
Abstract
Objective
This study aimed to compare infection, aseptic loosening, revision, operation time, function scores, and the radiographic radiolucent line (RLL) between cementless and cemented fixation in total knee arthroplasty (TKA).
Methods
Articles reporting the outcomes of cemented and cementless TKA were searched in Medline, EMBASE, Web of Science, and the Cochrane Library. The search was conducted from articles published from January 1996 to May 2024. Odds Ratios (OR) and confidence intervals (CI) were used to measure the results. Cochrane Collaboration’s Review Manager software was used to perform the meta-analysis.
Results
Sixteen randomized controlled trials containing 2358 participants were included in this meta-analysis. Pooled data found that, in TKA, there were no significant differences between cemented fixation and cementless fixation for a prosthesis in infection, aseptic loosening and revision. The subgroup analysis and sensitivity analysis results of the knee society score (KSS) showed a significant difference favoring cementless fixation in a follow-up of less than 5 years (MD = −2.30, 95%CI –3.85 -0.74, p = .001) while favoring cemented fixation in a follow-up over 5 years (MD = 2.79, 95%CI 0.95 4.63, p = .003). The operation time of cementless was less than that of cemented (MD = 12.03, 95%CI 8.30 15.77, p < .00001). No significant difference was detected in knee society function score, Western Ontario and McMaster Universities osteoarthritis index, and RLL. There was no heterogeneity across studies (p > .1), and most studies have a low risk of bias.
Conclusions
Within a follow-up period of less than 5 years, cementless TKA had better KSS, while over 5 years, KSS was better in cemented TKA, and cementless TKA required less operation time.
Introduction
Total knee arthroplasty (TKA) is the terminal strategy for degenerative knee diseases such as osteoarthritis or chondrocalcinosis, which can efficiently release pain and improve knee function and life quality.1–3 It was predicted that by 2030, approximately 3.8 million people will undergo TKA each year in a previous study. 4 There are two different methods for prostheses fixation: cemented fixation and cementless fixation. Fixation with cement is more common and considered by some scholars to be the gold standard for TKA, but it has not yet been unified. 5 Plenty of studies about cemented TKAs have illustrated a high survival rate after long-term follow-up.1,4,6 These implants provided long-term fixation, with prosthetic survival rates ranging from 77% to 94% at 16 to 20 years postoperatively.7,8 Among the associated complications, aseptic loosening is the leading reason for implant failure in TKA. 9 However, many studies have reported results of cementless TKA, which were similar to those of cemented.10–12 Furthermore, the benefits of cementless fixation for TKA include less surgical time and no need to remove excess cement when revision is necessary. Also, beyond the above advantages is the high survival of the prosthesis in the short follow-up of below 5 years. 13
Despite constant efforts to determine which fixation is the better one for TKA, it remains unclear whether the clinical and radiological outcomes of cementless fixation are different from those of cemented fixation. The previous meta-analyses showed no significant differences in outcomes between cemented fixation and cementless fixation, but they included some low-quality cohort research or a few randomized controlled trials (RCT) among which some are repeat studies, which may cause certain bias in those meta-analyses.11,12 Accordingly, this study aimed to conduct a meta-analysis including newly published high-quality RCTs not included in previous meta-analyses to evaluate the clinical and radiological differences between the cemented fixation and the cementless fixation in patients undergoing TKA. Based on the controversy found in the previous studies, it was hypothesized that there is no difference in clinical and radiological outcomes between cemented and cementless fixation. This meta-analysis was registered in PROSTERO (CRD42023387271).
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), the 2020 PRISMA checklist was illustrated in Supplemental Table 1.
Literature search
Electronic databases including PubMed, EMBASE, Web of Science, and the Cochrane Library, were used to search related studies published from January 1996 to May 2024. Two investigators (ZL and LW) conducted the search independently. All studies included are English-language publications. Planned, ongoing, or unpublished trials were also searched by hand. When there is insufficient information in the study, contact the research author to obtain relevant data. The study selection followed PICO algorithm (Population-Patients who underwent total knee arthroplasty; Intervention- Cemented fixation of the prosthesis; Comparison- Control group; Outcome- Clinical and radiological outcomes after TKA).
