
Abstract
Introduction
The foot is a complex structure composed of several tissues, each of which can be the origin of the proliferation and development of the tumour. Most lesions about the foot are reactive or inflammatory, but some are true neoplasms.
Method
This is a retrospective analysis of 4997 patient records treated in the Orthopaedic Oncology Unit of University Malaya Medical Centre, Malaysia, between 1 January 2010 to 31 December 2020. Demographic data of 195 patients with foot tumours were analysed out of 4997 neoplasm patients.
Results
There were 195 cases of foot tumours: 148 were benign, and 47 were malignant. 47 were bone tumours, 4 were metastases, and 144 were soft tissue tumours. Six patients succumbed to the disease, two cases of giant cell tumour (GCT) and one patient with synovial sarcoma had a recurrence. Treatment of foot tumours was wide resection in general. However, in metastasis cases, amputation was done. The majority of tumours were in the toes and dorsum of the foot. Soft tissue tumours of the foot occur in the elderly population in contrast to bone tumours, mainly in the second decade of life. The gender distribution was almost equal for foot tumours. Ganglion and Giant Cell Tumour of the bone are the commonest benign soft tissue and bone tumours. The most common malignant soft tissue and bone tumours are malignant melanoma and chondrosarcoma. The amputation rate is 5.64% the recurrence rate is 1.54%. Mortality rate is 3.08%. The MSTS score is 79%, and the TESS score is 76.23%.
Conclusion
Foot tumours are relatively rare, mostly originating from soft tissue and exhibiting a benign nature. Nonetheless, a noteworthy proportion—approximately a quarter of these tumours—demonstrate malignancy. The surgical interventions undertaken in managing these tumours and associated functional outcomes generally yield acceptable results.
Introduction
The foot, characterized by its intricate structure, encompasses diverse tissues including skin, adipose tissue, muscle, nerve, bone, and cartilage, each capable of being the origin for the proliferation and development of tumours. While a significant number of lesions around the foot are reactive or inflammatory, a subset constitutes actual neoplasms.1–4 Notably, the majority of foot tumours, totalling approximately 80%, are typically benign in pathology.5,6 Understanding the varied tissue components and the prevalence of benign lesions underscores the importance of precise diagnostic evaluation and management strategies for individuals presenting with foot tumours.
A majority of patients, exceeding 90%, typically manifest with local swelling, and approximately half experience pain. 7 However, specific symptoms such as size, pain, or a history of trauma may be vague and lack specificity for a tumour diagnosis. Notably, the potential for malignancy in foot tumours is often underestimated, as benign tumours can present with intense pain, while certain malignant tumours, such as synovial sarcoma, may be entirely painless with a gradual onset over several years.8,9 The absence of pain, fractures, or other distinctive symptoms, coupled with the relatively low prevalence of certain tumours in the foot and ankle, frequently leads to delayed diagnosis.1,10–13 Early recognition of these subtleties is crucial for timely intervention and optimal outcomes in foot tumour management.
Superficial tumours, in contrast, are often detectable through palpation or may exhibit symptoms in the early stages of the disease.14–17 The occurrence of benign musculoskeletal tumours is approximately 200 times more frequent than malignant counterparts. Specifically, tumours affecting the feet contribute to around 3% of all musculoskeletal tumour cases. Within the realm of soft tissue tumours, approximately 8% of benign, and 5% of malignant tumors are located in the foot.1,2,18–21 Despite advancements in medical knowledge, the aetiology of these tumours remains ambiguous. The interplay of various factors contributing to the development of foot tumours underscores the complexity of their origin and necessitates further research to elucidate their underlying causes.
Morphological characteristics of foot tumours, both benign and malignant, can exhibit overlapping features. The differentiation between the two often relies on a combination of factors including age, location, and clinical examinations such as consistency, presence of skin changes, attachment of the lump to the overlying skin or underlying structures, the presence of transillumination, and imaging findings. Despite these considerations, distinguishing between benign and malignant lesions can be challenging in many instances.
