
Abstract
The ankle joint serves as the primary weight-bearing flexor joint in the human body. When standing, the entire body’s weight is supported by this joint, and during walking, the load on it increases to 5 times that of body weight. Ankle sprains account for approximately 20% to 30% of all sports injuries. Among these, lateral ankle ligament injuries constitute more than 85% of all ankle sprains, with around 70% of acute or occasional ankle sprains progressing into chronic lateral ankle instability (CLAI).1–3 Ankle instability can be classified into mechanical instability and functional instability. 4 Mechanical instability refers to conditions where joint range of motion exceeds normal physiological limits due to various factors. Functional instability refers to a condition where joint movement may not exceed normal physiological limits but lacks complete or partial autonomous control for various reasons. Birmingham 5 demonstrated no difference between functionally unstable ankles and normal joints. Ozeki 6 suggested that this condition arises from a deficiency or damage to mechanoreceptors present in the ankle joint capsule or ligaments. Chen 7 discovered that instability in one ankle joint may result in pain in the other.
The anterior talofibular ligament (ATFL) is the weakest component of the lateral ankle ligament complex and it is highly susceptible to injury. Failure to obtain prompt and effective treatment following an injury can often lead to synovial hyperplasia and Talar osteochondral injury. In severe cases, this condition can progress to osteoarthritis. 8 Therefore, repairing or reconstructing ATFL has become a crucial aspect in managing CLAI.
Traditional methods for treating ankle sprains and functional ankle instability encompass nonoperative treatment and surgical intervention. 9 In cases where symptoms are mild or have minimal impact on daily life or work, nonoperative treatments such as external fixation braces and orthopedic shoes can be utilized. If ankle instability persists or pain remains significant after 3 months of nonoperative treatment, surgical intervention is necessary. Surgical options for CLAI include anatomical repair, anatomical reconstruction, and non-anatomical reconstruction. Anatomical repair is the least invasive with a faster recovery time, making it the preferred choice for initial lateral malleolus ligament operations. Broström 10 initially proposed a method involving repairing and tightening the ATFL to address CLAI by directly suturing the torn ends of ATFL and/or CFL during surgery. This approach resulted in good restoration of ankle joint stability with an 85% success rate. Modified surgical techniques such as Watson-Jones, 11 Evans, 12 Chrisman-Snook 13 surgerys have also demonstrated positive outcomes in previous reports. The Gould 14 procedure has shown favorable results by reinforcing the suture of the outer portion of inferior extensor retinaculum (IER) using a fibular periosteal flap to enhance strength and stability of anterolateral soft tissues surrounding the ankle joint. Additionally, bone anchor technology has been successfully employed in recent years to repair or reinforce the ATFL. 15
The objective of this study introduces a all-inside modified “outside-in” Broström -Gould procedure as an alternative approach for addressing CLAI and establishes a correlation between these findings, subjective symptoms reported by patients, and objective results from clinical follow-up examinations.
Anatomy and biomechanics
ATFL originates approximately 1 cm above the tip of the lateral malleolus and courses in an anterior, medial, and downward direction at an angle of approximately 25° from the horizontal plane. Its primary function is to restrict forward movement and varus deviation of the talus bone. The distal portion of this ligament wraps around and terminates at the anterior external corner of the lateral articular surface of the talus. When in a neutral position, the running direction of the ATFL is nearly perpendicular to the longitudinal axis of fibula. This anatomical arrangement effectively limits anterior displacement of the talus bone. However, it should be noted that this ligament is actually inclined at an angle of about 25° relative to horizontal plane. This inclination demonstrates its important role in counteracting foot varus as well. The attachment area between this ligament and talus bone exhibits close adherence, which aids in dispersing tension within this region and reducing susceptibility to tearing or fracturing when ankle pronation occurs along with forward movement of talus bone. 16 Histological studies have also confirmed that tear injuries are more likely to occur at fibula attachment site rather than at talus attachment site for this particular ligament. 17
Materials and methods
This retrospective study included 40 consecutive CLAI patients (40 ankles) who underwent total arthroscopic treatment for CLAI with a modified “outside-in” Broström-Gould procedure from February 2020 to November 2022.