Inclusion and exclusion criteria
The inclusion criteria: (1). Participants: patients who underwent TKA with the diagnosis of osteoarthritis or chondrocalcinosis. (2). Intervention: cemented or cementless fixation for the prosthesis. (3). Study design: full-text RCTs. (4). Outcomes: reporting at least one of the outcomes. And the exclusion criteria are as follows: (1). TKA for revising and complicated TKA; (2). Case reports, basic research, and conference papers; (3). Incomplete data, unreproducible data, and statistical errors; (4). Duplicate publications or secondary publications.
Selection of the literature
Two independent investigators (ZL, LW) assessed whether the study could be included, they scanned the titles and abstracts of each study. Then, selected randomized controlled trials that might be relevant according to inclusion and exclusion criteria. When divergences occurred, all authors discussed until they reached a consensus.
Data extraction
The aimed data from the included studies were extracted by two independent authors (ZL, LW). The baseline of included studies contained the following information: sample size, age, gender, BMI, outcome measures, intervention, and follow-up. Contact the authors to obtain the unclearly relevant data when necessary. When divergences occurred, all authors discussed until they reached a consensus.
Outcome assessment
The clinical evaluation included the Range of Motion (ROM), 14 the Knee Society Score (KSS), 15 and the Western Ontario and McMaster Universities osteoarthritis index (WOMAC), 16 Knee Society Function Score (KSFS), 17 revision, 18 infection, 19 operation time, and aseptic loosening. 20 The radiological outcome was radiolucent lines (RLL), 21 which means radiographic observation of the interface between bone and cement for cemented component or between bone and prosthesis for cementless component.
Risk bias and quality assessment
Two investigators (LZ, LW) evaluated the risk of bias of the included RCTs independently using the Cochrane collaboration tool, 22 focusing on random sequence generation, allocation concealment, blinding of outcome assessment, blinding of participants and personnel, incomplete outcome data, selective reporting, and other bias. Each item above was classified into high (H), low (L), and unclear (U) according to the risk of bias. Quality assessment was performed using Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria. To assess the publication bias of each included outcome, the egger’s test was performed, and funnel plots were generated. Two independent investigators (ZL, LW) assessed all the included studies. When any controversies occurred, discussed with a 3rd author (LZ) until consensus.
Statistical analysis
Forest plots and funnel plots were generated by the Review Manager Software Package (RevMan Version 5.3, The Cochrane Collaboration, Copenhagen, 2014). The stata 16.0 was used to perform the egger’s test. When p < .05, the publish bias exists. GRADEpro Guideline Development Tool (GDT) online (https://gradepro.org/) was used to carry out GRADE assessment. Cochrane Q test and the I2 index were utilized to determine the heterogeneity. 23 And the random-effects model will be used when the evaluation of heterogeneity is significant (I2 >50%, p < .10). When the p > .10 or I2 <50%, the heterogeneity is not significant, then the fixed-effect model was applied to calculate the pooled effect. When existed, the heterogeneity was identified and explained using a subgroup analysis and sensitivity analysis using RevMan 5.3; The random-effects model would be used to merge the data when the source of heterogeneity cannot be determined. 24
Results
Search results
The initial literature search yielded a total of 1862 articles. After titles and abstracts screening, according to the inclusion criteria and exclusion criteria, 119 articles remained available. After articles that were not RCT, had no useful data, or were not the comparison of cemented and cementless fixation were excluded, 16 high-quality randomized controlled trials14–21,25–32 were included in the present meta-analysis. The investigators reached an agreement. The flowchart of the studies included is presented in Figure 1. Flow diagram of the studies included.
Characteristics of the trails
The characteristics of included studies.
