
Abstract
Purpose
To describe the implementation and evaluation of a hospital-initiated, community-based, digital prehabilitation program (My PreHab Program: MPP) for adults referred for elective joint replacement.
Methods
MPP was implemented July 2022 and comprises a personalised digital health screen that guides the provision of self-management resources. Adults (
Results
Of those invited (N = 689), 77.8% participated. Participants and non-participants were similar in key demographic variables except regional invitees were more likely to participate than metropolitan (88.0% vs 75.4%, p = .002) and non-participants tended to be older (median age = 69.0 vs 64.0, p = .005). Participants reported on average four modifiable risk factors: most commonly chronic pain (79.1%), obesity (57.3%), and frailty (40.9%). Most participants (80.4%) reviewed all resources provided and reported action/intention to address issues identified (90.9%). Participants perceived MPP as acceptable (3.2/5), appropriate (3.3/5), and feasible (3.4/5). Early trends for participants progressing to surgery (n = 33) show a reduced length of stay (MPP = 4.3, baseline = 5.3 days).
Conclusion
MPP demonstrated high adoption, fidelity, and participant engagement. It is acceptable, appropriate and feasible and has the potential to be scaled-up digitally at low-cost. Modifiable risk factors were prevalent and early indications suggest this preoperative intervention may benefit both patients and the healthcare system.
Keywords
Introduction
Osteoarthritis (OA) of the knee and hip joints can result in severe pain, disability and loss of function and its prevalence is increasing globally.1,2 Advanced knee and hip OA is commonly managed with Total Knee Replacement (TKR) and Total Hip Replacement (THR) procedures. 3 With surgical rates for TKR and THR increasing around the world, the predicted cost to the health system will exceed AUD$5.32 billion by 2030 for procedures alone.4,5 During an acute admission, post-operative complications occur in 12% of TKR patients and 11.2% of THR patients. 6 By six months post-surgery, this figure has increased with many patients experiencing at least one complication (TKR = 53.6%, THR = 39.7%). Complication rates are predicted to increase 10% each year due to population-based increases in ageing and medical comorbidities. 7 The resultant burden on the health and wellbeing of patients, families, and the healthcare system is significant and includes worse psychosocial outcomes, delayed functional recovery, mortality and financial costs.8–11 Many hospital acquired complications can be avoided and surgical outcomes enhanced by supporting improvements in health and wellbeing prior to surgery through prehabilitation (prehab). 12 The use of digital technology to identify risk factors and empower patients to improve their health and wellbeing before planned surgery may be a cost-effective way to improve patient outcomes and health system performance.
Prehab is any intervention that is provided before surgery to address modifiable risk factors and enhance general health and/or wellbeing prior to surgery.12,13 Modifiable risk factors for joint replacement surgery include obesity, diabetes, smoking, anaemia, and opioid use. 14 Data from the national joint registry highlights an increased risk of revision for infection associated with increasing American Society of Anaesthesiologists (ASA) score and Body Mass Index (BMI) category. 15 Examples of recommended interventions include delaying TKR or THR until BMI <40, a targeted glycated haemoglobin (HbA1c) of ≤53 mmol/mol, smoking cessation (at least four weeks before an operation), oral iron supplementation or intravenous iron transfusion, and avoiding the use of opioids. 14 Education and exercise programs have been shown to improve pain and function in patients with OA and exercise and cognitive behavioural therapy are evidence based treatments for chronic pain.16,17 Although core prehabilitation components have been identified, more research is needed to determine the most effective combination of interventions, as well as timing, and mode of delivery.
Individual, in-person, prehab is resource intensive and costly, making it challenging to sustain in public health services. It is also often cost-prohibitive on a private basis, making it inaccessible for a large portion of the population. However, digital technologies to remotely support home-based prehab across a variety of conditions can provide cost-effective alternatives that are feasible, effective and acceptable to patients.18,19 Emerging research into websites and mobile apps for knee OA has demonstrated their effectiveness in supporting people to manage symptoms and improve function. 20 There are also a growing number of free online programs improving access to evidence-based interventions.21,22 Digitally facilitated prehab interventions offer potential advantages over older models, with the opportunity for rapid dissemination and uptake, flexibility for patients and staff and the ability to be scaled up rapidly with minimal additional expense. 23
Wait times for elective surgery are long in most public health systems, with patients frequently experiencing significant periods of time on ‘hidden’ outpatient and surgical waitlists.
