
Abstract
Purpose
To examine the effects of tourniquet use in arthroscopic anterior cruciate ligament reconstruction in terms of (1) intraoperative visualization, (2) surgical time, (3) consumption of sterile saline, and (4) postoperative pain.
Methods
In this prospective randomized clinical trial, patients were assigned to Tourniquet Group or No Tourniquet treatment groups. The primary outcomes were intraoperative visualization, with scores ranging from 0 to 10 (0 = no visibility; 10 = clear and perfect display), surgical time, and the consumption of sterile saline. The secondary aim was to measure postoperative pain (24 h after surgery) with the visual analog scale (VAS) for pain.
Results
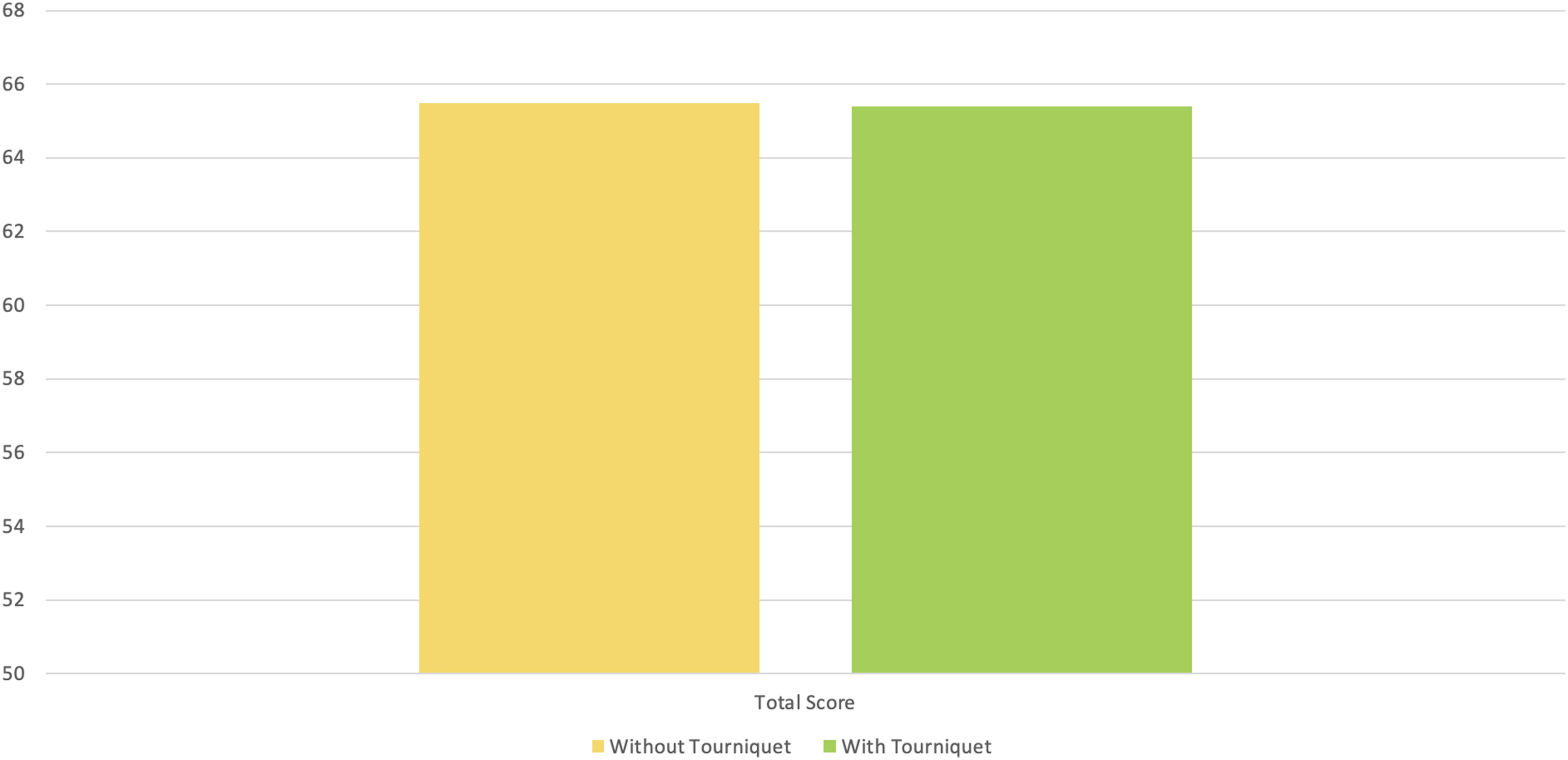
A total of 71 patients were included in the No Tourniquet group, and 75 were included in the Tourniquet group, with mean ages of 26.73 ± 8.05 years and 26.95 ± 10.11 years, respectively (p = .88). In the No Tourniquet group, 37 concomitant meniscal lesions were treated, whereas in the Tourniquet group, 38 (p = .99) were treated. The mean surgical times were 51.07 ± 6.90 and 50.03 ± 7.62 (p = .325), respectively, while the mean amount of saline consumed was 6.17 ± 1.18 L versus 5.89 ± 1.23 L (p = .217). Both groups achieved optimal visualization, with a sum of all surgical steps of 65.49 ± 1.86 for the no tourniquet group and 65.39 ± 1.88 for the Tourniquet group (p = .732). Postoperative pain was significantly lower in the No Tourniquet group (VAS score: 2.82 ± 1.33 vs 5.80 ± 1.22).