Basic diagnostics typically involve plain radiographs taken in at least two planes of the foot and ankle. These radiographs are instrumental in detecting bony lesions, calcified matrix changes, fractures, radiological aggressiveness, and periosteal reactions. 22 The integration of these diagnostic modalities is essential for a comprehensive assessment, aiding in the accurate diagnosis and subsequent management of foot tumours.
Ultrasound examination plays a role in determining whether a lesion is intraosseous or extraosseous and in differentiating solid from cystic tumours. However, it’s crucial to note that the effectiveness of ultrasound is highly dependent on the operator’s expertise. As such, for imaging malignant tumours, MRI stands out as the gold standard investigation. 22 MRI provides invaluable insights for the detailed assessment of soft tissue tumours, offering information on their composition, relationship to neurovascular structures, and origin. This imaging modality assists in differentiating benign lesions from aggressive or malignant ones, with aggressive tumours often exhibiting features such as infiltration of normal fat marrow, concomitant oedema, and contrast enhancement.6,23
To achieve a definitive diagnosis of specific malignant lesions, the incorporation of immunohistochemical and genetic or molecular adjuncts is essential.16,24 These supplementary diagnostic tools play a pivotal role in refining the diagnostic process, contributing to a more precise and targeted approach. They enhance our understanding of the tumor’s nature, enabling a comprehensive characterization that goes beyond morphological features. This, in turn, facilitates the development of an appropriate and tailored treatment plan, emphasizing the importance of a multidisciplinary approach in the management of malignant lesions.
Tumours affecting the foot can be broadly categorized into two main groups: benign and malignant. Malignant tumours further subdivide into soft tissue tumours, primary bone tumours, and metastatic lesions. The definitive treatment for benign lesions typically involves an excision biopsy for symptomatic tumours. However, in cases where tumours exceed 2 cm in size, preoperative biopsies are recommended, as malignancy becomes a possibility.4,18,25 The ramifications of misdiagnosing or delaying the diagnosis of malignant foot tumours are significant and may result in an increased rate of amputations or local recurrences. Timely and accurate diagnosis, along with appropriate intervention, is crucial for optimal outcomes in the management of foot tumours.
The current body of literature on foot tumours primarily consists of sporadic cases, small cohort studies, and case reports detailing both benign and malignant tumours. Notably, there is a scarcity of comprehensive cohort studies focusing specifically on primary tumours of the foot. The limited availability of extensive cohort studies underscores the need for further research and larger-scale investigations to provide a more comprehensive understanding of the epidemiology, diagnostic approaches, and treatment outcomes associated with primary foot tumours. The development of such studies could significantly contribute to advancing knowledge in this domain and inform evidence-based practices for the management of foot tumours.
Methodology
All patients referred to the Orthopaedic Oncology Unit at our institution between 1st January 2010 and 31st December 2020 who had undergone a biopsy or excision due to a lesion in the foot were included in this study. This is a retrospective data analysis of a prospectively collected database. Patients’ demographic data, such as age, gender, size and location of lesion, date of presentation to date of biopsy taken, presence of metastasis, and patient’s final diagnosis, were recorded. A Medical Research Ethics Committee approval (MREC ID: 2018925-6714) was obtained.
All cases were biopsy-proven with Pathological tissue biopsy reviewed by a trained musculoskeletal pathologist. The correlation of clinical and radiological findings aided in concluding a diagnosis of the lesion. The available radiographs were reviewed to scrutinise soft tissue mass, abnormal calcifications or secondary osseous involvement of the lesion. The foot tumours reported in this study were classified based on the World Health Organization (WHO) classification of musculoskeletal tumours. 26
From January 2007 to December 2017, 4997 tumours were treated in all anatomic sites at our centre, and we identified 195 foot tumours (3.90%).
Following history taking and physical examination, patients are subjected to routine blood investigations, followed by conventional radiograph imaging, computed tomography, magnetic resonance imaging, bone scans or angiograms if required. A tru-cut biopsy was carried out for lesions suspicious of malignancy, and the samples were sent for histological examination and confirmation. For benign lesions, an excisional biopsy was performed.