24
Many people with severe joint disease wait months to years for surgery and over half experience a deterioration in health-related quality of life during this period.25,26 As this waiting period is often a passive stage, it offers an opportunity to leverage the potential upcoming surgery as a key motivator for behaviour change (through prehab) and thus improve surgical outcomes.
27
A simplified typical surgical journey with prehab included is depicted in Figure 1, however, it is acknowledged the path to surgery may not be linear. The typical surgical journey.
Given long waiting times and the need for a cost-effective approach to reduce post-operative complications and improve surgical outcomes, we saw an opportunity to design and trial a hospital-initiated, community-based, digital program (My PreHab Program: MPP) for people placed on outpatient appointment and surgical waitlists who were referred for TKR or THR surgery. This preliminary report provides an overview of MPP cohort characteristics, implementation measures described by Hermes et al. 28 (program levels of adoption, reach, acceptability, appropriateness, feasibility, fidelity), patient reported engagement in health behaviours and preliminary surgical outcomes.
Methods
Setting
MPP was implemented across two metropolitan public hospitals in the largest health network in South Australia (Central Adelaide Local Health Network: CALHN). Together, these sites perform hundreds of joint replacement operations annually (391 in 2022).
Eligibility
Individuals were invited to participate if: (a)
Intervention
The co-design and initial user testing of MPP with patients, clinical experts and key stakeholders, is reported elsewhere. 29 In brief, MPP is a digital patient pathway that comprises a study specific health screen completed by patients (Health Assessment Questionnaire: HAQ, Supplement A) to identify modifiable risk factors and guide the provision of targeted, practical resources to empower self-management and/or facilitate access to primary care supports. It also includes a summary report and progress check-ins. Participants are informed about the long wait for surgery and the potential benefit of prehab at the outset. Examples of information provided to participants can be viewed on our companion website, www.calhn-prehab.sa.gov.au. Participation was voluntary with all participants providing informed consent digitally. Non-participants received usual care consisting of no proactive pre-surgery health optimisation strategies, other than that provided by individual clinicians either in primary care or at surgical review.
Patients were invited to MPP from July 1, 2022, to June 30, 2023, with two entry points available during the defined prehab period (Figure 2). The primary entry was at the point of placement on the outpatient waitlist following usual referral triage (Outpatient Waitlist Entry Point: Outpatient-WEP). The second entry point was for patients who had already been reviewed by a surgeon and placed on the surgical waitlist, thus providing broader access to the program (Surgical Waitlist Entry Point: Surgical-WEP). Initial check-in for the Surgical-WEP group occurred 2-months post referral and all participants (Outpatient-WEP and Surgical-WEP) then received 6-monthly follow-ups (Supplement C). Only data from the first check-in scheduled in the 12-month period were reported on. Opportunities for feedback occurred at 2-weeks post registration (Patient Experience Questionnaire: PEQ, Supplement B) and 6-weeks post-operatively (Post-Operative Feedback: POF, Supplement D). All feedback provided by participants who registered within the 12-month period were analysed. Questionnaires were study specific and are available in the supplemental materials. MPP digital pathway.
As part of standard clinical practice across both units, all HAQ responses were reviewed prior to waitlist allocation. Referrals could be declined by triaging clinicians if the patient reported information did not meet departmental referral guidelines. For declined referrals, access to MPP pathways was terminated four weeks post registration. However, data collected prior to termination (e.g., HAQ and PEQ responses) were retained in analyses to inform broad understanding of the referred cohort.
Cohort characteristics
Detailed participant health characteristics were collected from the HAQ and included general medical (comorbidity) and study specific modifiable risk factor screening. These included emotional wellbeing, smoking status, presence of chronic pain, alcohol, drug and medication use, iron deficiency/anaemia history, frailty, exercise and physical activity levels, diabetes management and awareness and utilisation of equipment and community services. The questions and descriptions for each category are available in Supplement A. Frailty screening was included in the questionnaire using the FRAIL Scale. 30 The HAQ also asked participants to rate their confidence in their ability improve their health before surgery and their desired level of support.
Implementation outcome measures
Implementation measures for behavioural intervention technologies described by Hermes et al. 28 guided the evaluation of the implementation and served as intermediate outcomes, with relevant measures outlined below.
Adoption
Patient adoption of MPP was measured by registration and participation and was automatically captured by the digital pathway. Participation was deemed to have occurred upon completion of the HAQ.