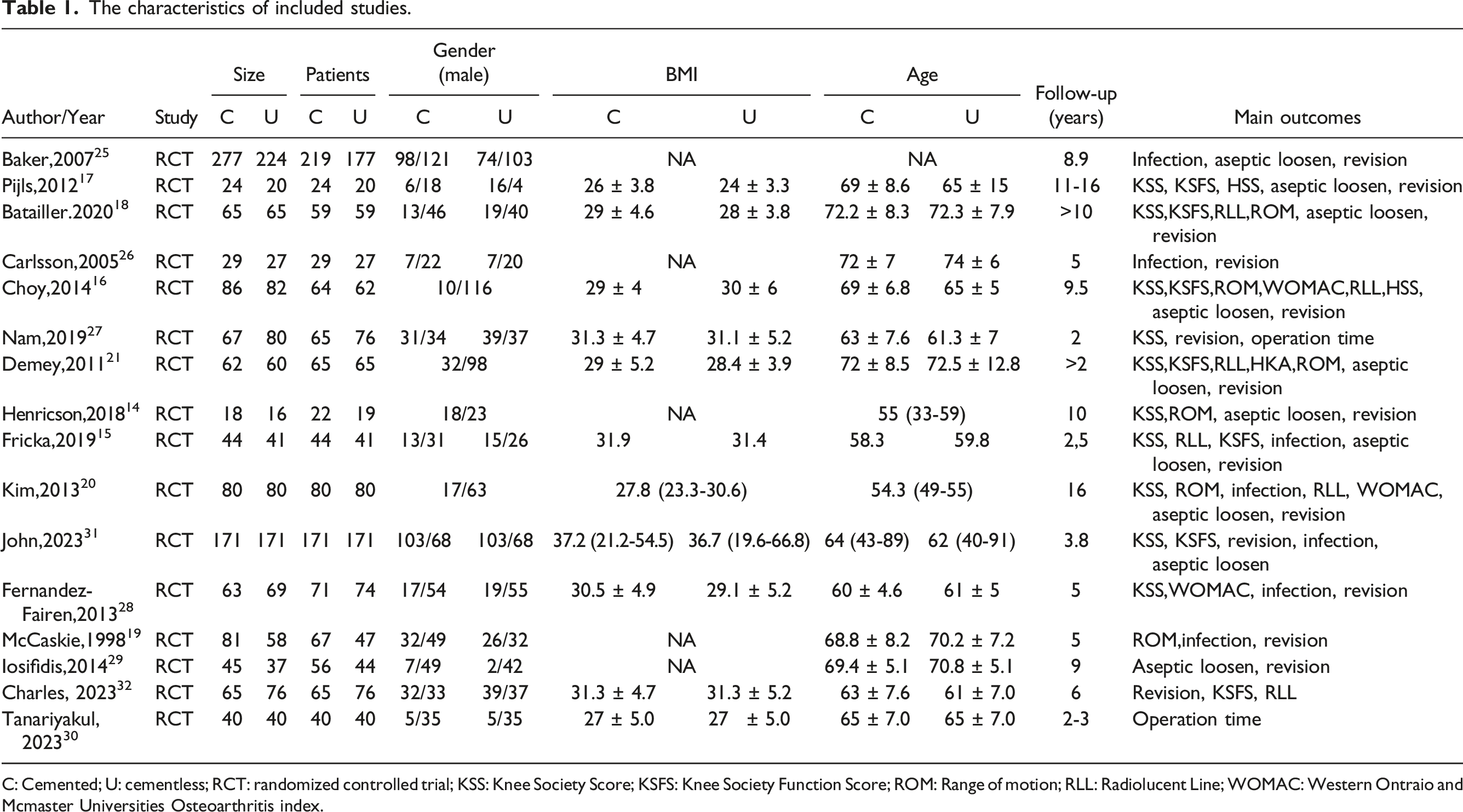
C: Cemented; U: cementless; RCT: randomized controlled trial; KSS: Knee Society Score; KSFS: Knee Society Function Score; ROM: Range of motion; RLL: Radiolucent Line; WOMAC: Western Ontraio and Mcmaster Universities Osteoarthritis index.
Revision
All included studies14–21,25–32 reported data on revision between the cemented and the cementless group. Thirty-six out of 1183 in the cemented group were revised, while 32 out of 1130 in the cementless group were revised. However, the fixed-effects meta-analysis showed that there was no significant difference in revision between the cemented group and the cementless group with no heterogeneity (OR = 1.01; 95% CI 0.63 to 1.62, p = .96; Heterogeneity: χ2 = 5.27, p = .92, I2 = 0%). The funnel plot showed no significant publication bias. The forest plot and funnel plot are illustrated in Figure 2(a) and (b). The Egger’s test showed no publication bias (intercept = −0.43, p = .51). Forest plot and funnel plot for revision, infection, and aseptic loosening after total knee arthroplasty. (a-b). Forest plot and funnel plot for revision; (c-d). Forest plot and funnel plot for infection; e-f. Forest plot and funnel plot for aseptic loosening.
