
Abstract
Purpose
This study aims to systematically review the efficacy and safety of total ankle replacement (TAR) and ankle fusion (AF) as treatment options for end-stage ankle arthritis.
Methods
A comprehensive literature search was conducted on data from multiple databases, including PubMed, The Cochrane Library, Construction and Building Materials, Embase, Web of Science, and Scopus for RCTs and prospective cohort studies comparing TAR and AF in patients with end-stage ankle arthritis from inception up to June, 2023. Our primary outcomes of interest included patients’ clinical function scores and complications. We employed Review Manager 5.4 and Stata/MP 14.0 software for the meta-analysis.
Results
Our analysis incorporated 13 comparative studies, including 11 prospective studies, one pilot RCT, and one RCT. The pooled results revealed no significant difference in postoperative Short Form-36 scores between the TAR and AF groups (MD = −1.19, 95% CI: −3.89 to 1.50, p = .39). However, the postoperative Foot and Ankle Ability Measure scores in the AF group were significantly higher than in the TAR group (MD = 8.30, 95% CI: 1.01–15.60, p = .03). There was no significant difference in postoperative complication rates between the TAR and AF groups (RR = 0.95, 95% CI: 0.59 to 1.54, p = .85).
Conclusion
Currently available evidence suggests no significant disparity in postoperative outcomes between TAR and AF. In the short term, TAR demonstrates better clinical scores than AF and lower complication rates. Conversely, in the long term, AF exhibits superior clinical scores and lower complication rates, although this difference is not statistically significant.
Introduction
Osteoarthritis (OA) primarily arises from the degradation and damage to articular cartilage. While not as prevalent as hip and knee arthritis, ankle arthritis affects approximately 1% of adults worldwide.1–4 It is often observed in individuals with a history of ankle fractures and ligament injuries around the ankle joint, resulting in symptoms like joint pain and restricted ankle movement and function. 5 During its initial stages, conservative non-surgical approaches, such as weight management, medications, and physical therapy, can alleviate symptoms and slow disease progression. 6 However, in advanced cases, conservative treatments yield limited benefits, prompting the consideration of surgical interventions such as arthroscopic joint debridement, microfracture, 7 osteochondral grafting, 8 distraction arthroplasty, 9 periarticular osteotomy, 10 ankle fusion (AF) and total ankle replacement (TAR). Currently, TAR and ankle fusion represent the predominant strategies for addressing end-stage ankle arthritis, with ankle fusion still being regarded as the “gold standard” by many researchers.
Many researchers favor ankle fusion due to its evident therapeutic effects, which enable patients to regain normal daily activities.11,12 Nevertheless, it entails joint resection and fusion of the tibia and talus, resulting in biomechanical alterations in the ankle joint, a loss of ankle motion function, and an increased risk of joint degeneration surrounding the ankle. 13 To mitigate biomechanical changes and preserve ankle motion function, TAR was introduced as an alternative to ankle fusion in the 1970s. 14 With ongoing technological advancements, statistics indicate that TAR can deliver excellent or good outcomes for over 80% of patients, while 72% of patients who undergo ankle fusion achieve excellent or good results. 15 Consequently, the debate regarding the comparative advantages of TAR and ankle fusion in ankle arthritis treatment persists.
Although many studies have attempted to compare the advantages of TAR and AF, no randomized controlled trials (RCTs) were included, and their findings were based on retrospective and prospective studies. To our knowledge, no research has hitherto exclusively focused on prospective studies, and a comprehensive analysis of the current status of these two surgical options is warranted. An increasing body of evidence suggests no substantial disparities in functional scores and complication rates between TAR and ankle fusion in ankle arthritis treatment.16–18 However, some studies, such as those by Kim et al. 19 and Shih et al., 20 have suggested higher complication rates associated with TAR. Liu et al. 21 reported that TAR exhibited superior clinical scores and lower complications in short-term follow-ups but found no difference in clinical scores between the two methods in long-term follow-ups. Indeed, the inclusion of both prospective and retrospective studies may introduce selection bias, which could affect the comparative outcomes of TAR and ankle fusion.
This study aims to systematically assess the effectiveness and safety of TAR and ankle fusion in treating end-stage ankle arthritis. We conducted a meta-analysis of comparative studies to ascertain whether significant differences exist between the two surgical approaches in terms of (1) clinical functional scores and (2) complication rates. We aimed to provide a more robust scientific foundation for clinical decision-making and ultimately enhance the care and outcomes for patients with ankle arthritis.