Conclusions
Tourniquet use during ACL reconstruction does not improve intraoperative visualization and does not reduce surgical time but leads to greater postoperative pain with a risk of well-known tourniquet-related complications.
Level of evidence
Level I – Randomized clinical trial.
Introduction
The utilization of a tourniquet was initially suggested in 1904 and has since become a customary practice in surgical procedures. The effects of a tourniquet can be attributed to its ability to increase visibility in the surgical field, increase procedural accuracy, and reduce surgical time. The technique has been employed in several patient cohorts, such as those receiving total knee arthroplasty and foot and ankle surgery. Using a tourniquet has been shown to effectively decrease the amount of blood lost during surgery and lower the risk of blood clot formation in total knee arthroplasty. Additionally, it has been found to dramatically reduce the duration of hospital stay in foot and ankle surgery. 1
Nevertheless, the application of a tourniquet carries inherent dangers such as thigh pain, a heightened need for pain relief medication, muscle injury, increased bleeding from drainage tubes, and the development of deep-vein thrombosis (DVT). Hence, it is imperative to exercise caution and possess adequate expertise when utilizing it. Tourniquets are currently used in arthroscopic knee surgery, namely, in routine procedures such as meniscus repair and ACL reconstruction. However, their usage relies on the surgeon’s preference, and conflicting results have been reported from various techniques. 2
While numerous clinical studies have examined the impact of tourniquet application on results after surgery involving the upper and lower limbs, only a limited number of studies have specifically investigated its effect on postoperative outcomes in ACL reconstruction. In their randomized controlled experiment, Reda et al. demonstrated that the use of a tourniquet during ACL reconstruction leads to increased levels of discomfort and knee hemarthrosis after surgery. 3 However, they also reported that the impact of the tourniquet on muscle strength is only brief. 3 A study conducted by Arciero et al. and Rorabeck and Kennedy revealed a negative impact of tourniquet application on muscular performance in the early postoperative period. However, no significant change was observed after 6 months.4,5
In a recent study, Nagashima et al. examined the occurrence of DVT after ACL reconstruction with and without the use of a tourniquet. They discovered that ACL reconstruction performed without a tourniquet resulted in a significantly lower incidence of DVT and less postoperative drainage than ACL reconstruction performed with a tourniquet. 6
The aim of the present study was to examine the effects of tourniquet use in arthroscopic anterior cruciate ligament reconstruction in terms of (1) intraoperative visualization, (2) surgical time, (3) consumption of sterile saline, and (4) postoperative pain.
Methods
Study design and patient inclusion
The present study was approved by our Institutional Ethics Committee (institutional review board ACL (L2104)). The datasets used and/or analyzed during the current study are fully available upon reasonable request. We conducted a prospective, randomized, controlled trial to assess the effect of tourniquet use on patients who were assigned to undergo ACL reconstruction via a 4-strand hamstring autograft. The included subjects were all patients who had undergone unilateral primary ACL reconstruction under subarachnoid anesthesia and who were aged older than 16 years. Patients with bilateral knee injury, other knee ligament injuries (such as anterolateral ligament injury, posterior cruciate ligament, medial collateral ligament, or lateral collateral ligament), or a history of previous knee surgeries were excluded. Concomitant meniscal treatment (meniscectomy or meniscal repair) was not considered an exclusion criterion. Patients with contraindications to tourniquet use or symptomatic peripheral vascular disease were also excluded. Patients with allergies or with systemic disease that presented contraindications to tranexamic acid, mepivacaine or adrenaline were also excluded.