The lesions are categorised according to soft tissue localisation and zones described by Kirby et al. Based on their anatomical classification, an imaginary line was drawn on the lateral projection of a foot radiograph from the metatarsal heads to the insertion point of the Achilles tendon. Another two vertical imaginary lines were drawn, with one from the midtarsal point to the posterior end of the longitudinal plantar arch and another from the metatarsophalangeal joints to the sole. From the lines drawn, four zones can be formed: heel (Zone 1), dorsum of the foot (Zone 2), sole (Zone 3), and toes (Zone 4), as shown in Figure 1.
27
Staging of the tumours diagnosed was done using the Enneking staging system.
28
Subcategorisation of foot tumors according to anatomy.
26

Statistical analysis
For the statistical analysis of the collected data, the incidences and distribution of tumours about the foot were tabulated with Microsoft Excel ® for Windows 10 and SPSS v20 using non-parametric tests. The cases of patients with foot tumours were identified from the registry of the Orthopaedic Oncology Unit and subclassified into benign, malignant, and metastasis lesions. The benign lesions of the foot are divided into benign bone and soft tissue lesions. The malignant lesions of the foot are divided into malignant bone, malignant soft tissue and metastasis (Figure 2). Age distribution of foot tumor.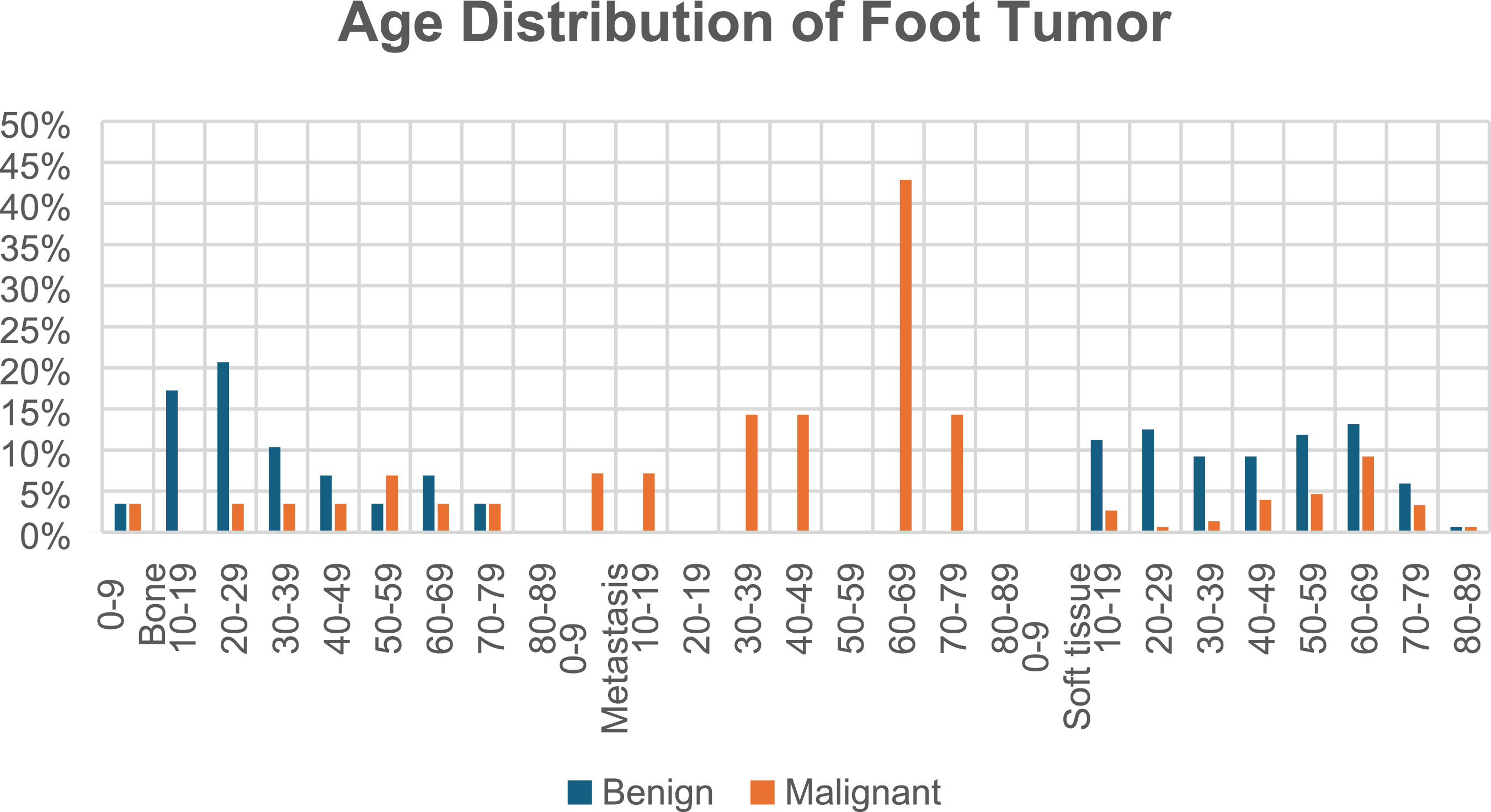
Results
Among the 4997 cases with neoplasms registered in the Orthopaedic Oncology Unit, we identified 266 cases of foot tumours. However, 71 patients were excluded due to incomplete records. Therefore, only 195-foot tumours are included in this study after verifying the exclusion criteria.
