
Abstract
Different techniques have been described for glenoid fractures, there is still a need for safe and effective agents to promote outcomes. From January 2016 to April 2021, the clinical data of 17 patients with pulley type IA fractures treated by the V-shaped fixation technique under shoulder arthroscopy were retrospectively analyzed. Preoperative X-ray, CT, and MRI examinations were completed. The functional score of the shoulder joint, such as the visual analog scale (VAS), Constant score, and Modified Rowe score, was used to evaluate the preoperative and final follow-up clinical outcomes. The active shoulder range of motion (ROM) was also collected preoperatively and at the final postoperative follow-up. Accordingly, intraoperative and postoperative complications were also observed. The mean follow-up was 49.52 months (16-79 months). The patients’ follow-up exams showed that shoulder joint flexion, abduction, external rotation, internal rotation, and pain were not significantly different from those of the contralateral side (p > .05). The mean Constant score was 83.52 (58-98), and the average Modified Rowe score was 94.29 (70-100). X-ray and CT films of all cases showed good healing without articular depression or steps. Three patients had traumatic arthritis, with VAS <3 pain. No postoperative complications, such as infections, nerve or vessel damage, or suture anchor problems occurred during the follow-up period. Using the Double-pull, V-shaped fixation technique can stabilize the reduction of glenoid fractures while reducing the possibility of bone destruction. It is a good solution and provides an opportunity to treat rotator cuff tears associated with the procedure.
Introduction
Glenoid fractures occur when high-energy trauma to the humeral head impinges on the glenoid. Glenoid fractures are rare, and most can be treated conservatively and achieve good outcomes. The decision to use nonsurgical or surgical treatment should depend on the size and displacement of the fracture fragment, as glenoid fractures are inextricably associated with shoulder instability events.1–4
Fracture classification systems such as the Ideberg classification 5 are most commonly used in the literature based on the trauma mechanism, location, and severity of fracture patterns. The classification Type I is a glenoid rim fracture further subdivided into type IA (anterior rim fracture) and type IB (posterior rim fracture). Type IA is the most common glenoid fracture and is usually caused by dislocation of the shoulder.6–8 Many authors agree that an intra-articular step off greater than 4 mm or a glenoid rim fracture involving more than 5% to 10% of the glenoid surface are indications for surgical fixation.1,9–11 Different techniques, such as all-arthroscopic repair, arthroscopic-assisted fixation, open reduction, and internal fixation, have been described with promising results. Research in recent years has shown that arthroscopic-assisted screw fixation has good to excellent outcomes with low recurrence rates.12–15
The purpose of this retrospective study was to describe the Double-pull V-shaped fixation technique under arthroscopy in the treatment of Ideberg Type IA glenoid fracture.
Methods
Study design
From January 2016 to April 2021, 17 patients with glenoid Ideberg Type IA fractures were treated with the Double-pull V-shaped fixation technique under arthroscopy. In this study, all 17 patients met the inclusion criteria and were retrospectively analyzed.
The inclusion criteria were as follows: (1) Patient age at time of injury >18 years; (2) diagnosis of Ideberg Type IA scapular glenoid anterior fracture, bone defect >20%, displacement >1 cm; (3) injured shoulder with no previous surgery; and (4) arthroscopic glenoid Ideberg Type IA fracture repair surgery using the Double-pulley V-shaped internal fixation technique.
The exclusion criteria were as follows: (1) pathological fractures; (2) previous shoulder fracture or surgery; (3) shoulder osteoarthritis; and (4) vascular or nerve lesions in the injured shoulder.
Seventeen patients were included in the study: male/female: 6/11, average age: 50.82 years (28-71 years), and the dominant side injury accounted for 65% of those studied. X-ray, CT, and MRI examinations were completed before the operation, and the average fracture area was 28.06% (21%–37%) as measured by preoperative three-dimensional CT and intraoperative probing. Causes of injury: Twelve cases (70.59%) suffered a direct impact on the posterolateral shoulder joint, and five cases (29.41%) suffered an indirect injury. Nine cases were from electric vehicle traffic accidents (52.94%).