Infection
Seven of the trials15,19,20,25,26,28,31 compared the infection between the cemented group and the cementless group. Twenty out of 745 patients in the cemented group and 13 out of 670 patients in the cementless group were infected. The fixed-effects meta-analysis of the 7 trials showed that there was no significant risk of infection between the two groups after total knee arthroplasty. (OR = 1.39, 95% CI 0.70 to 2.73; p = .34), and there was no heterogeneity (χ2 = 1.22, I2 = 0%, p = .98). The funnel plot showed no significant publication bias. The forest plot and funnel plot are illustrated in Figure 2(c) and (d). The Egger’s test showed no publication bias (Intercept = 0.92, p = .26).
Aseptic loosening
Ten studies14–18,20,21,25,28,31 compared the number of participants whose prosthesis got loosened after total knee arthroplasty. From a total of 1668 patients, 17 out of 872 patients in the cemented group had prosthesis loosening, while 16 out of 796 were in the cementless group. The fixed-effects meta-analysis of 10 trials revealed that the incidence of prosthesis loosening was similar between the cemented and the cementless groups (OR = 0.89, 95% CI 0.46–1.71, p = .72), with no heterogeneity (χ2 = 2.33, I2 = 0%, p = .80). The funnel plot showed no significant publication bias. The forest plot and funnel plot are illustrated in Figure 2(e) and (f). The Egger’s test showed no publication bias (Intercept = −0.31, p = .87).
Knee society score
A total of 11 trails14–18,20,21,27,28,31 involved a total of 1393 participants who compared KSS scores between the cemented group and the cementless group at different times. Due to the significant heterogeneity, subgroup analysis was carried out, dividing the included groups into two subgroups according to the follow-ups. The subgroup within 5 years was defined as a