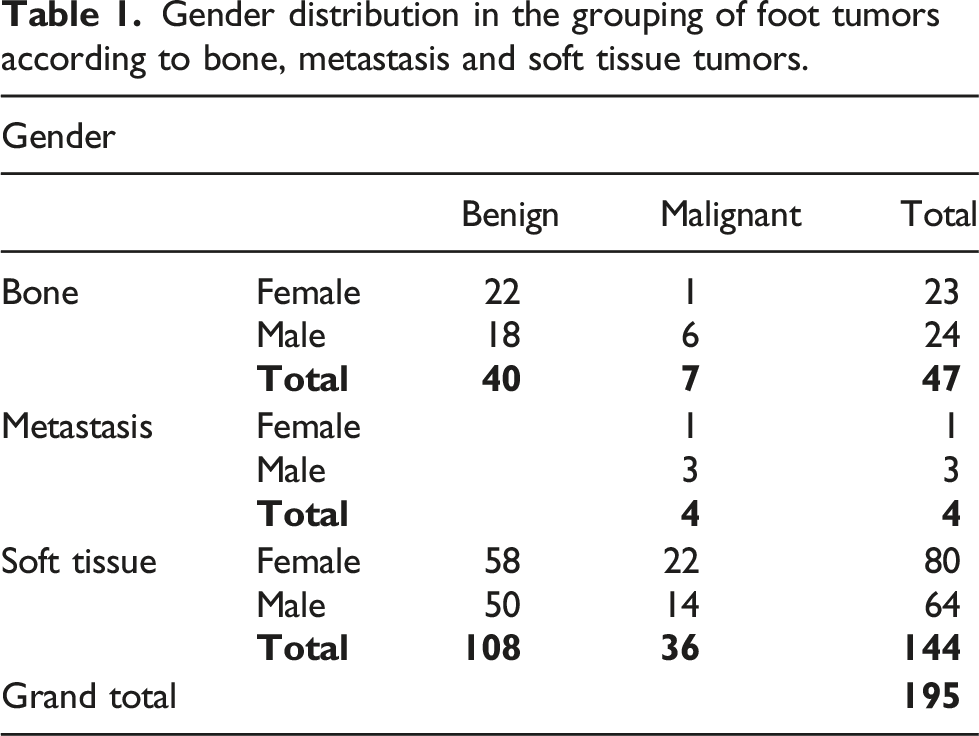
Gender distribution in the grouping of foot tumors according to bone, metastasis and soft tissue tumors.
Age distribution of foot tumors.

