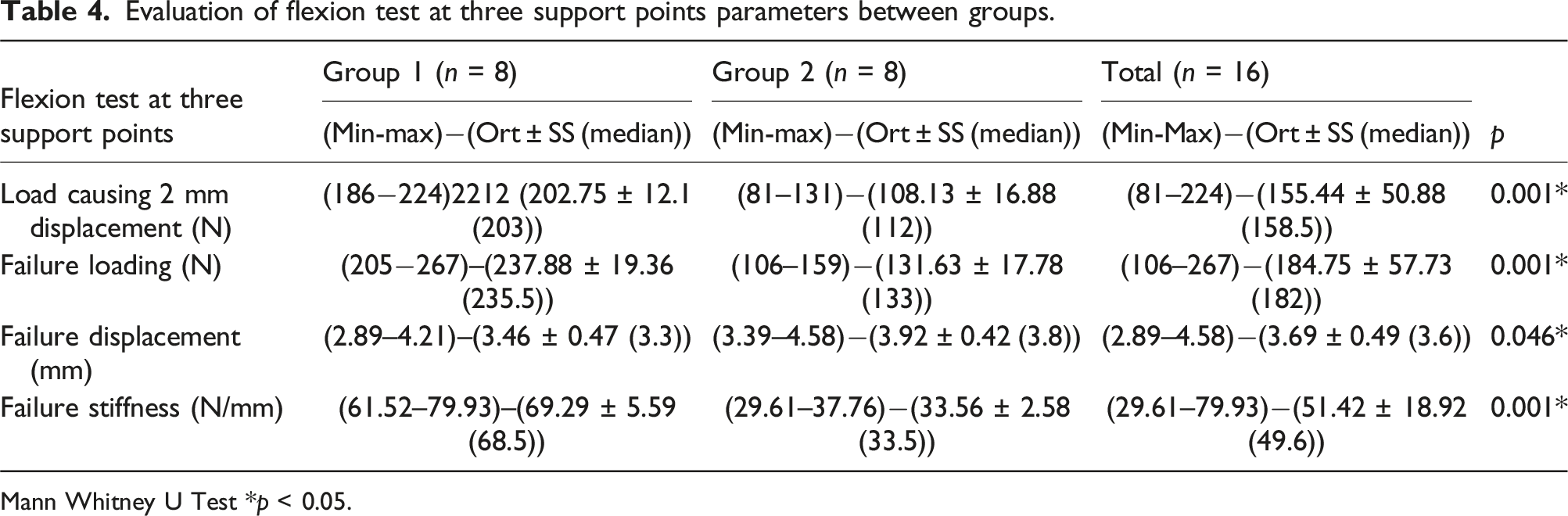
Mann Whitney U Test *p < 0.05.
In both the flexion test at three support points and the bending test setups, Group 1 exhibited statistically significantly higher values for the load causing 2 mm displacement, the maximum load during failure, and stiffness compared to Group 2. Additionally, the displacement value at failure was statistically significantly lower in Group 1 than in Group 2 (p < 0.05 for all).
Discussion
This study’s primary findings are summarized as follows: In both experimental setups, Group 1 demonstrated significantly higher force measurements at both the 2 mm displacement of the osteotomy line and at the point of failure compared to Group 2. Additionally, the displacement value during failure was significantly lower in Group 1 than in Group 2. Furthermore, Group 1 exhibited significantly greater stiffness values than Group 2. These results highlight the superior biomechanical performance of Group 1, indicating more effective fixation and structural integrity under the tested conditions.
To ensure the accuracy of the data, our study aimed to control for variables such as bone quality, fracture geometry, fracture reduction, and implant selection factors known to influence the mechanical efficiency of internal fixation and the focus was placed on the positioning of the implant. The use of Sawbones materials was chosen to standardize the models in terms of bone density, shape, and size, thereby minimizing variability and ensuring consistent conditions across all specimens. 21 Heiner’s study demonstrated that synthetic bone models generally matched real bone in terms of overall structural rigidity. 22 However, Quenneville et al. identified discrepancies between synthetic and real bone when evaluating impact resistance. 23 This disagreement may stem from the use of heterogeneous cadaver bone samples from elderly donors in hardness evaluations. Synthetic specimens represent high-quality bone and do not have the defects, inconsistencies, or morphological differences found in real cadaveric specimens. Therefore, synthetic bone models were preferred over donor bones for the current study to ensure consistency and accuracy.