short follow-up subgroup, while the other with beyond 5 years was defined as a long follow-up subgroup. Finally, it was found that there were no significant differences in KSS between the 2 groups in short follow-up (MD = −0.95, 95%CI –4.05 to 2.16, p = .55), with certain heterogeneity (χ2 = 17.91, p = .001, I2 = 78%). Additionally, there was no significant difference between the 2 groups in at least postoperative 5 years with heterogeneity (MD = 1.76, 95%CI –0.18 to 3.70, p = .08; Heterogeneity: χ2 = 9.57, p = .09, I2 = 48%), the forest plot is illustrated in Figure 3. Sensitivity analysis was performed later, finding that after excluding one RCT15,16 in long follow-up, there was no heterogeneity (χ2 = 6.37, p = .17, I2 = 37%), and KSS in the cemented group was significantly higher than that in the cementless group (MD = 2.79, 95%CI 0.95 to 4.63, p = .003). Also, after excluding one RCT15,16 in short follow-up, there was no heterogeneity (χ2 = 1.99. p = .57; I2 = 0%), and KSS in the cemented group was significantly lower than that in the cementless group (MD = -0.18, 95%CI -1.37 to 1.01, p = .004). The funnel plot showed no publication bias. The forest plot of sensitivity analysis and funnel plot are illustrated in Figure 4(a) and (b). Egger’s test was not available here due to the 95%CI covered 0, we performed begg’s test and found there was no publication bias in both long follow-up (Spearman’s coefficient = −0.60, p = .21) and short follow-up (Spearman’s coefficient = −0.2, p = .75). Forest plot for KSS after total knee arthroplasty. Forest plot and funnel plot for KSS sensitivity analysis after total knee arthroplasty. (a) forest plot for KSS; (b) Funnel plot for KSS.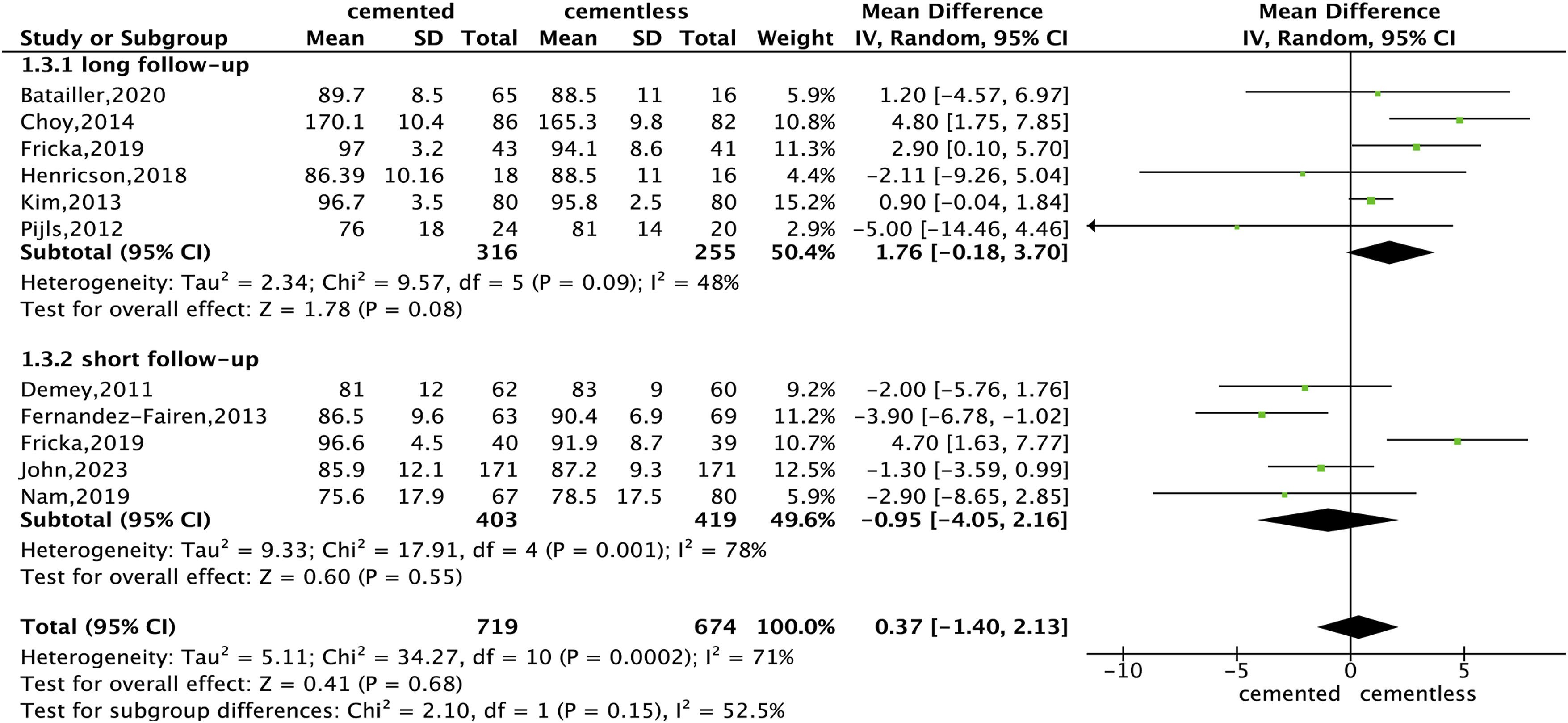

Operation time
Two studies
30
