
Abstract
Keywords
Introduction
The shoulder joint is the most mobile joint in the human body, and it is also the joint with the most dislocations, especially the anterior dislocation of the shoulder joint. 1 In patients with recurrent anterior dislocation of the shoulder, the glenoid bone defect caused by the repeated anterior dislocation of the shoulder further aggravates the anterior instability of the shoulder. It has been reported that 90% of patients with recurrent anterior shoulder dislocation will develop glenoid bone defects. 2
Studies have shown that when the glenoid defect is greater than or equal to 25%, bony reconstructive surgery is recommended.3,4 The current main surgical methods include Bristow-Latarjet surgery and iliac crest bone graft. Although the Bristow-Latarjet procedure has achieved good results in the treatment of recurrent shoulder instability. 5 However, this operation can lead to complications such as nerve damage and early shoulder osteoarthritis, and is not suitable for patients with more than 40% of glenoid defects.3,6 Iliac crest bone graft also has risks of donor site damage, bone resorption and bone nonunion, and it is difficult to determine the reasonable bone mass that should be supplemented during surgery. 7 In addition, the concavity-compression mechanism plays a large role in maintaining the stability of the shoulder joint. 8 Concavity-compression mechanism is a mechanism of shoulder joint stability, in which the convex head of the humerus is pressed into the concave glenoid fossa. 9 This prevents the movement of the humeral head in a direction parallel to the glenoid surface. When a bone defect occurs in the glenoid, the geometry and labrum of the glenoid are damaged, and the concavity-compression mechanism is affected, resulting in a significant decrease in the stability of the shoulder joint of the affected limb. Therefore, how to accurately repair the glenoid bone defect and how to restore the glenoid width to maintain the stability of the shoulder joint requires further in-depth research.
The purpose of this study was to investigate the effect of 3D-printed technology to repair glenoid bone defect on shoulder joint stability. 3D-printed technology was used to design and fabricate a biological titanium alloy spacer to repair the glenoid bone defect. Through biomechanical tests, the width of the glenoid that should be restored after glenoid bone defect was determined, and its effect on the stability of the shoulder joint was discussed. We hypothesized that the glenoid component of the shoulder prosthesis could be fabricated using 3D-printing technology, which would enable a precise reconstruction of the shoulder glenoid articular surface geometry.
Methods
Specimen preparation
Twenty-five voluntary donated adult male cadaveric shoulder specimens with an age range of 20–40 years were used. All specimens underwent anteroposterior and lateral X-ray examinations to exclude bony lesions such as acromioclavicular joint dislocation, periarticular fracture, osteoarthritis, and evidence of soft tissue surgery such as rotator cuff. Twenty-four hours before the experiment, the specimens were thawed at room temperature. The muscles around the shoulder joint were removed, and the glenoid labrum and joint capsule structure were preserved to make shoulder bone specimens.