Patient positioning and establishing portals
In the healthy lateral decubitus position, the posterior, anterior and anterolateral approaches of shoulder arthroscopy were established as described in the literature.
16
The anterolateral approach allows a better view of the fracture site and the capsule ligament complex (Figure 1). Glenoid fracture site and the capsule ligament complex were observed arthroscopically.
Surgical technique
The four key steps of the operation were first-pull, second-lift, third-hold and fourth-close (Figure 2). First-pull (Figure 3): After fracture clearance under arthroscopy, the bone fragments and the joint capsule ligament complex were fully released with a bone pry. One needle of PDS thread was perforated at the superior margin of the glenoid fracture block of the superior glenoid labrum capsule complex. Using PDS-2 thread, indirect ligament traction reduction of fracture fragments was used to pull up the glenoid limb-labrum ligament thus reducing bone fragments. Second-lift (Figure 4): A 3.5 mm double-line anchor was implanted at the edge of the scapular neck fracture. The lasso band PDS-2 line was placed in the 5:30 and 4:30 directions to suture the fracture of the glenoid margin. The 3.5 mm anchor bolt was drawn out with the same color tail line for backup, and the sunken scapula glenoid fracture block was lifted on the tail line. Third-hold (Figure 5): implant a 2.8 mm anchor at five and 3:30 in the direction of scapular glenoid cartilage. According to the different colors of the tail line and the reserved 3.5 mm anchor tail line, the fracture block was fixed with the Double-pulley dual-row technique. Fourth-close (Figure 6): Finally, a 2.8 mm anchor was implanted at 2 o’clock to complete the lifting and sealing of the antero-superior space of the shoulder joint. There were 13 cases (76.47%) with rotator cuff tears and/or SLAP injuries. Arthroscopic treatment of the rotator cuff and SLAP injury were performed to restore the centralization of the humeral head in the glenoid fossa. The rotator sleeve tear was repaired with the Surture-Bridge technique. Sketch description of Double-Pulley, V-Shaped Fixation Technique. The first key step of the operation. The second key step of the operation. The third key step of the operation. The fourth key step of the operation.




Postoperative treatment
After surgery, the patients were fitted with a neutral abductor pillow to suspend the shoulder for 6-8 weeks. Coaxial training, table climbing, and extension exercise and internal rotation and back extension exercise were feasible within 2 weeks. After 3-4 weeks of passive exercise to flexion 100 and abduction 90 but avoiding external rotation, resistance exercise were performed for 3 months, active exercises, including flexion and abduction, scapular stabilization training and careful external rotation, were assisted after 6 weeks, and dumbbell exercises began at 6-8 weeks. Patients were allowed to resume noncontact sports after 3 months and contact sports after 6 months.
Outpatient follow-up and imaging review were performed 1, 2, 3, 6, and 12 months after the operation, and a telephone follow-up visit was performed 1 year later. The follow-up evaluation includes VAS score, Constant score, Modified Rowe score, shoulder joint test fear test, and reset test, measuring shoulder joint flexion, abduction, neutral external rotation and internal pronation, and extension angles, and comparing them with the healthy side.
Statistical analysis
In the case of a normal distribution, the sample t test was used for data analysis. When the distribution was nonparametric, STATA was used to perform the Mann–Whitney rank sum test on independent samples.
Results
Comparison of range of motion between operative side and the contralateral upper limb.

Postoperative follow-up of patients.

There was no significant difference in motor recovery, VAS, constant and Modified Rowe scores: between age >60 and <60 (p > .05); Simple glenoid scapular fracture group and glenoid fracture with rotator cuff tear group (p > .05); Glenoid fracture <25% group and glenoid fractures >25% (p > .05).