Methods
Search strategies
This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines established in 2020. 22 We conducted computerized searches of multiple databases, including PubMed, The Cochrane Library, China Biology Medicine (CBM) databases, Embase, Web of Science, and Scopus, to identify comparative studies involving ankle replacement and ankle fusion for patients with ankle osteoarthritis. The search period spanned from the inception of the databases to June 2023. The search queries employed a combination of subject terms and free-text keywords. The English search terms comprised “replacement,” “arthroplasty,” “ankle,” “fusion,” and “Arthrodesis,” among others. The Chinese search terms included “ankle,” “replacement,” “fusion,” etc.
Inclusion and exclusion criteria
First, we eliminated irrelevant and duplicate records based on title, abstract, and keyword assessments. Subsequently, the remaining literature was thoroughly reviewed. The final selection was made in accordance with predetermined inclusion and exclusion criteria. The inclusion criteria were as follows: (1) The intervention group consisted of individuals who underwent TAR, and the control group consisted of individuals who underwent ankle fusion; (2) The study outcomes encompassed at least one of the following: clinical scores or complications; (3) Studies reporting clinical scores must include mean and standard deviation; (4) Prospective studies or RCTs; (5) Clear reporting of the number of participants in each group. Studies lacking outcome data were excluded, as were those dealing with pathological fractures and duplicate publications.
Study selection and data collection
Two authors independently extracted relevant patient-related information, including: (i) first author, publication date, study location, study design, participant count in each group, gender distribution, mean age, body mass index (BMI), and average follow-up duration; (ii) postoperative clinical functional scores; (iii) postoperative complications. In case of disagreements, the two authors resolved them through discussion. The extracted outcomes comprised clinical functional scores, including Short Form-36 (SF-36), Foot Ankle Ability Measure (FAAM), and Visual Analog Scale (VAS), among others.
Study risk of bias assessment
Two authors independently assessed the quality of the included studies using the Newcastle-Ottawa Quality Assessment Scale. 23 This scale comprises three primary domains: selection, comparability, and outcome, with eight total items. The selection domain incorporates four items, each with a maximum score of one point, comparability includes one item with a maximum of two points, and outcome involves three items, each with a maximum score of one point.
Statistical analysis
Statistical analyses were conducted using Review Manager 5.4 and Stata/MP 14.0 software. As the follow-up durations in various studies were not uniform, standardized mean difference (SMD) and its 95% confidence interval (CI) were used to assess continuous variables, while risk ratio (RR) and its 95% CI were employed for dichotomous variables. Heterogeneity among study results was assessed using the χ2 test (α = 0.1), and the I2 value was used to quantify the extent of heterogeneity. A fixed-effects model was applied for meta-analysis when no statistical heterogeneity was detected. In the presence of statistical heterogeneity, further analysis was conducted to identify and address any clinical heterogeneity. Finally, a random-effects model was used for meta-analysis, and subgroup analyses were performed based on different follow-up durations, clinical function scores, and complications.
Results
A total of 2243 relevant documents were identified in the initial search, resulting in 2006 articles after eliminating duplicates. After reviewing titles, abstracts, and keywords, 233 articles were excluded from the meta-analysis and review. Out of the remaining 1714 articles, 12 were excluded due to the unavailability of the original text. Subsequently, 47 documents were subjected to a detailed full-text examination, excluding 34 papers. The specific reasons for exclusion are detailed in Figure 1. Ultimately, 13 studies16,24–35 met the criteria for inclusion in our meta-analysis. A flowchart of the literature screening performed in this study.
Study characteristics
Baseline characteristics of included studies.

TAR: Total Ankle Replacement; AF: Ankle Fusion; RCT: Randomized Controlled Trial; NR: Not reported. Outcomes: 1, Buechel-Pappas ankle score (BP score); 2, Visual Analog Scale (VAS); 3, Short Form-36 scores six Dimensions (SF-6D); 4, American Orthopedic Foot and Ankle (AOFAS); 5, Short Form-36 scores (SF-36); 6, Ankle Osteoarthritis score (AOS); 7, Musculoskeletal Function Assessment (MFA); 8, Pain score; 9, Foot Ankle Ability Measure score (FAAM); 10, Manchester–Oxford Foot Questionnaire (MOXFQ); 11, EuroQol Group 5-Dimension 5-Level (EQ-5D-5L); 12, complications.
Quality assessment of included studies according to the Modified Newcastle–Ottawa scale.