Model making and fixing
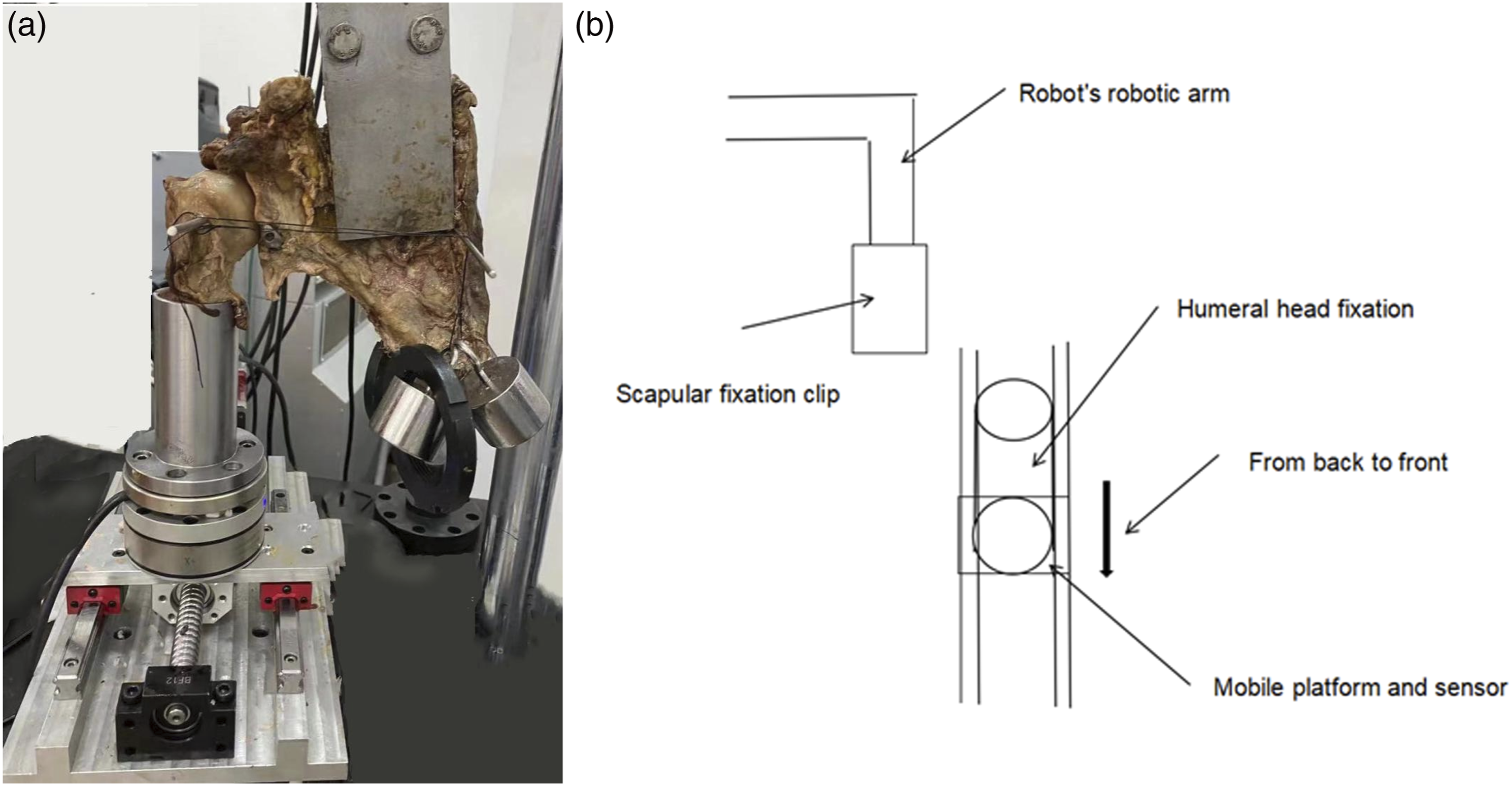
All experimental mechanical models have the same requirements for specimen preparation, fixing method, loading method, and simulated load to improve detection accuracy. The model making process includes: (1) Design and manufacture of 3D-printed glenoid pads: The CT scan data of the glenoid specimen were imported into Mimics software in DICOM format for 3D reconstruction (Figure 1). Using titanium alloy as the material, the EOS M280 printer was used to print out the experimental pads (Figure 2). (2) Installation of 3D-printed pad: After smoothing the shoulder glenoid defect, the 3D-printed guide plate was installed on the shoulder glenoid defect. A 2.0 mm Kirschner wire was inserted through the pilot hole, a 4.5 mm hollow electric drill was used to drill the bone canal from anterior to posterior, and a metal pad was placed into the bone canal. After confirming that the pad was installed flat, two bone tunnels were drilled with a 3.0 mm drill bit, and then a 3.0 mm cannulated screw was used to fix the pad. (3) Preparation and grouping of glenoid bone defect specimens: The 25 shoulder joint specimens were divided into groups A, B, C, D, and E, with 5 specimens in each group (Figure 3). Group A: no bone defect and the structure of the glenoid labrum and joint capsule was intact; Group B: Anterior inferior bone defect of the shoulder glenoid; Group C: a pad with a width of 2 mm was installed at the defect site; Group D: a pad with a width of 4 mm was installed at the defect site; Group E: a pad with a width of 6 mm was installed at the defect site. (4) Design of a fixed support and specimen installation (as shown in Figure 4): The middle and lower two-thirds of the humeral shaft will be securely enclosed within a tubular metal base using denture base resin. To maintain shoulder joint stability, the transverse and axial stresses exerted by the muscles around the shoulder joint can push the humeral head into the glenoid cavity. Therefore, starting from the neutral position of the glenohumeral joint, a 30N axial stress will be applied to the glenohumeral joint specimen to simulate the axial stress exerted by the muscles around the shoulder joint. In cases of shoulder dislocation, anterior dislocation is the most common. By applying axial stress from posterior to anterior on the lateral side of the humeral head, combined with transverse and axial stresses, the anterior dislocation of the shoulder joint can be visually simulated under the influence of force. 