Discussion
The identification and treatment of Ideberg Type IA fractures is difficult due to occluded humeral head images and the lack of a good understanding of the injury. Glenoid fractures are usually acute injuries caused by the direct impact of the humeral head against the glenoid rim after high-energy impact injury. This is significantly different from the injury mechanism of bony bankart lesions. Ideberg Type IA glenoid fractures are frequently associated with acute rotator cuff tears, while older patients have chronic rotator cuff tears.17,18 These conditions require anatomical reduction and stable fixation to avoid future development of osteoarthritis and chronic pain.
Ideberg Type IA fracture is a split fracture with dislocation and is relatively rare. In young patients with high-energy trauma, or elderly patients with low-energy fall injury, the humeral head directly impinges on the labrum edge of the shoulder joint, and bone defects often involve >1/3 of the articular surface.
5
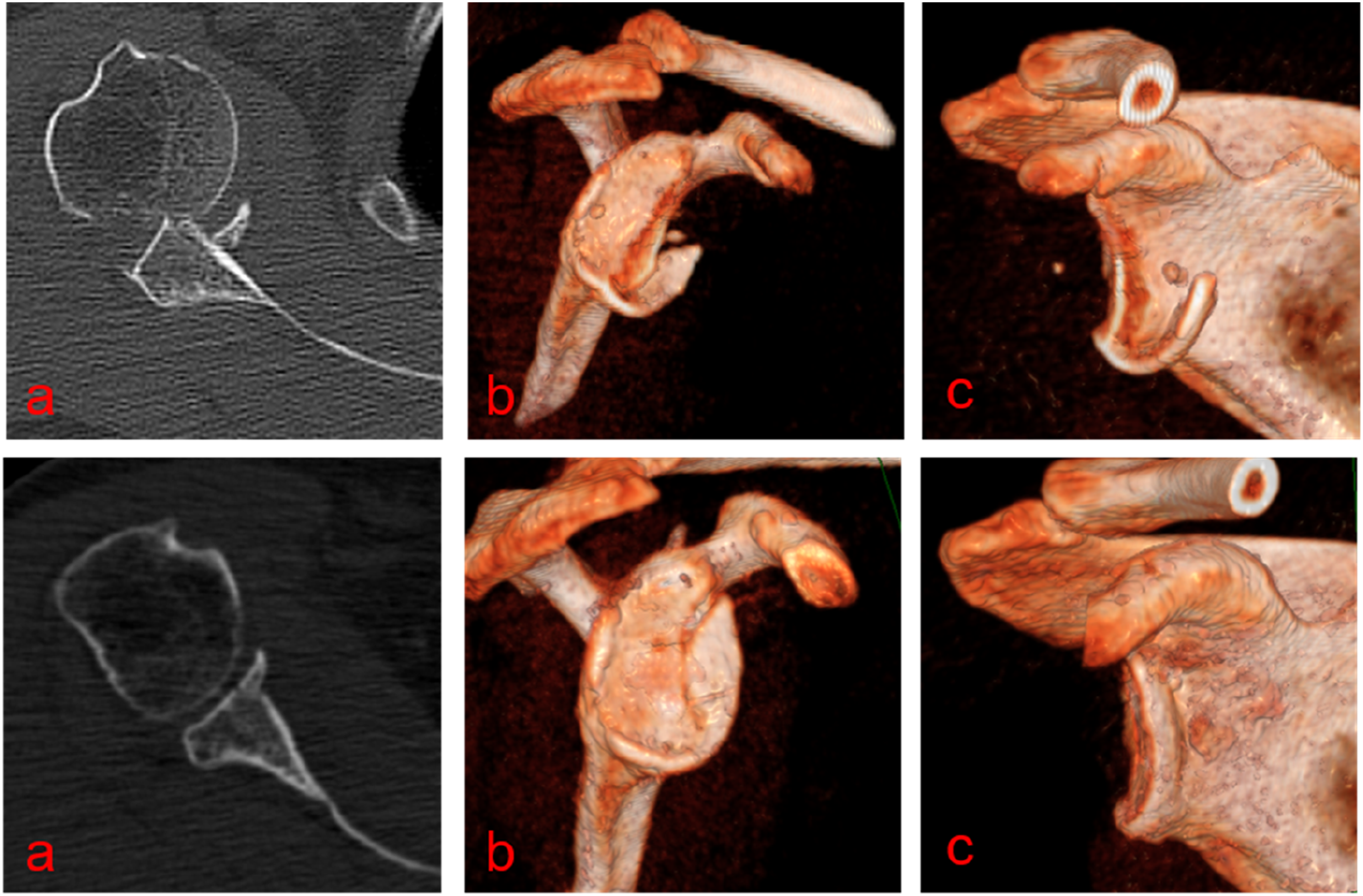
The degree of instability and subluxation of the shoulder joint will be increased in patients with scapular edge fracture combined with subluxation or rotator cuff injury (Figure 7,8)
19
and surgical treatment should be considered to achieve anatomical reduction of the glenoid edge fracture and contraction of the joint capsule (Figure 9,10). When the intra-articular step-off is greater than 4 mm or a glenoid rim fracture involves more than 5% to 10% of the glenoid surface, it is generally accepted as an indication for surgical fixation.1,9,20 X - ray shows a scapular edge fracture combined with subluxation. MR shows a scapular edge fracture combined with rotator cuff injury. CT 3D reconstruction shows the size and extent of the glenoid fracture. X-rays showed that the anchors were in good position postoperatively.


The curative effect of glenoid margin fracture depends on the fracture type (comminution degree, displacement), whether there are other fractures, and the basic function of the shoulder joint before injury. The time between injury and operation is also a key factor. According to our study, satisfactory results can be obtained provided the surgical method and timing are appropriate. A strict grasp of surgical indications is needed to avoid some patients only requiring