Inclusion criteria
The patients had a history of ankle sprain lasting for more than 3 months, with frequent foot slapping. They exhibited a positive unilateral heel raising test, positive ankle drawer test, and positive talar tilt test. Additionally, all patients showed an ATFL injury on magnetic resonance imaging (MRI).
Exclusion criteria: Presence of neuromuscular disorders,open injury, ankle joint fracture (excluding distal malleolus avulsion fractures), without evident talus osteochondral damage, combined medial deltoid ligament injury, soft tissue infection or intra-articular infection in the ankle joint,ankle arthritis resulting from various causes, unsuccessful previous open or arthroscopic lateral ankle ligament reconstruction, elderly patients with excessive smoking history, other systemic diseases.
All patients received nonoperative treatment for 3-6 months prior to surgery. However, there were no significant improvement in symptoms and recurrent ankle sprains were observed. Preoperative evaluation included the unilateral heel-raising test, ankle drawer test, and talar tilt test to assess structural ligament insufficiency. It should be noted that these tests may yield negative results if the ankle instability was purely functional. The unilateral heel-raising test requires precise execution as it was prone to false negatives. Additionally, the talus tilt test should be performed under X-ray guidance with proper precautions taken against radiation exposure. Homogeneous MRI was conducted before hospitalization.
Operative technique
Arthroscopic exploration and cleaning
The patient was placed in supine position with a thigh tourniquet, foot protruded from the operating table about 8-10 cm,placed a soft pad under the hip to make the affected ankle slightly pronate, routinely disinfected, and anatomical structures such as the ATFL, superficial peroneal nerve, peroneal tendon, and retinaculum were marked to determine the approach position and suture range. A standard anteromedial and anterolateral approach were performed with a 30° ankle arthroscopy. Meanwhile, ankle stability and articular cartilage injury were observed under the arthroscope. Arthroscopy revealed that the ATFL was damaged completely at the fibular attachment in all patients, 5 cases had slight injury of talus osteochondral, synovial hyperplasia was observed in 25 cases, 8 cases had osteophytic hyperplasia, 2 cases with injury of the anterior tibiofibular ligament, 1 case with avulsion fracture of fibula attachment.We thoroughly removed hyperplastic osteophytes and synovial issue, removed fibula avulsion fracture, and cleaned up damaged talar cartilage tissue.
Arthroscopic ATFL repair and IER strengthening
The surgical procedure involved creating an auxiliary incision at the surface projection of the anterior fibula, specifically targeting the ATFL. The scope was introduced through both the anterior and external central approaches, while instruments were operated through the auxiliary approaches. To expose the distal fibula’s ATFL endpoint, radiofrequency vaporization was utilized to remove soft tissue on the fibula’s surface. Additionally, a sharpening machine was used to freshen up the bone surface (Figure 1). A bone hole was drilled at the endpoint of the ATFL, followed by insertion of a 3.5 mm diameter corded anchor (Johnson & Johnson). Double strands of PDS line were threaded into the 16-gauge trocar, and the loop was threaded out at the tip of the needle. The trocar was inserted toward the lower edge of the ATFL, and then the needle was positioned close to the lateral side of the talus upward, paying attention to avoid damage to the lateral talus cartilage. The PDS line loop was pulled on the upper edge of the ligament with mosquito vascular forceps.One tail line of the anchor was taken as the main line and the other as the auxiliary line. PDS line was “loop-like” to lead to the auxiliary line, and the PDS line was completely removed. The auxiliary line loop was rotated clockwise for 180°, the main line passed through the line loop, the auxiliary line loop was rotated clockwise again for 180°, and the tail of the auxiliary line passed through the line loop. The ankle joint was fixed with a knot pusher in the dorsiflexion valgus position to complete the anatomical repair of the ligament. (Figure 2) (Figure 3) Arthroscopic vision showing the ATFL is ruptured at the insertion of the fibula. (1) Talus. (2) Fibula. (3) ATFL remnant. Arthroscopic vision showing anchor reconstruction of ATFL insertion and external knotting techniques. Schematic diagram of the anchor to reconstruct the ATFL insertion.