The patients were randomized into two groups: those who underwent ACL reconstruction with the tourniquet inflated (Tourniquet group) and those with the tourniquet not inflated (No Tourniquet group).
A total of 192 patients were assessed for eligibility. Overall, 46 patients were excluded: 35 because of the present exclusion criteria (20 with concomitant anterolateral ligament reconstruction, 4 with concomitant medial or lateral collateral ligament reconstruction, and 11 with previous surgery to the affected knee) and 11 because they refused to participate.
Thus, 146 patients were included in the study; 75 patients were randomized to surgery with a tourniquet, and 71 were randomized to surgery without a tourniquet but with a local injection of adrenaline and mepivacaine. All patients provided written informed consent for participation in this study, which was approved by the ethics committee of our hospital. A flowchart of the Consolidated Standards for Reporting Trials (CONSORT) is shown in Figure 1.
7
Randomization and allocation of the patients included in the study according to Consort Flow Diagram.
Randomization
Injection details for both groups.
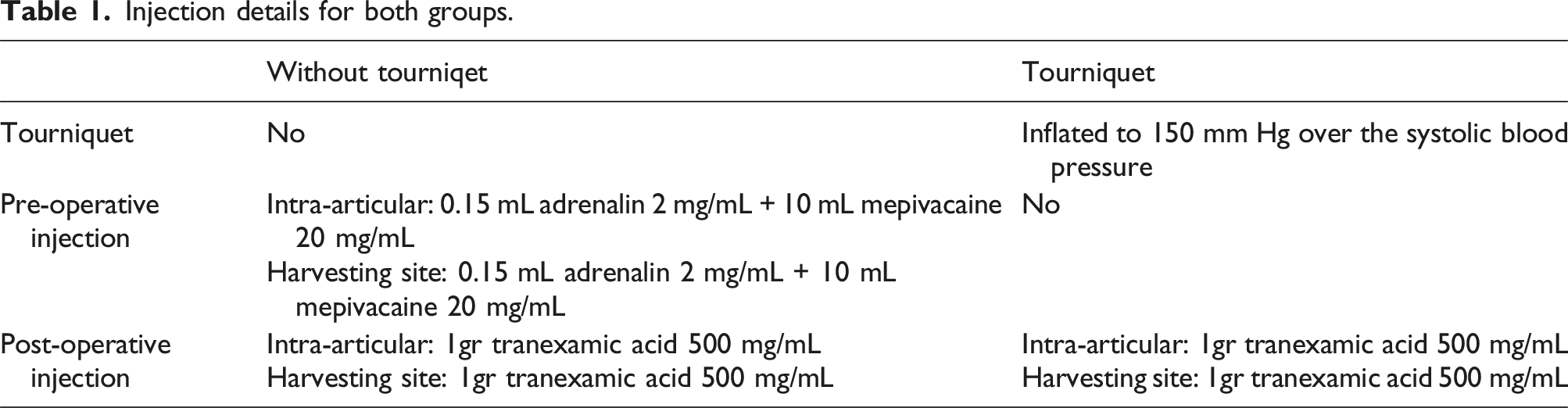
Surgical technique
All patients underwent the same surgical procedure: the distal pes anserinus was lifted with a small “L”-shaped incision. The hamstrings were extracted via a tendon stripper. The tendons were measured and mixed with saline and one g of vancomycin. The tendon was prepared and folded twice and hung on the ULTRABUTTON device. The graft was marked with a stitch at the same point as the half-tunnel femoral length. A far medial portal was created. With the knee flexed at 90°, a 7-mm reamer is introduced from the far medial portal to reach the desired anatomic femoral insertion. Once the desired position has been reached, the knee is flexed to 120°. With the knee at 120° and the reamer at the desired point, a Kirschner wire is introduced through the reamer. The 7-mm reamer is removed, and we proceed with half-tunnel creation. The size of the femoral half tunnel is usually 20 to 25 mm. After this step, the 9-mm drill is removed, and a 4.5 mm drill is used to mill the entire femur up to the lateral cortex. The knee was placed again at 90° of flexion. The tibial ACL guide was set at 55° and then introduced through the anteromedial portal. The tibial tunnel was established, starting with a 6-mm reamer and then upsizing to a 9-mm reamer once the position was confirmed. The transport wire is retrieved from the tibial tunnel with a grasper. At this point, the graft was introduced into the transport wire and passed through the tibial and femoral tunnels. 8
Postoperative management
All patients received the same standardized postoperative rehabilitation protocol and pain-control program. We administered 4000 U of enoxaparin starting 8 h after surgery. Intraoperatively and after surgery, patients received paracetamol (1 g) every 8 h and ketorolac after 12 and 24 h. 9
Patients were discharged the day after surgery and followed the same rehabilitation protocol with immediate weight-bearing and full range of motion, as well as crutches for balance and comfort, until the patients could walk confidently without limping.