reported operation time with 221 participants. Results exhibited that operation time in the cemented group was significantly higher than in the cementeless group (MD = 12.03, 95%CI 8.30 to 15.77, p < .00001; Heterogeneity: χ2 = 0.04, p = .83, I2 = 0%). The funnel plot did not exhibit any significant publication bias. The forest plot and funnel plot are listed in Figure 5(a) and (b). Forest plot and funnel plot for Operation time, KSFS and ROM after total knee arthroplasty. (a-b). Forest plot and funnel plot for operation time; (c-d). Forest plot and funnel plot for KSFS; (e-f). Forest plot and funnel plot for ROM.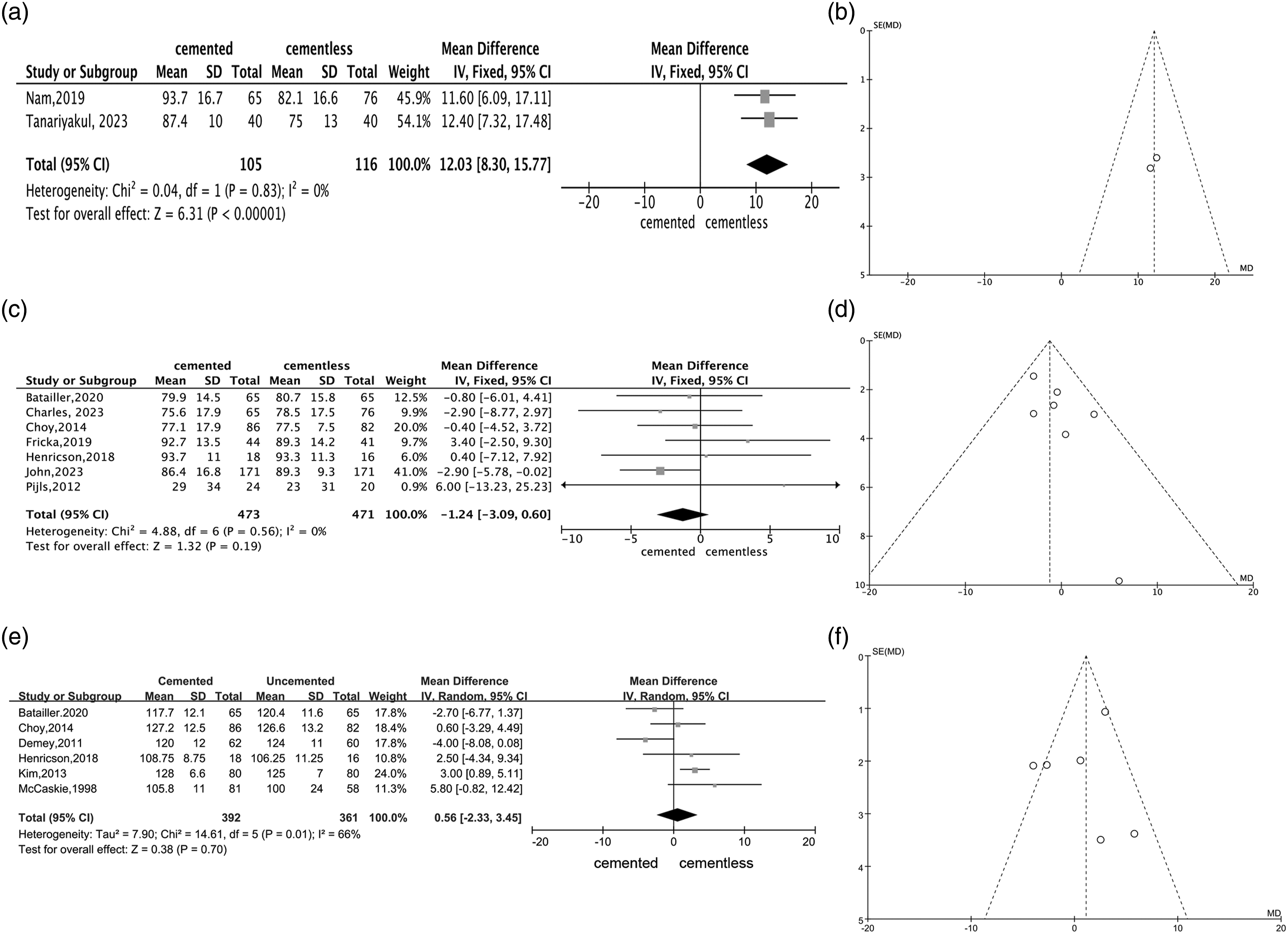
Knee Society Function Score
Overall, seven studies14–18,31,32 reported KSFS with 944 participants. It was found that there was no significant difference in KSFS between cemented groups and cementless groups after total knee arthroplasty (MD = −1.24, 95% CI -3.09 to 0.60, p = .19; Heterogeneity: χ2 = 4.88, p = .56, I2 = 0%). The funnel plot showed no significant publication bias. The forest plot and funnel plot are listed in Figure 5(c) and (d). The Egger’s test showed no publication bias (Intercept = 0.15, p = .93).
Range of motion
A total of six studies14,16,18–21 reported the ROM scores in cemented and cementless fixation for the total knee arthroplasty with a total of 753 samples, and the meta-analysis demonstrated that two groups have no significant difference (MD = 0.56, 95%CI –2.33 to 3.45, p = .70), meanwhile, it has heterogeneity (χ2 = 14.61, p = .01, I2 = 66%). Sensitivity analysis was performed and none of these trials be excluded can decrease the heterogeneity. Because of the heterogeneity, the random effect model was adopted. The funnel plot showed no significant publication bias. The forest plot and funnel plot are illustrated in Figure 5(e) and (f). The Egger’s test showed no publication bias (Intercept = 0.82, p = .51).
