
Abstract
Introduction
Os acromiale (OA) is an uncommon pathology, with a variable prevalence rate among different populations. OA was first described by Cruveilhier in 1849, as a “clear line of bone discontinuity exactly where the acromial epiphysis fuses generally with the scapular spine”, 1 this description has evolved and has been modified by several authors to encompass all aspects of this condition, defined as unfused epiphysis of the acromion and failure of one ossification center resulting in a separate epiphyseal fragment. 2 There are three ossification centers in the acromion; all typically appear by 18 years of age and fuse by 24 years, pre-acromio, meso-acromion and meta-acromion, and the type of OA is determined accordingly. 2
The prevalence of OA varies between populations, ranging from 1%–30%,3,4 this point is addressed in the genetic theory, 2 as a potential explanation for this variation. The pooled rate prevalence of OA among people of black ancestry from five studies, 2 is estimated to be 14.75%, on the other hand, a pooled rate prevalence of people from white ancestry, native Americans and middle easterners, is estimated to range between 4.06 and 5.78%, 2 displaying a clear difference between the prevalence of OA in black ancestry and other ancestries. 2 However, we have to clarify that middle easterners in the previously mentioned pooled rate are represented by Israeli samples, which cannot represent the prevalence in other populations in the middle east, due to a difference in the background ancestries.
Patients with OA are generally asymptomatic, and often discovered incidentally.5,6 However, some patients may present with shoulder pain especially during abduction, with decrease in active range of motion, weakness and clicking of the shoulder, and some might manifest with point tenderness located at the site of non-union. 7 This presentation is similar to that of patients with subacromial impingement, 8 making both the process of diagnosis and management more challenging.
OA is best viewed on an axillary view X-ray of the shoulder in adult patients. Nevertheless, adolescent patients may need further investigations such as MRI or SPECT-CT. 9 A negative x-ray does not necessarily exclude OA and further investigations are needed.2,10
In this study we calculate the incidents of OA in the Saudi population, by reporting the frequency of OA utilizing shoulder MRI of patients with shoulder pathology in our institute, as a result, weighing the burden of OA and the possibility of interfering with other shoulder pathologies. In addition, to the best of our knowledge, there have been no publications reporting the prevalence of OA in patients with shoulder pain in our population.
Methods
We utilized a retrospective chart review to conduct our research. After obtaining our IRB approval we gathered all shoulder and upper arm MRIs from the radiology department and available in PACS (picture archiving and communication system) at a tertiary center between June 2015 until February of 2021, that amounted to 2779 shoulder MRI images. An exclusion criterion was applied to the sample which included: patients younger than 24 (as acromion of patients younger than 24 years is physiologically unfused), non-Saudis, repeated examination of the same shoulder and if the examination showed inadequate imaging. After applying the criteria, we excluded 356 images, and we performed systematic random sampling to reach our target sample size of 751 shoulder MRI studies.
All MRI studies were inspected and evaluated by musculoskeletal radiologists, holding a professor degree. We looked for OA and categorized it according to the side (right, left), the type (pre-acromion, meso-acromion and meta-acromion) and the size (length, width, and thickness). Patients with OA were further evaluated for the status of the rotator cuff and the type of pathology (Tendinopathic changes, partial tear, full-thickness tear).
In the included sample, patients were scanned in supine position. The scanning protocol included axial, sagittal and coronal imaging. All patients were scanned on Magnetom Skyra fit 3T (Siemens Healthineers, Erlangen, Germany) with axial Proton Density (PD) weighted fat-saturated imaging. At 3T, images were obtained with the following technical parameters: fast spin echo, repetition time (TR) of 1800 to 2200 milliseconds, echo time (TE) of 34 milliseconds, fat saturation, 3.5 mm thickness, approximately 2-min scan time, 0.7-mm skip between slices, the field of view (FOV) of 160 mm, 384 × 256 matrix, number of excitations (NEX) of 2, and echo train length (ETL) of 18 to 21.
Data collection was performed through SyngoVia reading software (Siemens Healthineers, Erlangen, Germany). Patient age, gender, underlying diagnosis, and pertinent previous surgical treatments were all recorded separately from the measurements.
For analysis, patients were categorized according to age into four quartiles; (25–44; 45–56; 57–67; 68–81). Chi-square test was conducted to test for significant differences between male and female, left and right and the difference between age groups in regard to the presence of OA. Analysis was completed using the Statistical Package for Social Science (IBM Corp. Released 2015. IBM SPSS Statistics for Mac, Version 23.0. Armonk, NY: IBM Corp).
Results
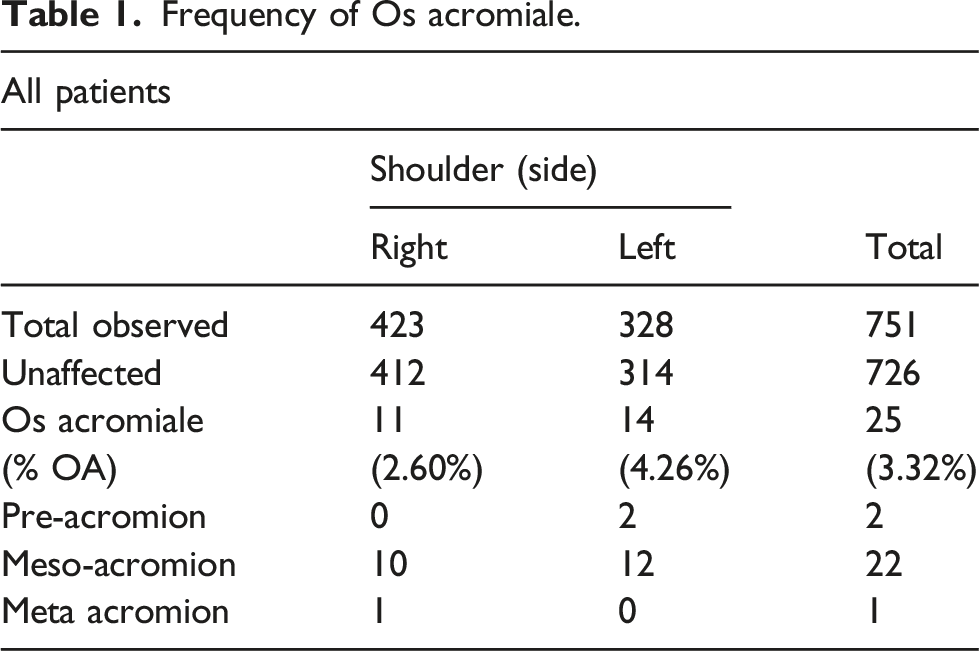
Frequency of Os acromiale.
Mean size of the Os acromiale fragments.