3D model drawing of guide plates and pads. (a) The position where the guide plate was to be placed. (b) Front view of the guide plate. (c) Side view of the guide plate. (d) The location where the pad was to be installed. (e) Front view of the pad. (f) Side view of the pad. Physical drawing of the 3D printed pads. Front (a) and side (b) view of the pad with a glenoid width of 2 mm. Front (c) and side (d) view of the pad with a glenoid width of 4 mm. Front (e) and side (f) view of the pad with a glenoid width of 6 mm. Experimental specimen of the glenoid structure. (a) Complete shoulder glenoid structure. (b) The glenoid structure with 2 mm 3D printed pad installed. (c) The glenoid structure with 4 mm 3D printed pad installed. (d) The glenoid structure with 6 mm 3D printed pad installed. (a) The images show the device settings for each test. (b) A schematic diagram of a fixed support and specimen installation.



Testing protocol
The primary outcome measures were the distance the humeral head moved forward at the time of glenohumeral dislocation and the maximum load required to dislocate the shoulder. A torque fatigue tester (TFT-J-ECO, DePuy Orthotech, Tracy, CA) and an IRB-1600 industrial robot was used in the study. The load was transferred through the load sensor and the strain was transferred through the strain cell of the machine. After the experiment, the computer automatically outputs stress, strain data and curves.
The pig shoulder joint was preloaded once before the experiment to correct the sensor and displacement values. The one-way pivot shift test was carried out under normal temperature and pressure, and the loading speed was 1 mm/s. The loading was stopped until the shoulder dislocated, and the data about the force and the displacement of the brake were recorded. Due to the new bone defect caused by shoulder dislocation in the experiment, only one biomechanical experiment was performed for each specimen.
Statistical analysis
Data were analyzed using SPSS 10.0 and origin software. Data are presented as mean ± standard deviation. ANOVA was used for comparison between groups, and a p value <.05 was considered statistically significant.
Results
Results of humerus displacement changes and axial stress loading.

*Compared with Group A, p < .05.