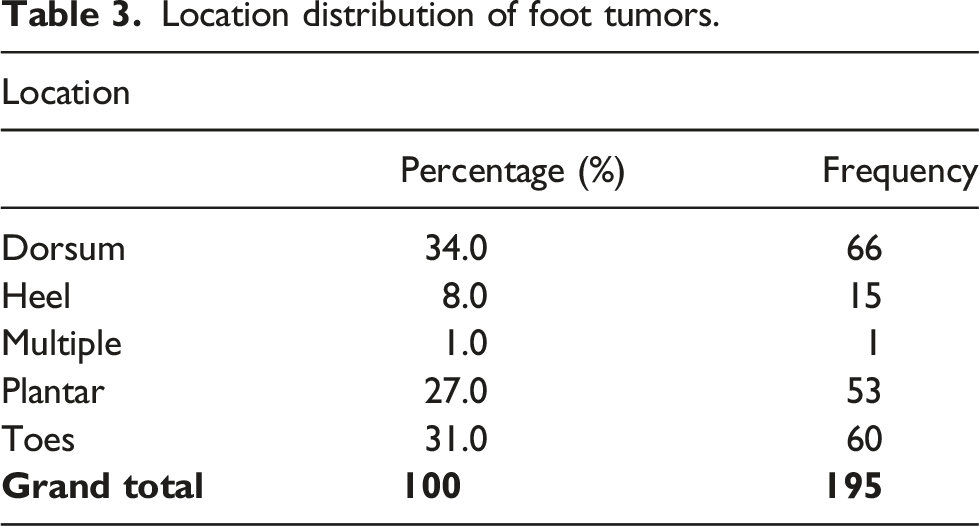
Location distribution of foot tumors.
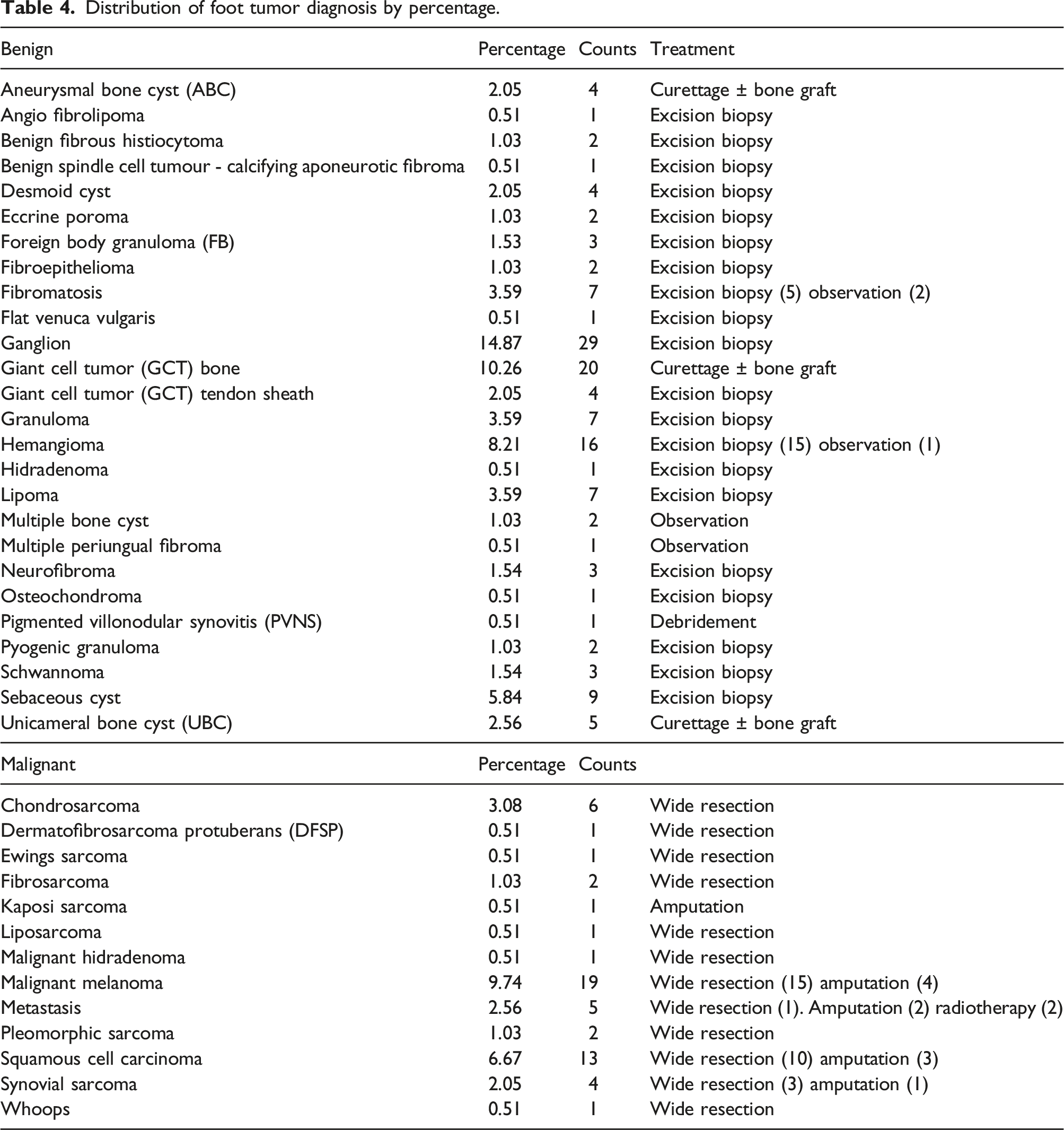
Distribution of foot tumor diagnosis by percentage.