Fidelity
The extent to which the MPP platform was used by participants as intended was automatically collected and assessed by the percentage of eligible individuals completing planned questionnaires or activities at key check points; registration (completion of HAQ and provided topics), 2-weeks post registration (PEQ), 2- or 6-months post registration (initial check-in) and 6-weeks post-operatively (POF). All individuals who registered for MPP received the PEQ, only those accepted by the clinical units and placed on the relevant waitlist received the initial check-in.
Equity of reach
Standard demographic information of invitees was compared between participants and non-participants to identify any barriers to participation. The Index of Relative Socio-economic Disadvantage (IRSD) was used to explore program reach to disadvantaged areas (a score of one represents the most disadvantaged and ten the least). 31
Acceptability, appropriateness and feasibility
.Patient perception of acceptability, appropriateness and feasibility were measured via questions defined by Weiner et al. 32 in the PEQ and POF (Supplement B, D). Questions were measured on a 5-point Likert Scale and assigned values ranging from one to five. Scores were averaged with higher scores indicating greater levels of acceptability, appropriateness, or feasibility. As validated cut-off scores were not available, the authors determined the minimum threshold for each measure was a mean of >3. Study specific questions were also included exploring factors such as perceived ease of usability and patient experience with the platform (Supplement B, C, D).
Intervention outcome measures
Patient reported engagement in health behaviours
Patient-reported engagement with MPP’s core messages were assessed via the PEQ, check-ins and POF. Behaviours of particular interest included seeing their General Practitioner (GP) to discuss MPP specific content and having taken action to reduce risk factor(s) (Supplement B, C, D).
Preliminary surgical outcome data
Length of stay (LOS) data for participants who had a TKR or THR operation in the reporting period were obtained from the hospital’s CALHN electronic medical record system. Average LOS for MPP participants (both TKR and THR) was compared with CALHN data from the same time period (excluding MPP participants, 2022/2023 financial year: FY 22/23) and the year preceding implementation of MPP (2021/2022 financial year: FY 21/22).
Data analysis
Data were analysed using IBM SPSS Statistics (Version 29). Descriptive statistics were used to understand the demographic and clinical characteristics of the sample and evaluate outcome measures. Associations between demographic data for participants and non-participants, and cohort characteristics for females and males were analysed with the threshold for statistical significance set at p < .05. Fisher’s Exact Test (2-sided) was applied to categorical data in 2 × 2 contingency tables, with odds ratios (OR) along with their corresponding confidence intervals (CI) calculated. 33 Chi-square was used for larger contingency tables, with Cramer’s V used for effect size calculations. 34
Ethics approval
The design, development and user-testing was approved by the CALHN Human Research Ethics Committee (HREC) (approval #15507). 29 From July 1, 2022, the project was regarded by CALHN HREC as an evaluation of a quality improvement initiative and have provided publication approval (approval #18901).
Results
Adoption
Of the 689 individuals invited to participate in MPP during the initial 12-month period, 547 (79.4%) registered and the majority (n = 536) went on to participate (Figure 3). Thirty-six referrals were then declined due to high BMI following clinician review of the HAQ, resulting in a final sample of 500 participants (Outpatient-WEP = 447, Surgical-WEP = 53). There was no significant difference between intake groups (Outpatient-WEP, Surgical-WEP) on any of the key characteristics (demographic, cohort) and as such, data were collapsed and examined as a single patient cohort. Patient flow of study cohort.
Equity of reach
Baseline demographics for MPP participants and non-participants.

Abbreviations: IQR, interquartile range; THR, Total Hip Replacement; TKR, Total Knee Replacement; IRSD, index of relative socioeconomic disadvantage. NB: Numbers represent n (%) unless specified by * to represent years.
Cohort characteristics
Cohort characteristics.

Abbreviations: BMI: body mass index.
aIncludes multiple selections.
bMobility scooter, wheelchair or knee scooter.
Activity levels were low, with nearly two thirds of participants reporting they were either ‘a little’ or ‘not very active’ (65.5%) and 42.2% of participants classified as ‘frail’. This was exemplified by 57.1% advising that they were unable to ‘walk around the block’ (300 m) unaided. The complexity of this cohort was further highlighted by the presence of additional health conditions outlined in Table 2, including diabetes (19.4%), heart disease (18.5%) and/or unspecified ‘serious’ comorbidities (16.8%).
Participant reported confidence to improve health prior to surgery and amount of support desired.