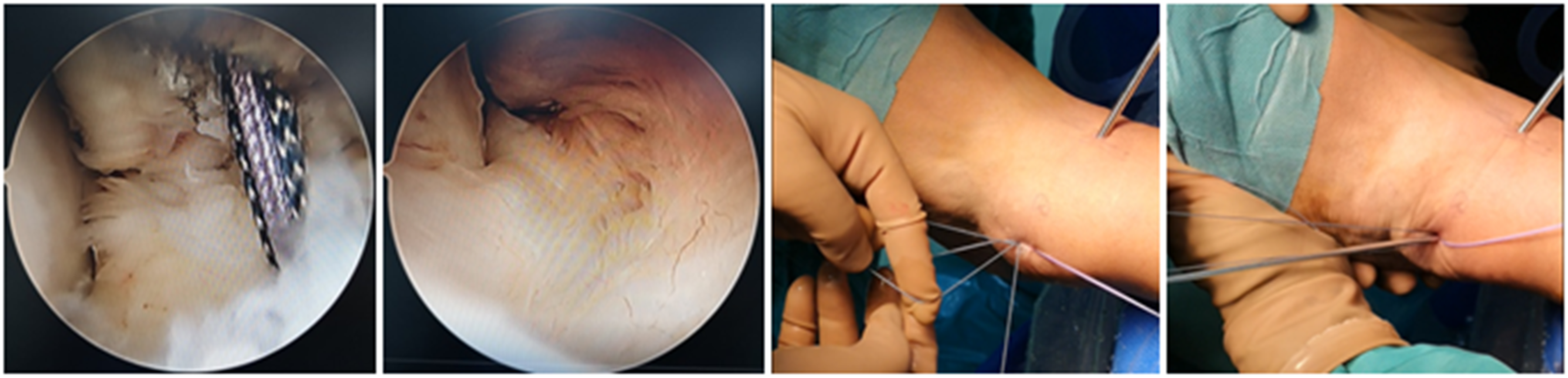

Another anchor line was threaded through the tail of the greater horn needle, perpendicular to the direction of the extensor retinaculum, and out of the deep layer of the IER. The other line was threaded in the same way, and the two lines were at an Angle of about 45°. Both of the lines were converged and knotted in the subcutaneous layer (Figure 4). The anterior drawer test and varus test of ankle joint were negative after operation (Figure 5). IER was pulled to the anterior border of the lateral malleolus. The anterior drawer test and varus test of ankle joint were negative. Schematic diagram of the IER to the anterior border of the lateral malleolus.

Postoperative management
The isometric contraction training of the lower limb muscles commenced on the second day postoperation. The brace was removed at 2 weeks postoperation, and a long-leg ankle brace was worn for passive-active dorsiflexion and plantarflexion functional exercises. At 4 weeks postoperation, half weight-bearing exercises, ankle varus and valgus functional recovery exercises (passive-active), as well as calf muscle strength training were performed with an ankle brace. At 6 weeks postoperation, the ankle brace was discontinued to enable full weight-bearing walking, along with active-passive varus and valgus functional exercises for ankle stress and lower limb balance training.
Statistical methods
The measured data were analyzed and processed using SPSS-22.0 statistical software, and the results were presented as mean ± standard deviation (
Results
Characteristics of the patients.

Comparison of VAS, AOFAS and Karlsson-Peterson scores before and after surgery in 40 patients.