conservative treatment to undergo unnecessary surgery. Different surgical techniques, such as total arthroscopic repair, arthroscopically assisted internal fixation, open reduction, and internal fixation, have achieved good clinical results.1,21–23 Surgical complications after fixation of glenoid fractures usually include infection, stiffness, heterotopic ossification, nerve damage, postoperative muscle weakness, and bone loss. 24 In recent years, shoulder arthroscopic technology has developed rapidly and made breakthroughs when compared with traditional open technology. Shoulder arthroscopy, as a minimally invasive surgical technique, has the advantages of reducing scar tissue, rapid healing, and early rehabilitation. 13 Its application in the treatment of different types of glenoid fractures has been widely reported in the literature.
In recent years, arthroscopic surgery has been more widely applicable to Ideberg Type IA or IB fractures (IA, IB comminuted fractures, VI fractures), acute anterior and inferior glenoid fractures involving articular surface fractures <30% or multiple bone fragments.17,25,26 Bauer, 27 2006, reported the arthroscopic treatment of 5 cases of Ideberg Type IA glenoid fracture. During the operation, the bone fragment was first reduced and maintained with a suture, which was passed through the glenoid to the infraspinatus fossa and then bound and fixed on the fascia of the infraspinatus muscle. Kim 28 reported that six Bony Bankart patients were treated arthroscopically by three-point fixation and conferred effective and had firm fixation of the bony Bankart lesion with a mean postoperative Rowe score of 94.29, but they did not give precise criteria for bony lesion sizes used in their study. There is also no standardized summary of the reset and fixation process. In their study, push-locks were used to immobilize the fracture, but it could lead the bony fragment to crack if too much tension was applied. In 2018, A. Corradini 17 reported the treatment of 11 patients with Ideberg Type IA scapular glenoid margin fracture by indirect ligament traction technique and single-band wire anchor internal fixation and achieved satisfactory results. Preoperative planning is essential to achieve satisfactory clinical results and reduce bone destruction while firmly fixing the fracture.