Fidelity
Following completion of the HAQ, all participants were provided with a summary report and targeted health information based on their responses. Engagement with this information was high, with 85.6% accessing the summary report and 80.4% viewing all information provided. At least one health topic was viewed by 89% of participants. As seen in Figure 4, when information about modifiable risk factors was generated for participants to review, they were all consistently accessed by participants. Health information provided versus accessed by participants.
Most participants completed feedback questionnaires scheduled at 2-weeks post registration (n = 396/536, 73.9%) and 6-weeks post-operatively (n = 25/33, 75.8%) (Figure 3). The first progress check-in at 2- and 6-months post-registration for Surgical-WEP and Outpatient-WEP participants, respectively, was completed by 117 participants (n = 305, 41.2%).
Acceptability, appropriateness and feasibility
At 2-weeks post registration, most respondents reported no problems accessing or using the digital MPP platform (75.3%). MPP scored an average of 3.2 for acceptability, 3.3 for appropriateness and 3.4 for feasibility (out of 5). Participant responses for each measure are shown in Figure 5, with the majority either reporting they ‘neither agreed nor disagreed’ or ‘agreed’ with the statements. Many responders found the MPP content ‘useful’, including the summary report (64.4%) and targeted health information (55.6%). However, at the first progress check-in, participants had mixed responses about MPP information assisting with health improvements in the preceding 2- or 6-month period, with 28.2% ‘agreeing’, 32.4% ‘unsure’, and 39.3% ‘disagreeing’ that it had helped. Acceptability, appropriateness and feasibility of MPP at 2-weeks post registration.
When participants reflected on their experience 6-weeks following their joint replacement (n = 25/33), average scores for acceptability (3.8 out of 5), appropriateness (3.9 out of 5), and feasibility (3.7 out of 5) all improved. As seen in Figure 6, 72.0% responded they either ‘agreed’ or ‘completely agreed’ it was acceptable and appropriate, and 68.0% felt it was feasible. Similarly, respondents’ beliefs about MPP helping them to prepare for surgery improved, with seven ‘agreeing’ and fourteen ‘strongly agreeing’. Most (80%) indicated they would be likely to recommend MPP to friends and family if they required surgery (‘likely’ = 10, ‘very likely’ = 10). Acceptability, appropriateness and feasibility of MPP post-operatively.
Patient reported engagement in health behaviours
At 2-weeks post registration, respondents reported high engagement levels with their GP specifically in relation to MPP recommendations. Most (86.6%) advised that they had either ‘seen’ (41.2%), ‘booked an appointment’ (20.2%) or ‘planned to see’ (25.3%) their GP and many (59.3%) reported they had started optimising health areas identified in their summary report. A further 31.6% indicated that although they hadn’t started, they had plans to commence optimisation.
Participant reported engagement with their GP remained high at the first check-in, with 79.5% indicating they had discussed the identified health areas with their GP. However, progress in addressing health areas was varied; 23.1% advised they had implemented the health recommendations identified in their summary report, while 53.0% still had progress to make. Only 6% did not intend to work on identified areas and despite all participants receiving information on at least one modifiable risk factor, 17.9% responded ‘no health areas were identified’. The most prevalent health areas perceived to have already been optimised or in progress were activity and exercise (28.2%), pain management (28.2%) and nutrition and weight optimisation (21.5%) (Figure 7). These health categories were similarly identified as priority areas by participants who had not started optimisation but planned to. Participant progress in optimising health at initial check-in.
Post-operatively, nearly all respondents (96%) advised that prior to surgery they had worked on improving health areas identified.