Clinical function scores
Seven studies24–27,30,31,33 reported SF-36 scores, and after excluding duplicate studies and data with varying follow-up times, two studies25,27 were included, comprising a total of 358 patients (TAR: n = 251, AF: n = 107). The random-effects model meta-analysis revealed no significant difference in postoperative scores between the TAR and AF groups (MD = −1.19, 95% CI: −3.89 to 1.50, p = .39) (Figure 2). Four studies16,30,31,33 provided FAAM scores, and after excluding data from different follow-up periods within the same studies, two studies16,30 were included, encompassing 773 patients (TAR: n = 531, AF: n = 242). The meta-analysis using a random-effects model demonstrated that the postoperative score of the AF group was significantly higher than the TAR group (MD = 8.30, 95% CI: 1.01–15.60, p = .03) (Figure 3). Considerable heterogeneity was observed due to variations in study design and geographic location. Forest plot for postoperative PCS score of SF-36. SF-36: Short Form-36; PCS: physical component summary subscale; TAR: Total Ankle Replacement; AF: Ankle Fusion. Forest plot for postoperative ADL of FAAM. ADL: activities of daily living; FAAM: Foot and Ankle Ability Measure; TAR: Total Ankle Replacement; AF: Ankle Fusion.

Complications
Eight studies16,25–27,29–32 reported complications. After excluding data from different follow-up periods within the same study and cases where multiple complications in the same patient led to a complication rate greater than 1, six studies16,25–27,29,30 were included, covering 1217 patients (TAR: n = 831, AF: n = 386). The meta-analysis using a random-effects model revealed no significant difference in the incidence of postoperative complications between the TAR and AF groups (RR = 0.95, 95% CI: 0.59–1.54, p = .85) (Figure 4). Further subgroup analyses were conducted to assess the credibility of the studies due to variations in study design and follow-up times. Sensitivity analyses of TAR and AF complication rates (Supplemental Figure 1) indicated no significant difference in overall complication rates between TAR and AF. The funnel plot analysis also showed no evidence of publication bias (Supplemental Figure 2). Subgroup analysis based on follow-up duration revealed a significant difference in the incidence of postoperative complications between the TAR and AF groups at the 24-month follow-up (Figure 5). Forest plot for total complication rate. TAR: Total Ankle Replacement; AF: Ankle Fusion. Forest plot for complication rate at different follow-up times. TAR: Total Ankle Replacement; AF: Ankle Fusion.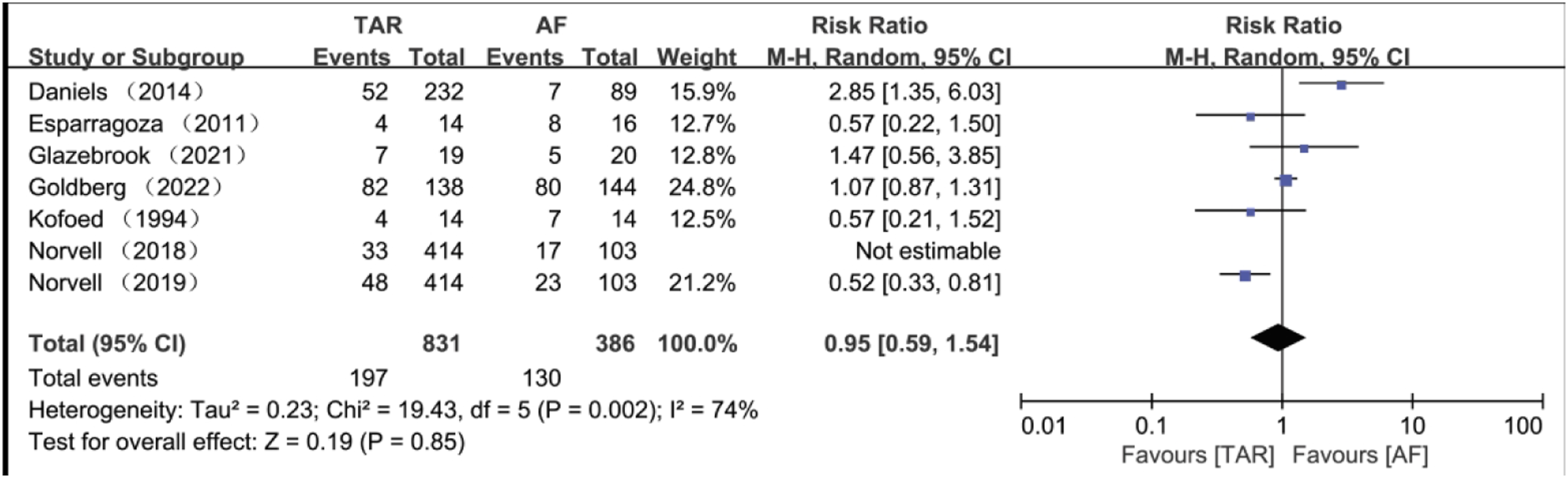

Discussion
The mainstay of treatment for patients with end-stage ankle arthritis remains TAR and AF. 12 While AF is widely regarded as the “gold standard” for end-stage ankle arthritis, it has limitations, mainly due to the associated loss of ankle motion range. 13 Numerous studies have sought to compare the outcomes of TAR and AF, but the findings have been quite diverse.18–21,36,37 Prior research often combined prospective and retrospective studies for analysis, prompting us to exclusively include prospective studies for our meta-analysis.