Fractures that are initially managed conservatively but become displaced during follow-up should be treated surgically. 24 K-wire application, which is one of the minimally invasive methods, can be preferred primarily due to its cost-effectiveness, simple percutaneous application, low hospital stay, low surgical complications such as minimal tissue damage.24,25 Additionally, to prevent progressive soft tissue damage and potential infection in open or crush-type toe fractures, it is recommended to stabilize the fracture using temporary percutaneous K-wires after wound debridement and washout in the operating room, rather than opting for permanent implants and extensive incisions.24,26 Minimizing the use of materials on the toes significantly helps in reducing the risk of implant related complications. For this reason, K-wire fixation following closed reduction offers the advantage of stabilizing the fracture while minimizing tissue damage.24,27 However, displacement between fracture fragments can occur in some patients during follow up. This issue may arise because K-wires are often applied in various configurations for fixation. In the current study, we aimed to identify which K-wire configurations are biomechanically more stable and durable by applying different configurations in equal numbers and under consistent conditions. The results indicated that the CC configuration was more durable and stable compared to the PC configuration.
The stability of the fixation is critical for the revascularization and healing processes of the bone. 28 In a biomechanical study by Lee et al., supracondylar humerus fractures were stabilized using either two crossed K-wires or two parallel K-wires. The study demonstrated that crossed K-wires provided greater stability than parallel wires in tests involving varus, valgus, extension, and rotational forces. 29 In another study involving pediatric patients with supracondylar humerus fractures, no significant difference in clinical stability was observed between fixation with two parallel lateral pins and cross pinning with one wire from the medial side and one from the lateral side. 30 In another biomechanical study on synthetic scaphoid bones, a perpendicular osteotomy was performed along the long axis of the scaphoid, with fixation achieved using two parallel and two crossed K-wires. 31 The study demonstrated that the crossed K-wire configuration provided greater stability against vertically applied forces to the distal pole of each scaphoid. Our study was conducted on the first toe. Although the physiologically acting forces differed, our findings demonstrated that the cross-wire configuration provided more stable fixation, consistent with the studies by Lee et al. 29 and Gökçe et al. 31
During normal walking, the load under the hallux can be up to 25% of body weight. 32 In a male patient with an average body weight of 784 N, the minimum load that the fixation at the hallux should support for weight bearing is 196 N. 33 A higher load capacity than the specified value provides greater confidence in the load-bearing ability of a fixation method. Additionally, some studies used a threshold value of 2 mm as a failure criterion for displacement between bone fragments, with values exceeding this threshold interpreted as non-union.34,35 In our study, CC K-wires demonstrated remarkable stability, with no displacement beyond 2 mm even under forces exceeding the specified threshold. In contrast, PC K-wires failed at lower load values. Specifically, PC K-wire fixation failed in both test setups before reaching the load values experienced by the hallux during normal gait. This finding indicates that PC K-wire fixation does not adequately support full weight-bearing in the early postoperative period. Our in vitro study, where the test machine does not affect the fracture but only the implants, shows that CC K-wires offer superior biomechanical stability compared to PC K-wires. The CC K-wires remained stable and sufficient for load-bearing even with up to 2 mm of displacement. Consequently, we believe that patients with hallux proximal phalanx fractures treated with CC K-wires can safely begin weight-bearing once soft tissue edema subsides. These biomechanical findings encourage us to further explore clinical applications and additional research to validate and expand upon these results.
This study has some limitations. First, it is difficult to simulate the in vivo conditions of human bone, although composite bones can mimic normal human bones and seem to be a good option for making a standard biomechanical comparison. Additionally, studies with real patients or cadavers more accurately reflect clinical data. Only bending force and the flexion force at three support points were applied to the samples using the biomechanical test machine in this study. However, hallux fractures are exposed to varus or valgus forces, albeit slightly, during healing. Although statistically consistent and significant results were found within and between groups in this biomechanical study, it is important to add more samples rather than relying on a limited number to obtain more accurate data. As a final limitation, the estimated value of the load carried by the hallux was derived from values reported in other studies.
Conclusion
In conclusion, this study demonstrated that CC K-wires offer superior stability and reliability compared to PC K-wires in terms of force resistance and load-bearing capacity for the fixation of experimentally created osteotomy lines in synthetic proximal phalanx bone of the hallux. CC K-wires proved adequate for load-bearing after fixation, whereas PC K-wires were found to be inadequate. The findings of this study may serve as a foundation for future research on biomechanical gait and segmental foot kinematics. To further validate and support these results, additional studies involving clinical applications and cadaveric bone are necessary.
Footnotes
Author contributions
SK: Main author of manuscript, Study design. BK: Study design, Data collection and analysis. MC: Data collection and analysis. MYA: Data collection and analysis. BU: Study design. FE: Study design, Data collection and analysis. DG: Interpretation of study material, Senior author. CE: Interpretation of study material, Senior author. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.