Similar to stability, humerus displacement was significantly lower in groups B (11.12 ± 0.01 mm) and C (11.52 ± 0.01 mm) compared with group A (18.49 ± 0.03 mm) (p < .05). When the glenoid width was restored and exceeded 2 mm (ie, with a 4 mm pad), there was no significant difference in humerus displacement between groups D and A (Figure 5). In addition, compared to group A, humerus displacement was significantly reduced in group E with a 6 mm pad (the glenoid width was restored and exceeded 4 mm), with a significant difference (p < .05). Humerus displacement changes.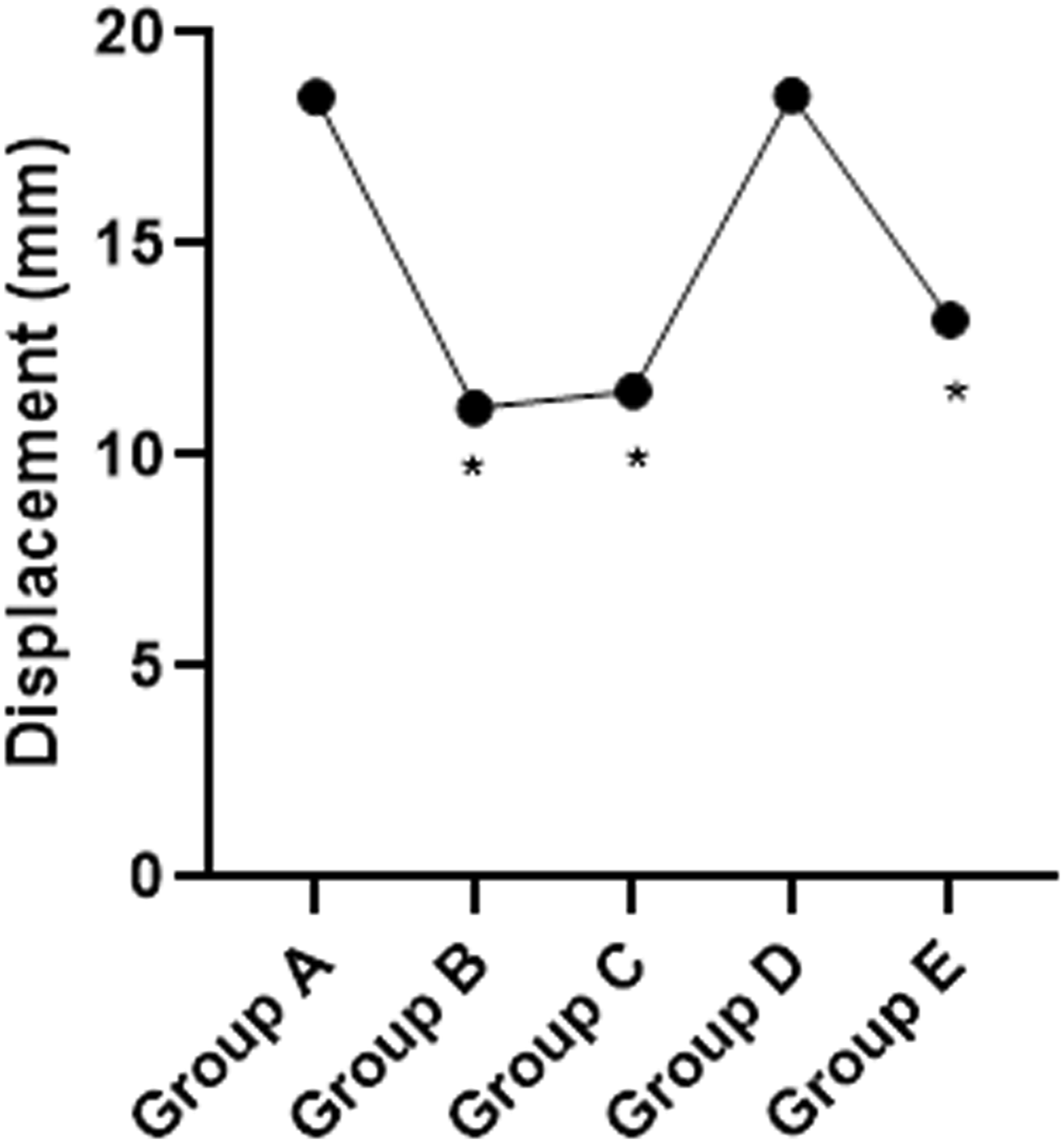
Discussion
The geometry of the glenoid and the labrum are important statically stable structures of the shoulder joint, and the integrity of the bony structure is the basis for maintaining the stability of the shoulder joint. 10 The bone defect of the shoulder joint will lead to the change in the shape of the glenoid, which will reduce the adaption of the glenohumeral joint and increase the possibility of humeral head prolapse. 11 On the other hand, the defect of the labrum leads to a decrease in the height of the glenoid rim and the depth of the glenoid, which leads to a decrease in the stability of the shoulder joint. 12 When the stability of the shoulder joint is reduced to a certain extent, the dislocation of the shoulder joint occurs under ordinary stress. 13 Studies have reported an anterior dislocation of the shoulder in 2% of the population. 14 The incidence of glenoid bone defect in patients with first-time dislocation of the shoulder joint is 22%, 15 and the incidence of glenoid bone defect in patients with recurrent dislocation is as high as 46% to 86%.16,17 When the glenoid bone defect was greater than 25%, the probability of redislocation after conventional soft tissue repair was significantly increased. 5 Therefore, it is very important to restore the geometric shape of the bony structure of the shoulder glenoid to maintain the stability of the shoulder joint. In this study, 3D-printed technology was used to design and fabricate a biological titanium alloy spacer to repair the glenoid bone defect. The main finding of this study was that the glenoid component of the shoulder prosthesis could be fabricated using 3D-printing technology, which would enable a perfect reconstruction of the glenoid articular surface geometry. Furthermore, we found that if the 3D-printed component was 2 mm larger than the normal glenoid width, it could partially compensate for the static stability of the original joint capsule and labrum complex, and restore the initial stability of the shoulder joint.