Outcome assessments
Intraoperative assessment
The primary outcomes were intraoperative visualization (divided into seven different surgical methods: suprapatellar; medial compartment; lateral compartment; central pivot; femoral tunnel; tibial tunnel; and graft passage), with scores ranging from 0 to 10 (0 = no visibility; 10 = clear and perfect display), surgical time (from the moment of the skin incision to the time of suturing), and the consumption of sterile saline measured in liters. An assessment of visualization was performed during surgery by an assistant who was not involved in the surgery and was not aware of the patient assignment group; furthermore, a second analysis was performed by looking at videos recorded by another assistant.
Clinical assessment
The secondary aim was to measure postoperative pain (24 h after surgery) with the visual analog scale (VAS) for pain. Ranging from 0 to 10, with greater scores indicating greater pain intensity. A score of 0 indicated no pain; a score of one to three indicated mild discomfort; a score of four to six indicated moderate pain; and a score of 7 to 10 indicated severe pain. VAS evaluations were performed by an orthopedic surgeon not involved during surgery. 10
Sample size
An estimated sample of 142 subjects, 71 for each group, were required to compare surgical time between groups with a two-sided t test, assuming a mean difference of 5, standard deviations of 5.5 and eight for the groups with and without a tourniquet, a 5% alpha, and 99% power, respectively. Additional subjects were recruited to ensure statistical significance in cases of adverse events.
Statistical analysis
Summary statistics are presented overall and by groups of patients with and without a tourniquet as the means and standard deviations (SDs) or absolute frequencies and percentages. After the distribution of continuous variables was tested, a t test or a Wilcoxon‒Mann‒Whitney test was performed to assess the mean differences between groups, whereas differences between categories were assessed with the chi-square test or Fisher’s exact-test. To assess whether the groups differed in terms of the VAS score, saline consumption, surgical time and intra-articular visibility, t tests or nonparametric Wilcoxon‒Mann‒Whitney tests were performed. Subgroup analyses by sex and age (above and below the rounded average value) were also performed. All tests were two-sided, and a p value less than 0.05 was considered statistically significant. Statistical analyses were conducted in R version 4.1.1.
Results
Demographic data.

Intraoperative outcomes
No difference between the two groups was found in terms of visibility at each stage of arthroscopy, total visibility score, or saline consumption (p > .05) (Figures 2–4). Mean surgical time in minutes of the two groups (without and with tourniquet). Visual Analogue Scale for Pain and Saline Consumption of the two different groups analyzed in the study (without and with tourniquet). Analysis of total score visibility between the two groups (without and with tourniquet).

Comparison of surgical time, saline consumption, pain and visibility.

aStatistical significant value.
All subanalysis groups presented similar results, with a significant difference in pain score only (p < .05). The details of the subanalysis are reported in Appendix 1.
Discussion
The most important findings of the present study are that the use of a tourniquet during anterior cruciate ligament reconstruction does not improve intraoperative visibility, does not reduce surgical time or lead to greater pain in the short term after surgery.
Currently, many studies have analyzed the use of tourniquets and their impact on ACL reconstruction, with contrasting results.