Shows the treatment given.

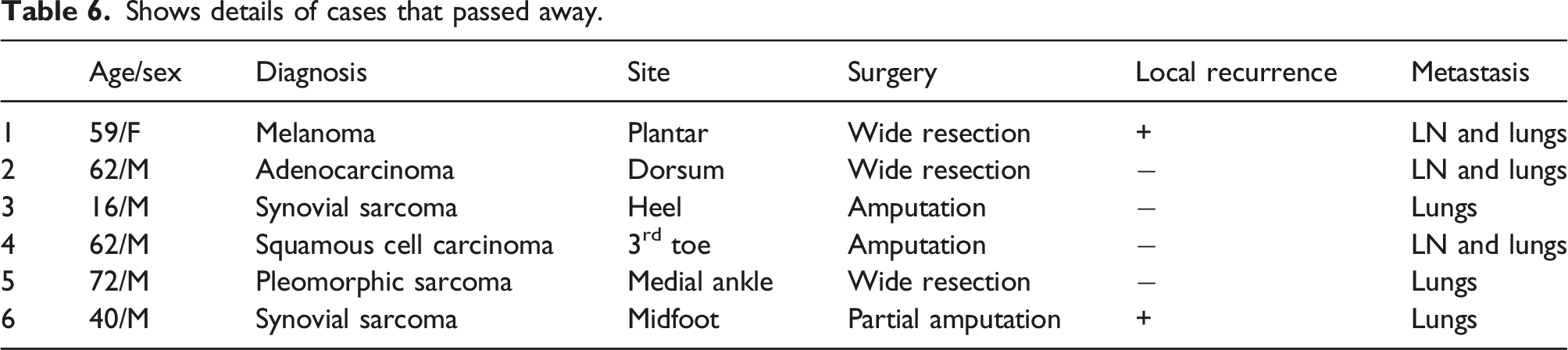
Shows details of cases that passed away.
Discussion
This research endeavour sought to ascertain the incidence and demographic characteristics of foot tumours documented within the confines of our Orthopaedic Oncology Unit. Over the period spanning January 2007 to December 2017, a total of 4997 tumour cases were meticulously catalogued in our database. Among these, 195 cases pertained specifically to foot tumours, constituting 3.90% of the comprehensive dataset under investigation.
The anatomical region comprising the foot is estimated to constitute approximately 3% of the overall body mass. Correspondingly, the incidence of bony neoplasms within the foot is observed to mirror this proportion, with approximately 3% of total bony neoplasms occurring in this anatomical region, as substantiated by references.1,2,18–21 Consistently, our investigative series aligns with this trend.
Shows a comparison between other published series and our study.

NOF: non ossifying fibroma; UBC: unicameral bone cyst; MFH: malignant fibrous histiocytoma; RCC: renal cell Ca; SCC: squamous cell carcinoma; NA: not available.
In our series of 195-foot tumours, there are 47 (24.1%) bone tumours, 4 (2.05%) metastasis and 144 (73.8%) soft tissue tumours, where benign soft tissue tumours predominate. This is in contrast to other fully published series (Table 7), where the majority of the tumours were bone in origin, particularly benign bone tumours. Patients diagnosed with foot tumours show almost similar distributions between males (n = 91) and females (n = 104). This is similar to other published series where there is a slight predominance of either sex with no series showing overwhelming predominance of one sex (Table 7).