Traditional glenoid reconstruction surgery focuses on the alignment of the bone fragment with the articular surface. The grafted bone block is only an extension of the glenoid joint surface, and does not actually restore the normal geometry of the glenoid joint surface, especially the anterior-posterior curvature of the glenoid joint and the role of the labrum. The physiological curvature of the anterior glenoid edge, the depth and the inclination of the glenoid play an important role in maintaining the anterior stability of the shoulder joint. 18 In addition, in bone reconstruction surgery, the size of bone block is often affected by the anatomical factors of the donor site, and the selection of bone block size lacks corresponding biomechanical data support.
In recent years, artificial joint replacement technology has continued to develop. Bone defects around the joint are usually filled with biological titanium alloy pads, and great success has been achieved in the immediate stability and long-term efficacy of the joint. 19 Inspired by the traditional concept of artificial joint treatment, our team attempted to apply 3D-printed technology to produce bio-type titanium alloy pads, which can be used to repair severe glenoid bone defects accompanied by recurrent shoulder dislocation. The application of 3D-printed technology can perfectly restore the anatomical morphology of the glenoid surface and the depth of the glenoid, especially the physiological radian of the anterior edge of the glenoid, which theoretically avoids the shortcomings of traditional bony reconstruction techniques. However, it is unclear to what extent the glenoid width and depth of the defect should be restored to achieve adequate shoulder stability. In this study, it was found that when the bone, labrum and joint capsule of the shoulder joint were intact (group A), shoulder dislocation occurred when the load reached 44.05 ± 0.36 N. When the width of the repaired glenoid exceeded the original glenoid width by 2 mm (4 mm pad was installed, group D) and 4 mm (6 mm pad was installed, group E), the shoulder dislocation will only occur when the load reaches 51.03 ± 0.36 N and 70.61 ± 0.67 N, respectively. Compared with group A, the difference was statistically significant, indicating that the shoulder joint stability had exceeded its initial state at this time. It can be seen that an appropriate amount of bone to fill the defect can reconstruct the geometric match between the humeral head and glenoid cavity and restore the instability caused by loss of glenoid width and depth. The glenoid labrum is an important structure that maintains the stability of the shoulder joint. Studies have shown that the average physiological thickness of the glenoid labrum is about 4 mm. 20 Therefore, the installation of 4 mm and 6 mm pads not only make up for the defect of the glenoid bone, but also make up for the function of the glenoid labrum to a certain extent.