Radiolucent Line
Overall, 6 studies15,16,18,20,21,32 reported the Radiolucent Line with a total of 806 samples. The random-effects meta-analysis of all 6 trials revealed that there was no significant difference between cemented groups and cementless group after total knee arthroplasty (OR = 1.73, 95%CI 0.65 to 4.62, p = .27); And it has certain heterogeneity: χ2 = 23.00, I2 = 78%, p = .0003), Then sensitivity analysis was performed and found that none of these trails be excluded can decrease the heterogeneity. Because of the heterogeneity, the random effect model was finally chosen. The funnel plot showed significant publication bias. The forest plot and funnel plot are illustrated in Figure 6(a)–(b). The Egger’s test showed publication bias (Intercept = −2.23, p = .10). Forest plot and funnel plot for RLL and WOMAC after total knee arthroplasty. (a-b). Forest plot and funnel plot for RLL; (c-d). Forest plot and funnel plot for WOMAC.
Western Ontario and McMaster Universities osteoarthritis index
Three studies16,20,28 assessed the cemented and cementless fixation for the total knee arthroplasty using the WOMAC scores, a considerable statistical heterogeneity existed among the 3 studies (χ2 = 7.70, p = .02, I2 = 74%), and the random-effects model was applied for performing the data analysis, the meta-analysis of the 3 eligible trials show that there was not a statistically significant difference in the WOMAC scores (n = 460, WMD = −0.22, 95%CI –1.76 to 1.31, p = .77). Sensitivity analysis was also performed and none of these trails were excluded can decrease the heterogeneity. Due to the heterogeneity, the random effect model was finally chosen. The funnel plot showed no significant publication bias. The forest plot and funnel plot are illustrated in Figure 6(c)–(d). The Egger’s test showed no publication bias (Intercept = −0.44, p = .80).
Certainty of evidence
The GRADE results showed that the certainty of the evidence for aseptic loosening, revision, infection, KSS, and operation time was high, and the certainty of the evidence for ROM, RLL, KSFS was moderate. The main reasons for the decreased level of evidence were bias and inconsistency. The results were shown in Supplemental Table 2.
Risk of bias assessment
The quality of all included RCTs indicated a low risk of bias. All RCTs contained detailed methods of random sequence generation. Seven RCTs reported allocation concealments, and because of not declaiming the allocation concealments, the rest studies were classified into unclear risk of bias. Five RCTs was assessed as unclear risk of bias because they didn’t report the blinding of participants and surgeons And outcome assessment was blind in 12 RCTs, the rest one didn’t report the information so we assessed it as high risk. Two studies contained incomplete outcome data. We tried to contact the authors for detail data but failed. All of the studies low risk of reporting bias. Details of deviation risk are shown in Figure 7. Risk of bias summary and graph of randomized controlled trials.
Discussion
Both cement fixation and cementless fixation are commonly used fixation methods in total knee arthroplasty, with cement fixation being more commonly used. The meta-analysis contains outcomes such as KSS, KSFS, WOMAC, ROM, revision, infection, aseptic loosening, operation time, and RLL. The meta-analysis results showed that there was no significant difference in revision between cemented and cementless fixation, which was consistent with the results of the previous study. For instance, Batailler et al. 18 reported that there was no significant difference in revision rate between the cemented group and cementless group. Many studies have shown that the main causes of TKA revision are infection and aseptic loosening.33–35 However, the results showed that there is no difference between the two groups in infection and aseptic loosening. This is also clear in Baker’s study, 25 which indicated that there was no significant difference between the two fixation methods in infection and aseptic loosening. Therefore, it is suggested that surgeons can choose either of the two methods according to their surgical tendency and the needs of patients. However, some potential uncertain factors may influence the prognosis of TKA, such as surgical skills, aseptic condition, osteoporosis, etc. These factors may affect the aseptic loosening and infection then lead to revision. Meanwhile, the subgroup analysis results showed that cementless fixation showed better KSS in the first 5 years after surgery, while cemented fixation showed superior results after 5 years, which indicates that cementless fixation may be suitable for older patients while cemented fixation fits younger patients to obtain a better joint function. As previous studies reported, KSS was similar in cementless and cemented fixation.16–18 Our finding is the first time to report the different KSS at different times between cemented and cementless fixation for TKA. Notably, the cementless group requires markedly less operation time, which further strengthens the above finding that cementless fixation fits older patients for surgical safety. Nam et al. 27 reported that the average operation time of cement fixation was 93.7 ± 16.7, while that of cementless fixation group was 82.1 ± 16.6. The results showed that cementless fixation may have more advantages in the length of operation. In addition, there was no significant difference in KSFS scores between the two methods. Fricka et al. 15 reported that there was no significant difference in KSFS score between the two groups, which was consistent with the current results. In addition, ROM, WOMAC, and RLL were also compared. This analysis showed that there were no significant differences between the cemented group and the cementless group. The results are consistent with those of the previous studies. Choy et al 16 reported that there was no significant difference in ROM and WOMAC between cemented and cementless fixation.