Our meta-analysis demonstrated that, during a 1-year follow-up, TAR yielded significantly higher Foot and Ankle Ability Measure-Activities of Daily Living (FAAM ADL) clinical scores compared to AF. The difference in FAAM ADL scores between TAR and AF was 8.30 (CI: 1.01–15.60), consistent with the results of Norvell et al., 30 who reported a nine-point difference, and Goldberg et al., 16 with a six-point difference. However, other clinical scores, such as SF-36, did not reveal significant differences during follow-up, which is in accordance with findings from studies by Fanelli et al., 36 Li et al., 18 Kim et al., 19 and Shih et al. 20 Notably, AF has been reported to benefit clinical functional scores in long-term follow-up. 38 Our results indicate that while AF may provide a long-term clinical score advantage, this advantage does not reach statistical significance. This observation might be linked to the substantial sample size when simultaneously analyzing prospective and retrospective studies.
Our study suggests that the overall complication rate of TAR is not significantly different from that of AF. However, during subgroup analysis based on follow-up times, we observed a significantly lower complication rate for TAR at the 2-year mark compared to AF (RR = 0.53, CI: 0.35–0.79), which is in line with the results of short-term complication rates (complications occurring within 2 years) investigated by Liu et al., 21 which indicated an RR of 0.67. While some reports have indicated higher complication rates for TAR in long-term follow-up,25,39,40 our study observed a higher complication rate for TAR compared to AF, although the difference was not statistically significant. The limitations of the present study should be acknowledged. Firstly, the number of TAR was significantly higher than the number of AF in this paper, which was due to the fact that in some of the prospective studies, random allocation was not fully followed, and most studies indicated that the study is a prospective study rather than a completely prospective randomized controlled study, and the decision whether a patient enters the TAR or AF group is jointly decided by the doctor and the patient. Secondly, the heterogeneity of the results was relatively high despite the subgroup analysis, which may be related to our relatively small overall sample size and the fact that we did not differentiate between the different designs of TAR techniques and analyzed all TAR techniques together. Some studies have indicated that different designs of TAR techniques have different effects, with newer TAR designs doing better than older TAR designs.41–43 Thirdly, although some studies have found that arthroscopic AF is superior to open AF,44,45 the AF techniques in this paper do not clearly distinguish between arthroscopic AF techniques and open AF, which is because AF was not fixed as an arthroscopic or open AF protocol in the prospective studies, and mostly the operator decided to perform arthroscopic AF or open AF based on the actual situation. Finally, clinical function scores differ significantly between countries, with relatively few standardized clinical scores, potentially introducing bias in comparing the two groups. Nonetheless, our study benefits from including only prospective studies, including RCTs for meta-analysis, enhancing the evidence level.
In conclusion, TAR demonstrates superior clinical function scores and complication rates in the short term. However, AF appears to perform better over a longer duration, albeit with a modest margin. The limitations in both the quantity and quality of the encompassed studies warrant further exploration through high-quality research to validate these conclusions.
Supplemental Material
Supplemental Material - Total ankle replacement versus ankle fusion for end-stage ankle arthritis: A meta-analysis
Supplemental Material for Total ankle replacement versus ankle fusion for end-stage ankle arthritis: A meta-analysis by Taiyi Li, Li Zhao, Yan Liu, Li Huang, Jin Zhu, Jie Xiong, Junfeng Pang, Lina Qin, Zonggui Huang, Yinglong Xu and Hai Dai in Journal of Orthopaedic Surgery
Footnotes
Author contributions
T.L.: literature search, data extraction, writing; L.Z.: data extraction, writing; Y.L. and L.H.: methodological quality assessment; J.Z., J.X., J.P., and L.Q.: statistical analyses; Z.H.: supervision; Y.X.: literature search, supervision, revision, final approval; H.D.: supervision, revision, final approval. All authors have read and approved to the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
Data availability statement
This study does not contain any third material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.