The median age observed in our study cohort was 45.6 years, indicating an older demographic profile when compared to certain published series. For instance, the study by Chou et al. reported a median age of 30 years, 11 while Ozdemir et al. 19 documented a median age of 28 years, and Murari et al. 32 reported a median age of 32.6 years. In contrast, the findings from Piertro Ruggieri et al. 20 indicated a median age of 43 years, Karaca et al. 34 reported 42.6 years, and Colterjohn NR et al. 33 documented a median age of 51 years, aligning more closely with the age distribution observed in our investigation.
Benign tumours of the foot exhibit a prevalent occurrence, whereas malignant tumours are notably rare—a pattern consistently observed across various series, including the present study. Within our dataset, ganglions and hemangiomas emerged as the most frequently encountered soft tissue benign tumours of the foot. In contrast, Giant Cell Tumours (GCT) of the bone and Unicameral Bone Cysts were identified as the predominant benign bone tumours of the foot.
However, disparities in tumour prevalence exist when compared to other series. For example, Chou et al. 11 reported GCT as the most common benign bone tumour, with fibromatosis and lipoma dominating as the most common benign soft tissue tumours in their study. Ozdemir et al. 19 documented Osteochondroma as their primary benign bone tumour, with Xanthoma and GCT of the tendon sheath being the prevalent soft tissue tumours. Pietro Ruggieri et al. 20 identified Pseudotumors and Multiple Chondromas as the leading benign bone tumours, while Lipoma and Schwannoma were noted as the primary benign soft tissue tumours. Kirby et al. 26 reported Ganglion and Lipoma as the common benign soft tissue tumours, and Colterjohn NR et al. highlighted fibromatosis as the principal benign soft tissue tumour.
Additionally, Owens et al. 4 emphasized that tumours such as giant cell tumours of the tendon sheath and plantar fibromatosis or inclusion cysts are frequently encountered at the plantar aspect of the foot, contributing to the diverse spectrum of tumour distribution within this anatomical region.
Within our series, the prevailing malignant bone tumour is Chondrosarcoma, while Malignant Melanoma emerges as the predominant soft tissue malignancy. In contrast, other series, as outlined in Table 6, identify Osteosarcoma,11,19,34 Ewing’s sarcoma, 20 and Chondrosarcoma 32 as the most common bone tumours. Regarding malignant soft tissue tumours, Synovial sarcoma is frequently reported in several series,11,20,27,34 with only one series 33 indicating Malignant Fibrous Histiocytoma (MFH) as the primary malignant soft tissue tumour.
Remarkably, our series exhibits a heightened incidence of skin cancers in contrast to sarcomas. This discrepancy may be attributed to referral patterns, with the possibility that other sarcoma units might not be specializing in the management of skin-related malignancies. Alternatively, these cases may be co-managed with units specializing in Plastic or General surgery, thereby influencing the distribution of tumour types within our dataset.
In our investigation, a predominant distribution of tumours is observed on the dorsum of the foot, with subsequent occurrences on the toes, plantar region, heel region, and instances of involvement across multiple regions. Notably, the majority of cases treated at our centre exhibit solitary lesions. However, it is pertinent to acknowledge that specific conditions, such as plantar fibromatosis and multiple lipomatosis, may predispose individuals to the involvement of multiple regions within the foot. This observed trend aligns with findings reported by Kirby, Shereff, and Lewis, 27 corroborating the propensity for certain pathological conditions to manifest as multiple lesions across distinct foot regions.
Patients presenting with foot tumours typically seek medical attention at an earlier stage of the disease, often prompted by an early onset of pain resulting from minor trauma. Ankle sprains are a common complaint among these patients. While plain radiographs are frequently employed to localize the lesion, soft tissue malignant tumours may display asymptomatic characteristics. Given that swellings around the foot are often initially misinterpreted as ganglions, a heightened level of clinical suspicion is crucial.