Zaid et al. examined the effects of tourniquet use in arthroscopic ACL reconstruction in terms of intraoperative visualization with respect to operative time and the consumption of sterile saline, intra- and postoperative blood loss, postoperative pain, opioid consumption, swelling, serum creatine phosphokinase (CPK) and hemoglobin (HB) concentrations, clinical outcomes, and graft healing. Intraoperative visualization was satisfactory in 100 of 100 patients in the tourniquet-up group and 64 of 100 patients in the tourniquet-down group (p < .05). The mean operative time was 58.4 min in the tourniquet-up group and 72.5 min in the tourniquet-down group (p < .05). The mean sterile saline consumption was 6.4 L in the tourniquet-up group and 8.7 L in the tourniquet-down group (p < .05). The respective amounts of estimated intraoperative and postoperative blood loss were 95.3 mL and 240.3 mL, respectively, in the tourniquet-up group and 230.2 mL and 75.6 mL, respectively, in the tourniquet-down group (p < .05). The results revealed no significant differences in postoperative pain, opioid consumption, percentage of patients using opioids, swelling, mean serum CPK and Hb levels, subjective and objective functional scores, or graft healing between the two groups. 11
Similarly, Nagashima et al. compared total perioperative blood loss and soft tissue damage with and without tourniquet use during ACLR and reported no advantage for not using a tourniquet in terms of blood loss or soft tissue damage. 12
Hao et al. evaluated the degree of tourniquet-induced ischemia via noninvasive continuous real-time monitoring and the relationship between changes in tissue oxygen saturation (StO2) and blood biochemical markers of ischemic injuries in patients undergoing arthroscopic knee surgery. 13 Data were collected from 29 consecutive patients who underwent arthroscopic procedures. Twenty-five patients underwent anterior cruciate ligament reconstruction, and four underwent meniscal repair. We investigated tourniquet‐induced changes in StO2, which were monitored via NIRS, and blood biochemical markers of ischemic injury. A significant decrease in the mean StO2 from the baseline was observed during tourniquet inflation in the operative legs. The average decrease in the mean StO2 was 58%. A comparison of the mean StO2 between the nonoperative and operative legs before tourniquet deflation revealed that the mean StO2 in the operative legs was significantly lower than that in the nonoperative legs. No significant clinical relationships were detected between changes in StO2 and blood biochemical markers of ischemic injury (creatine kinase) (p = .04, r = 0.38) or tourniquet duration (p = .05, r = 0.366). 13
The use of a tourniquet can also lead to deep vein thrombosis; in fact, previous studies have reported a wide range of DVT incidence rates, depending on whether asymptomatic DVT was included. 6 A recent notable study reported that the incidence of venous thromboembolism was 0.4% after ACL reconstruction. Because their study was based on a large registry database, only symptomatic complications were investigated. 14 However, Struijk-Mulder et al. reported a 13% incidence of DVT via ultrasonography: 9% with asymptomatic DVT and 4% with symptomatic DVT. 15 Sun et al. also confirmed a high percentage of silent DVT after arthroscopic knee surgery via venography. Given that the natural history of asymptomatic DVT is still unclear, thromboprophylaxis protocols for ACL reconstruction should be established in consideration of asymptomatic DVT. 16
Joo et al. assessed the true incidence of DVT after ACL reconstruction via a tourniquet, regardless of symptom manifestation. A total of 21 (8.1%) patients had DVT. Five (1.9%) patients had thrombosis at the popliteal vein; however, none of them exhibited symptoms. The other 16 patients had thrombosis at the distal veins: one patient at the anterior tibial vein, five patients at the posterior tibial vein, three patients at the peroneal vein, six patients at the soleal vein, and one patient at the muscular branch vein. The risk factors for proximal DVT included high-energy direct injury (p = .013, odds ratio = 10.62) and grade 2 soft tissue injury (p = .039, odds ratio = 6.78). 17
The use of a tourniquet can also benefit muscle strength and function, whereas other investigations have reported that ACLR with the use of a tourniquet has no effect on strength or function after rehabilitation.
In 2022, Beynnon et al. determined whether the duration of tourniquet use during ACLR affects knee extensor muscle contractile function and size at the cellula level 3 weeks after surgery and at the whole-muscle level at 6 months after surgery. The authors reported that the duration of tourniquet use at the time of ACLR surgery did not explain the variation in muscle fiber size, contractile function, or mitochondrial content at 3 weeks after surgery or the strength of the quadriceps musculature or patient-reported function or quality of life at the 6-months follow-up. 18
To reduce pain and bleeding, our protocol involves the use of intra-articular and pes anserinus with adrenaline and mepivacaine and, at the end of surgery, with local tranexamic acid.