The glenoid labrum is a fibro-cartilaginous rubbery structure which encircles the glenoid cavity deepening the socket providing static stability to the glenohumeral joint. 21 The pad is a rigid material that matches the physiological curvature of the front of the shoulder joint. However, compared to Group A, increasing the thickness of the spacer (i.e., installing a 6 mm spacer, group E) can provide rigid blocking to the humeral head within a smaller range of displacement. This may be due to the fact that the 3D-printed spacer, compared to soft tissue structures like the labrum, plays a rigid blocking role in maintaining shoulder joint stability. The thicker the spacer, the greater the load borne by the humeral head and glenoid, and when the spacer thickness exceeds an additional 2 mm, the humeral head and glenoid still experience rigid blocking. Excessive load can cause fractures around the glenoid or humeral head in a shorter relative displacement, leading to shoulder joint instability. Our study showed that the installation of 4 mm pad (the width of the shoulder glenoid exceeds the original shoulder glenoid width by 2 mm) is sufficient to meet the initial stability of the shoulder joint.
The 3D-printed spacers used in this study were made of medical porous titanium alloys. Titanium and titanium alloys have good properties in terms of strength, toughness and machinability.22,23 At the site of contact with host bone, the unique porous structure and rough inner and outer surface will facilitate the adhesion, proliferation and differentiation of osteoblasts, and promote the growth of new bone tissue into pores, so as to form biological healing between implant and host bone, and finally form a stable whole. 24 This technique is expected to change the complications of donor site lesion, nerve injury, bone resorption and bone nonunion associated with the traditional glenoid bone reconstruction techniques, and also provide a new solution for the revision after the failure of traditional bony reconstruction surgery.
This study has some limitations. First, this study mainly focuses on the stability of the glenoid bone structure, but does not take into account the bone defect situation on the humeral side, which may affect the overall function of the shoulder joint. Second, this study uses cadavers for experiments, which makes it difficult to accurately assess the stability of the shoulder joint in the human body, as all the muscles around the shoulder area were removed, and the muscles also play an important role in the stability of the shoulder joint. Finally, the number of specimens in the experiment is small, which may lead to bias.
Conclusion
Patients with recurrent shoulder dislocation often have severe glenoid bone defects. The 3D-printed technology can be used to make the shoulder glenoid pad to perfectly restore the geometric shape of the shoulder glenoid articular surface. In addition, if the 3D-printed pad is larger than the normal glenoid width of 2 mm, it can replace the static stability of the original joint capsule and labrum complex for the shoulder joint to a certain extent, and restore the initial stability of the shoulder joint.
Supplemental Material
Supplemental Material - Biomechanical study of 3D-printed titanium alloy pad for repairing glenoid bone defect
Supplemental Material for Biomechanical study of 3D-printed titanium alloy pad for repairing glenoid bone defect by Danlei Huang, Jun Wang, Feixiong Chen, Haoyuan Liu and Jianming Huang in Journal of Orthopaedic Surgery.
Footnotes
Acknowledgments
Authors thank for all contributors involved in this study.
Author contributions
Jianming Huang conceived and designed the study. Zhiyang Ye and Feixiong Chen contributed to the acquisition of data and statistical analysis. Haoyuan Liu analyzed the data and wrote a draft of the manuscript. Danlei Huang and Jun Wang analyzed and interpreted the results of the experiments and revised the manuscript. All authors read and approved the fnal manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Xiamen Superior Sub-specialty construction project of Arthroscopic minimally invasive Orthopedics department (No. 2018296), Xiamen Key Specialty construction project of Traumatic Orthopedics department (No. 2015347) and Xiamen Science and Technology Plan Project (No. 3502Z20194052).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.