Frequency of Os acromiale in males.

Frequency of Os acromiale in females.


Axial T2 star images for 3 different patients with different types os acromiale. Notice the articulation between the secondary ossification center and the acromion, proximal in Meta-acromion type (a), middle in Meso-acromion type (b) and distal in pre-acrominon type (c).
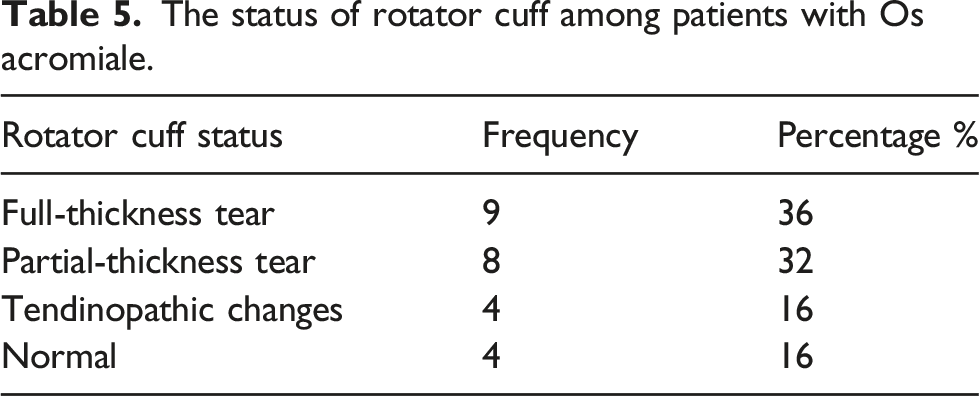
The status of rotator cuff among patients with Os acromiale.
Incidence calculation.

Discussion
Most patients who have OA are asymptomatic. Symptoms can be present due to impingement or due to associated pathology. 11 The reported prevalence of OA worldwide varies from 1.1%–20% with deferent sampling methods among deferent populations. 2 Overall prevalence of OA among Saudis visiting the Orthopaedic clinic with shoulder pain is 3.32%, which is considered relatively low compared to other populations in the literature. 2 Bilateral involvement is reported to be rare in the literature (0.7%–16%). 2 In our study there were only two cases with bilateral involvement among the 23 patients (8.7%).
It is reported in most of the literature that the prevalence of OA was found to be higher among males, but the results of significant association are conflicting. 2 In our study females have a higher prevalence of OA (72%) compared to males without a significant correlation between gender and OA. This could be attributed to the dominance of female gender among the study population. The pooled prevalence among multiple studies reported right side dominance in OA involvement. 2 The average age of the affected patients was 50.87 years old, which represents the average age for degenerative shoulder pain. 12 In Our study, left side involvement was predominant in (17/25) shoulders. The most common reported type of OA is meso-acromion. 13 Our results are consistent with the literature, and it was found in 88% of involved shoulders.
It is reported frequently that patients with OA are at risk of having rotator cuff tears. 14 The described association varies from 6.2%–9.8%. 2 . Rotator cuff tears were found in 68% of our patients with OA (Table 5). Subacromial impingement and tendinopathic changes were found in 16% of affected patients and 16% showed no rotator cuff pathology. The high percentage can be related to multiple factors: the age of the patients and presentation to the clinic with shoulder pain.
There were several limitations in this study. Firstly, the retrospective nature of the study, which might subject the data to data bias, however the cases was elected through simple random sampling. Another limitation is data was obtained from a single center, which could have hindered the capability of generalizing the study result over the entire population. Nevertheless, the data was obtained from a tertiary center that receives referrals from several regions in the country.
Conclusion
The rate of OA in patients presenting with shoulder pain is 3.32% in Saudi Arabia, which correlates with what has been previously reported in the literature. This study also corroborates the fact that the most common type of OA is meso-acromion accounting for 88% of cases. Further studies are needed to investigate the frequency of OA with or without the presence of degenerative changes and the painful presentation in shoulder clinics.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The data that support the findings of this study are available from concerned hospital but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission from IRB committee.