The use of tranexamic acid has been seriously debated for its potential chondrotoxicity. Na et al., in their systematic review, suggested that tranexamic acid administration at the time of ACLR results in decreased intra-articular bleeding (measured via a drainage system), hemarthrosis grade, and pain compared with the control. 19
Similarly, Alkhatib et al. reported that the use of tranexamic acid in ACLR reduces the need for aspiration, hemarthrosis, drain output, and knee swelling in the postoperative period. While early improvements in pain and function were observed, the clinical relevance of these findings is questionable. The risk of complications does not increase with tranexamic acid use, and the use of intravenous tranexamic acid over intra-articular tranexamic acid may improve and prolong hemarthrosis reduction, although the evidence is weak. 20
For chondrotoxic effects, Caglar et al. assessed the effects of tranexamic acid on the articular cartilage, anterior cruciate ligament, and joint capsule of the knee. Histologically, intravenous tranexamic acid damages the articular cartilage and ACL more than intra-articular tranexamic acid does. The intra-articular administration of tranexamic acid is more protective when the articular cartilage and ACL are preserved. 21
The intra-articular administration of local anesthetics, either alone or in conjunction with other drugs, is commonly regarded as a standard and secure clinical procedure. However, a significant number of patients with unusual acute chondral damage and degradation, known as joint chondrolysis, have been reported.22,23
In our experience, we never reported cases of chondrolysis due to lidocaine or adrenaline intra-articular administration; similar to our results, Ravnhiar et al. evaluated the in vivo effect of a single intra-articular injection of the local anesthetic (la) lidocaine on the viability of articular cartilage in intact or osteoarthritic (Oa) human knees and measured the synovial postinjection concentration of lidocaine in the knee. 24
This study revealed that a single intra-articular knee injection of 2% lidocaine did not influence chondrocyte viability in either healthy or Oa cartilage. A rapid decrease in the synovial La concentration (more than 40 times greater) is the most likely protective mechanism. 24
The reduced level post-operative level of pain can be a factor in return to sport after ACL reconstruction; in fact, approximately 82% of persons resumed some degree of sport involvement after ACLR. However, between 43% and 63% of patients did not regain their pre-injury levels of sport, indicating a decrease in overall physical activity adherence. Limited evidence exists to establish the correlation between physical activity and knee function in persons after anterior cruciate ligament reconstruction ACLR, however a decrease in physical activity may be associated with the onset of impaired knee function. 25
Our study had several limitations that should be acknowledged. First, this study was a single-institution, randomized controlled trial, and the groups were similar in their baseline characteristics. Second, only very short-term follow-up was considered. Third, the postoperative development of hemarthrosis is a concern in ACLR but was not evaluated in this study. Fourth, indicators of soft tissue damage were not recorded.
Conclusions
Tourniquet use during ACL reconstruction does not improve intraoperative visualization and does not reduce surgical time but leads to greater postoperative pain with a risk of well-known tourniquet-related complications.
Footnotes
Acknowledgments
None