In clinical practice, the results of this study indicate that both cemented and cementless fixation methods are feasible choices for TKA, with specific advantages depending on the duration of the prosthesis’s presence. Surgeons can choose fixation methods based on patient characteristics, surgical preferences, and specific clinical conditions. For example, cementless fixation surgery may be more suitable for elderly patients because of its shorter surgical time and better short-term functional effects, while cement fixation may be more suitable for younger patients or those who require long-term stability.
Strength
The previous meta-analyses involving cemented fixation and cementless fixation included a large number of low-quality cohort researches or few RCTs of which are repeat studies, which may cause certain bias in those meta-analyses,36,37 therefore, this study included 16 high-quality RCTs involving cemented fixation and cementless fixation in TKA, trying to provide a reference for the clinic. Compared with the previous meta-analyses, there are certain advantages to the study. First, a detailed search strategy and more strict inclusion criteria were formulated. A sum of 16 high-quality RCTs were included in this study, providing more effective evidence. Second, cohort research was excluded to make sure of the reality of the results.
Limitation
In the analysis, all the valid data were included to ensure comprehensive coverage. However, certain indicators exhibited heterogeneity, which was addressed through appropriate subgroup analyses and sensitivity analyses where necessary. Despite these efforts, this meta-analysis has inherent limitations, including the limitation of publication language, which may introduce language bias and exclude relevant studies in other languages. In addition, the surgical management plan, the kind and material of prosthesis and rehabilitation plan were not standardized across studies, potentially contributing to variability in results. Similarly, the small sizes of the included studies may affect the generalizability and robustness of the findings. Furthermore, the studies from different countries conducted introduce potential uncertainties regarding the positive evidence for TKA. The KSS score system is a synthesis, containing three parts, in which the really impacting factor is not specified. Due to certain characteristics of surgical techniques, orthopedic surgeons are unlikely to be blind, so care should be taken in interpreting the estimates of this meta-analysis. Future studies should focus on maintaining consistency in race, technique, and type of prosthesis to achieve more robust results.
Conclusion
Within a follow-up period of less than 5 years, cementless TKA had better KSS, while over 5 years, KSS was better in cemented TKA, and cementless TKA required less operation time. There is no significant difference between the two methods in terms of infection, revision, aseptic loosening, and other functional and impact scores.
Supplemental Material
Supplemental Material - Comparison of Cemented and Cementless Fixation in Total Knee Arthroplasty: A Meta-Analysis and Systematic Review of RCTs
Supplemental Material for Comparison of Cemented and Cementless Fixation in Total Knee Arthroplasty: A Meta-Analysis Systematic Review of RCTs by Zirui Liu, Lei Wen, Libo Zhou, Zhongcheng Liu, Yi Chen, Bin Geng and Yayi Xia in Journal of Orthopaedic Surgery.
Footnotes
Authors’ contribution
Study design: Yayi Xia, Zirui Liu, Data collections, Zirui Liu,Lei Wen, Libo Zhou, Zhongcheng Liu, Bin Geng, Data analysis: Zirui Liu, Lei Wen. Writing: Zirui Liu, Lei Wen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Lanzhou Science and Technology Plan Program (2021-RC-102), The National Natural Science Foundation of China (81960403, 82060405, 82360436), Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2021-MS-A07, CY2022-MS-A19), Natural Science Foundation of Gansu Province (22JR5RA943, 22JR5RA956, 23JRRA1500).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.