Prudent staging procedures are essential before embarking on surgical excision of the tumour. Occasionally, specialized views, such as the calcaneal axial view, and non-contrasted computed tomograms, are necessary for a comprehensive assessment of the calcaneum and subtalar joints. Recent advancements in MRI technology have significantly improved the precision of identifying the origin of a soft tissue tumour compared to evaluating the extraosseous extension of a bony tumour.
Healthcare professionals must exercise vigilance, as unplanned excisions are associated with unfavourable outcomes, especially when dealing with any lump over the foot. 31 This underscores the importance of a thorough diagnostic approach and appropriate imaging modalities to guide effective management strategies for foot tumours.
The conventional local treatment of malignant foot tumours was below-knee amputation at different levels. With the current advances in medical technologies, including adjuvant therapy, some patients may benefit from conservative surgery or partial amputation after a multidisciplinary team discussion. The prognosis of foot malignancy is not much different from tumours in other locations. 2
The predominant treatment modality in most cases involved surgical procedures, encompassing excision biopsies, wide resection, or curettage, with or without bone grafting. Conservative management with observation was employed in six patients, and 2 patients with metastatic carcinoma to the bone were treated with radiotherapy. 11 patients (5.64%) underwent amputation, either as a primary or secondary intervention due to disease recurrence. Regrettably, six patients (3.08%) succumbed to the disease, and three cases (1.53%) experienced tumour recurrence.
Notably, our amputation rate was lower compared to other reported series. For instance, Chou et al., 11 Colterjohn NR et al., 33 and Karaca et al. 34 reported higher amputation rates of 20.3%, 16.7%, and 22.0%, respectively. Conversely, our mortality rate aligned with the findings reported by Ozdemir, 19 who documented a rate of 2.1%. It is crucial to consider that Karaca et al. 34 exclusively published a series focusing on malignant bone and soft tissue tumours, resulting in a higher mortality rate of 16%. If we isolate malignant tumours within our series, the mortality rate would be 12.76%. Hence, the observed mortality rates for foot tumours across all published series appear comparable and are contingent on the prevalence of malignant counterparts within each respective dataset.
Functional scores were accessible for 125 patients in our study. The mean Musculoskeletal Tumor Society (MSTS) score for our cohort was 79% (range: 63%–93%), and the Toronto Extremity Salvage Score (TESS) averaged at 76.23% (range: 56%–84%). Unfortunately, comparative analyses with other series are limited, as the publication of functional scores is not widespread. Notably, one series focusing on soft tissue tumours by Colterjohn et al. 33 reported an average MSTS score of 88.57% at 12 months post-surgery. This provides a valuable reference point for the assessment of functional outcomes in the context of soft tissue tumours.
The retrospective nature of this study inherently imposes limitations, as it introduces potential variability in the accuracy and completeness of the data recorded in medical records. The exclusion of patients with incomplete records exacerbates this limitation, as it may introduce a source of bias. Additionally, the reliance on medical records from the pathology department for case selection resulted in the exclusion of tumours treated with lesion destruction through thermal ablation, such as osteoid osteoma, which may have impacted the comprehensiveness of the dataset. Furthermore, the study faces a constraint in the limited exploration of functional outcomes for patients with lower extremity tumours, and the relatively small sample size in this subgroup may limit the generalizability of findings. Consequently, the study does not provide a comprehensive reflection of overall foot function. To address this limitation, future investigations could consider incorporating specific scoring systems, such as the Foot Function Index (FFI) for foot tumours, or the American Academy of Orthopaedic Surgeons (AAOS) scoring system, to offer a more nuanced and standardized evaluation of the functional outcomes associated with foot tumours.
In conclusion, foot tumours are relatively rare, with the majority originating from soft tissue and exhibiting a benign nature. Nonetheless, a noteworthy proportion—approximately a quarter of these tumours—demonstrate malignancy. Thus, accurate differentiation between malignant and benign tumours is imperative, as misdiagnosis and inappropriate treatment can lead to unfavourable outcomes. The surgical interventions undertaken in the management of these tumours, along with the associated functional outcomes, generally yield acceptable results. Ongoing vigilance and comprehensive diagnostic approaches are crucial in optimizing the prognosis and treatment outcomes for individuals with foot tumours.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.