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Code availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethical statement
Data availability statement
The raw data are available upon reasonable request to the corresponding author.
Appendix
Subgroup analysis
Female (N = 42)
Descriptives
Without tourniquet
With tourniquet
p-value
Age, mean ± SD
28.06 ±8.35
27.85 ±11.54
0.931
Lesion
No
5 (33.3)
11 (40.7)
0.887
Yes
10 (66.7)
16 (59.3)
Side
Right
6 (40.0)
13 (48.1)
0.853
Left
9 (60.0)
14 (51.9)
Score
Without tourniquet
With tourniquet
p-value
Surgical time
49.47 ± 5.21
50.00 ± 7.52
0.989
Visual Analogue Scale for Pain
3.27 ± 1.22
5.96 ± 1.26
<0.001*
Saline Consumption
5.93 ± 1.03
5.81 ± 1.36
0.925
Visibility
Suprapatellar
9.27 ± 0.80
9.26 ± 0.76
0.930
Medial Compartment
9.27 ± 0.80
9.37 ± 0.63
0.773
Lateral Compartment
9.20 ± 0.77
9.26 ± 0.66
0.863
Central Pivot
9.53 ± 0.52
9.48 ± 0.58
0.845
Femoral Preparation
9.27 ± 0.80
9.30 ± 0.54
0.907
Tibial Preparation
9.53 ± 0.64
9.44 ± 0.64
0.635
Graft Passage
9.20 ± 0.86
9.33 ± 0.83
0.566
Score total
65.27 ± 2.05
65.44 ± 1.87
0.777
Male (N = 104)
Descriptives
Without tourniquet
With tourniquet
p-value
Age, mean ± SD
26.41 ± 7.95
26.56 ± 9.11
0.928
Graft
Hamstring
56 (100.0)
48 (100.0)
-
Lesion
No
29 (51.8)
26 (54.2)
0.964
Yes
27 (48.2)
22 (45.8)
Side
Right
30 (53.6)
26 (54.2)
>0.99
Left
26 (46.4)
22 (45.8)
Score
Without tourniquet
With tourniquet
p-value
Surgical time
51.50 ± 7.26
50.04 ± 7.75
0.337
Visual Analogue Scale for Pain
2.70 ± 1.35
5.71 ± 1.20
<0.001*
Saline Consumption
6.23 ± 1.22
5.94 ± 1.16
0.210
Visibility
Suprapatellar
9.45 ± 0.63
9.50 ± 0.58
0.718
Medial Compartment
9.29 ± 0.68
9.19 ± 0.73
0.504
Lateral Compartment
9.38 ± 0.59
9.35 ± 0.60
0.871
Central Pivot
9.39 ± 0.62
9.38 ± 0.64
0.907
Femoral Preparation
9.38 ± 0.62
9.35 ± 0.70
0.994
Tibial Preparation
9.34 ± 0.61
9.31 ± 0.62
0.838
Graft Passage
9.34 ± 0.67
9.27 ± 0.61
0.500
Score total
65.55 ± 1.82
65.35 ± 1.91
0.587
Young, <26 years (N =77)
Descriptives
Without tourniquet
With tourniquet
p-value
Sex
Female
6 (17.1)
15 (35.7)
0.118
Male
29 (82.9)
27 (64.3)
Graft
Hamstring
35 (100.0)
42 (100.0)
-
Lesion
No
16 (45.7)
19 (45.2)
>0.99
Yes
19 (54.3)
23 (54.8)
Side
Right
16 (45.7)
19 (45.2)
>0.99
Left
19 (54.3)
23 (54.8)
Score
Without tourniquet
With tourniquet
p-value
Surgical time
50.51 ± 6.94
51.21 ± 7.63
0.838
Visual Analogue Scale for Pain
2.66 ± 1.35
5.69 ± 1.14
<0.001*
Saline Consumption
5.97 ± 1.12
5.86 ± 1.24
0.804
Visibility
Suprapatellar
9.51 ± 0.56
9.33 ± 0.69
0.266
Medial Compartment
9.40 ± 0.65
9.33 ± 0.65
0.633
Lateral Compartment
9.37 ± 0.65
9.26 ± 0.63
0.418
Central Pivot
9.40 ± 0.65
9.43 ± 0.70
0.741
Femoral Preparation
9.31 ± 0.68
9.33 ± 0.65
0.928
Tibial Preparation
9.40 ± 0.60
9.26 ± 0.66
0.378
Graft Passage
9.34 ± 0.68
9.07 ± 0.68
0.076
Score total
65.74 ± 1.77
65.02 ± 1.77
0.080
Old, ≥26 years (N = 69)
Descriptives
Without tourniquet
With tourniquet
p-value
Sex
Female
9 (25.0)
12 (36.4)
0.446
Male
27 (75.0)
21 (63.6)
Graft
Hamstring
35 (97.2)
33 (100.0)
>0.99
Lesion
No
18 (50.0)
18 (54.5)
0.892
Yes
18 (50.0)
15 (45.5)
Side
Right
20 (55.6)
20 (60.6)
0.857
Left
16 (44.4)
13 (39.4)
Score
Without tourniquet
With tourniquet
p-value
Surgical time
51.61 ± 6.90
48.52 ± 7.43
0.076
Visual Analogue Scale for Pain
2.97 ± 1.32
5.94 ± 1.32
<0.001*
Saline Consumption
6.36 ± 1.22
5.94 ±1.22
0.158
Visibility
Suprapatellar
9.31 ± 0.75
9.52 ± 0.62
0.243
Medial Compartment
9.17 ± 0.74
9.15 ± 0.76
0.947
Lateral Compartment
9.31 ± 0.62
9.39 ± 0.61
0.553
Central Pivot
9.44 ± 0.56
9.39 ± 0.50
0.613
Femoral Preparation
9.39 ± 0.64
9.33 ± 0.65
0.703
Tibial Preparation
9.36 ± 0.64
9.48 ± 0.57
0.449
Graft Passage
9.28 ± 0.74
9.58 ± 0.61
0.070
Score total
65.25 ± 1.93
65.85 ± 1.94
0.204