Studies have shown that the number, type and size of the suture anchors and the linear arrangement of multiple anchors have important effects on postoperative glenoid fracture and recurrent shoulder instability.29–31 For larger glenoid fractures, it has been reported that the use of at least three during arthroscopic surgery is recommended to reduce the incidence of postoperative unstable recurrence.31–33 In 2010, Zhang 34 suggested a new ‘Double-pulley’ dual-row technique for arthroscopic fixation of bulky Bankart lesions. In their study, two 3.5-mm double-loaded metal suture anchors were inserted as the medial row, and three 2.8-mm single-loaded metal suture anchors were placed at the edge of the glenoid as the lateral row. This technique creates two-line sutures that compress the fragment against its bone bed and restores better bony anatomy of the anterior glenoid rim. In our view, this technique may increase structural damage to the glenoid cavity despite providing strong fixation. The excessive use of anchors may also lead to larger bone defects in patients with secondary injuries. According to our study, V-shaped rim fixation (using a 3.5 mm double-line anchor implanted in the fracture margin of the scapular neck and two 2.8 mm anchors placed at five o’clock and 3: 30 o’clock on the glenoid edge) combined with a 2.8 mm anchor implanted at the 2 o’clock sealing technique can stabilize the fracture mass in the completion of larger labial fractures while reducing structural damage to the glenoid cavity. Our operation time is short and relatively simple. For a broad basal mass of the glenoid margin of the scapula, it is difficult to provide the maximum contact area between the fracture block and the glenoid bone bed and to put pressure on the broken end of the fracture, which may cause the fracture to tilt or rotate. The V-shaped fixation technique can obtain a larger contact area, pull-out force, rotation force, and anatomic reduction of the anterior glenoid margin.
In subluxation patients with poor bone quality and suspected rotator cuff tears, arthroscopy may also be used to treat rotator cuff or other joint injuries simultaneously. In this study, there were seven patients with scapular glenoid margin defects >30%, and the largest defect reached 37%, all of whom were able to achieve good reduction under arthroscopy and achieved good efficacy. There were no significant differences in ROM angle, VAS, Constant, and Modified Rowe score between the injured side and the healthy side. The technique described in this article is an alternative for reduction with stable fixation of large glenoid fractures.
Conclusion
The Double-pulley V-shaped fixation technique was useful and effective in the reduction and fixation of fractures for arthroscopic repair of larger Ideberg Type IA glenoid fractures. It provides a new option for arthroscopic treatment of scapula glenoid fracture. There are several limitations in this retrospective study. First, glenoid fractures are rare, so the sample size was small, and the follow-up time was minimal. Further studies should be performed to make comprehensive comparisons between this technique and other suture methods, such as the Double-pulley dual-row technique, in biomechanical and clinical outcomes.
Supplemental Material
Supplemental Material - Double-pulley, V-shaped fixation technique for arthroscopic repair of ideberg type IA glenoid fracture
Supplemental Material for Double-pulley, V-shaped fixation technique for arthroscopic repair of ideberg type IA glenoid fracture by Baichuan Li, Ke Rong, Haiquan Deng, Zhongfei Tang, Jian Tang and Jianchao Sun in Journal of Orthopaedic Surgery
Footnotes
Author contributions
BL and JS designed the research study. JT and KR performed the research. HD and ZT analyzed the data. JS wrote the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Natural Science Foundation of Guangxi Province (2023GXNSFBA026133).
Ethical Statement
Author’s note
Baichuan Li and Jianchao Sun wrote the main manuscript text and Ke Rong, Zhongfei Tang, Jian Tang, Haiquan Deng prepared figures and Tables. All authors reviewed the manuscript.
Data Availability Statement
The data that support the findings of this study are available from Guangxi Zhuang Autonomous Region People’s Hospital but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Guangxi Zhuang Autonomous Region People’s Hospital.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.