Discussion
The lateral ligament complex of the ankle joint comprises the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular ligament (PTFL). Among them, the ATFL is considered as the weakest and most vulnerable part. 18 Therefore, repairing or reconstructing the ATFL has become a crucial step in treating chronic lateral ankle instability (CLAI). Currently, there exist numerous surgical approaches for the treatment of CLAI. In 1966, Broström initially proposed a technique involving repair of the compressed ATFL to address CLAI. Building upon Broström ‘s procedure, reinforcement and suturing of the lateral aspect of the subextensor retinaculum (IER) with a fibular periosteal flap were performed to further enhance the strength and stability of the anterolateral soft tissue in the ankle joint, yielding satisfactory outcomes. However, advancements in anatomical and clinical research have led several scholars in this field to report that patients within the Broström -Gould group did not achieve superior clinical efficacy.19,20
Through the examination of the IER anatomy in the ankle joint, we observed a persistent gap between the lateral bundle of the IER and the anterior edge of the fibula. Inexperienced physicians often neglect suturing the fiber bundle of this lateral component during Gould procedure, which could potentially explain its ineffectiveness. Jeong 21 conducted measurements on patients with CLAI undergoing repair surgery, revealing an average distance of approximately 9.8 mm between the lateral bundle of interest and the anterior fibula. Dalmau22,23 observed that the feasibility of the Gould procedure relied on the presence of an “X” retinaculum; however, due to the inherent weakness of this structure, ligment repair did not yield the desired stability. C Stecco ‘s immunohistochemical staining study revealed that the upper lateral oblique bundle of the “X-shaped” IER consisted solely of collagen fibers and a limited amount of elastic fibers. 24 Gao ‘s research demonstrated that Gould augmentation surgery merely served as a “temporary internal fixation for 4 weeks post-surgery,” necessitating further validation through extensive data and time.19,20 Therefore, it is reasonable to speculate that the original Gould procedure may have involved the utilization of deep fascia in the sinus tarsi region and did not involve pulling the trunk of the lateral bundle of the IER to the anterior edge of the lateral malleolus. We employed a novel “outside-in” Broström-Gould technique for treating CLAI. Initially, we anatomically repaired the injured ATFL using an anchor, the IER edge was pulled in a “fan” shape to the anterior edge of the lateral malleolus, resulting in remarkable outcomes.
The most frequent postoperative complication of the Broström-Gould procedure was injury to the superficial peroneal nerve,25–28 which may be attributed to surgeons’ inadequate understanding of the anatomy in this region. To effectively reduce the incidence of postoperative nerve damage, Acevedo 29 conducted an anatomical study of the anterolateral ankle joint and introduced the concept of a surgical “safe zone” for this area. A distance of 15 mm from the anterior edge of the fibula was recommended to ensure sufficient interosseous ligament repair without compromising on preservation of the superficial peroneal nerve. All our procedures were performed within this safe zone. In this study, 2 cases experienced postoperative skin hypoesthesia on their dorsum pedis, but they were resolved with nonoperative treatment. It was considered that there were individual differences in the course of the superficial peroneal nerve from the dorsal ankle to the dorsal foot. 30
The modified “outside-in” Broström-Gould technique incorporates the following surgical modifications compared to the previous method: (1) All procedures were performed through an anterolateral approach; (2) The lateral band of the IER was pulled in a “fan-shaped” manner towards the anterior edge of the lateral malleolus, with a suture angle ranging from 40° to 50°; (3) The Gould suture was placed within the designated “safe zone”. This modified technique effectively relocates and reinforces the lateral bundle of the IER to enhance stability at the anterolateral ankle joint. Significant improvements were observed in evaluation indices between preoperative and postoperative assessments, indicating favorable surgical outcomes.
The limitations of this study are as follows: the sample size for surgery is relatively small, and efforts should be made to increase the sample size in future studies; the follow-up duration for most cases is short, and there is a lack of Color Doppler ultrasound and MRI review after arthroscopic ligament repair, which leads to uncertainty regarding long-term efficacy. Additionally, this study does not include a comparison with the open Broström-Gould procedure, which will be addressed in future research.
Conclusion
The modified “outside-in” Broström-Gould procedure is ultimately a straightforward, efficient, and replicable technique for treating CLAI. The postoperative aesthetic outcome was exceptional, while the patients reported a positive treatment experience.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Informed consent
All study participants provided informed consent.