Preliminary surgical outcomes
Thirty-three participants (6.6%) had TKR/THR surgery within the 12-month period (Outpatient-WEP = 13, Surgical-WEP = 20). More TKRs than THRs were completed (TKR = 20, THR = 13), and these participants had a combined average LOS across both CALHN sites of 4.3 days. Notably, this was less than that of non-MPP participants who underwent TKR/THR surgery during the same time period (4.7 days, p = .893) and of all patients who underwent these procedures in the year before MPP implementation (5.3 days, p = .431) (Figure 8). Average LOS for MPP participants (FY 22/23) compared with CALHN sites prior to MPP implementation (FY 21/22) and during implementation (FY 22/23).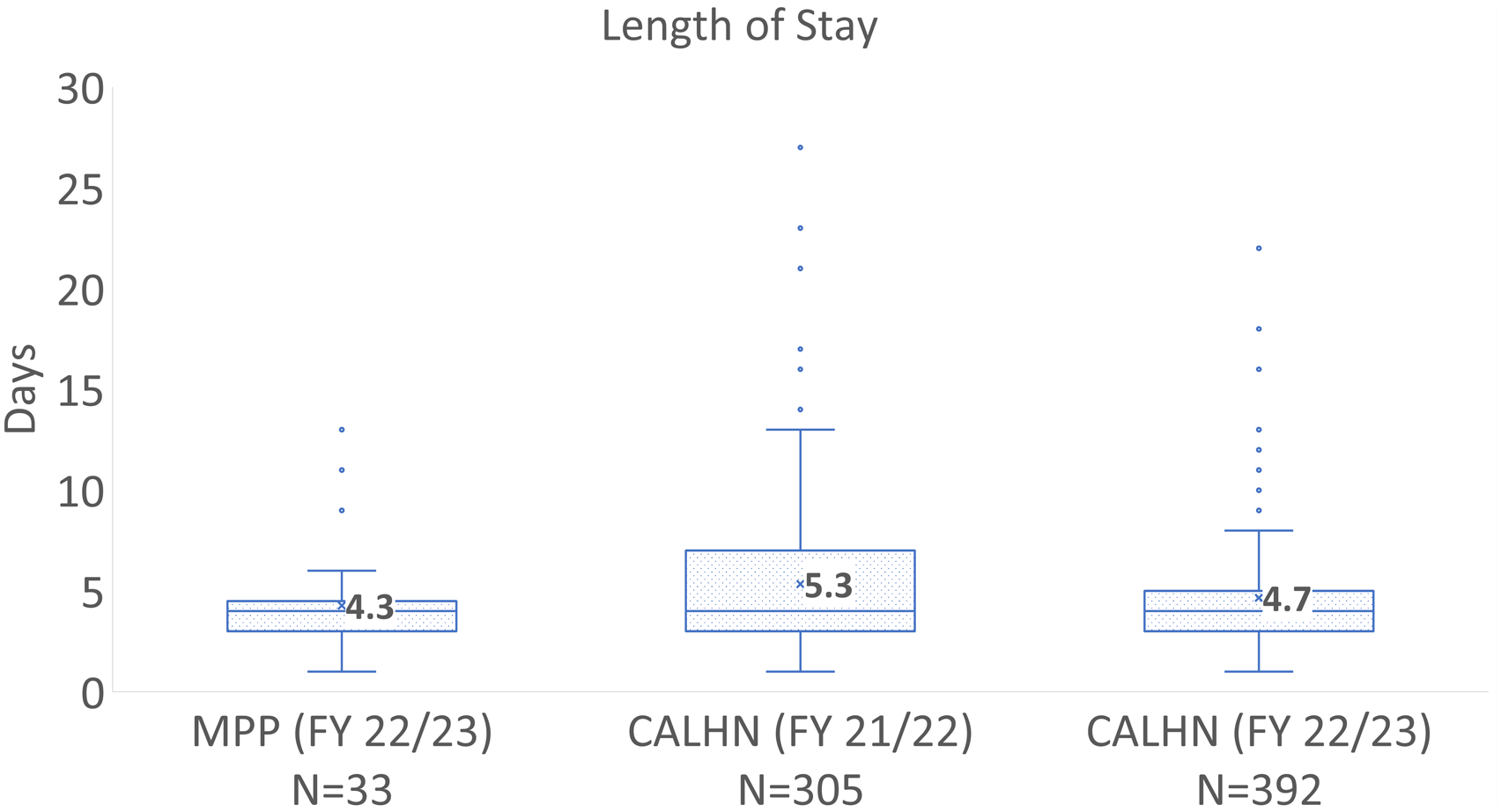
Discussion
This paper presents new insight into the prevalence of modifiable risk factors in individuals at the point of referral for joint replacement surgery and the potential to use a hospital-initiated semi-automated digital prehab pathway (MPP) to help optimise health and well-being during the pre-surgical period. MPP was well adopted by invitees and without active recruitment 79.4% registered. Almost all who registered went on to participate, completing the health screen (HAQ) and engaging in the health content provided. Ongoing running costs are minimal by utilising existing staff and promoting GP support and other community services.
Commonly cited barriers to accessing digital initiatives such as relative socio-economic disadvantage, indigenous status and requiring an interpreter for health appointments were not found to be barriers to participating in MPP. Similarly, the participation rate for regional residents was excellent (88.0%). Unsurprisingly, non-participants tended to be older, however the maximum age for both groups were very similar (participants = 88 vs non-participants = 91) and older participants were observed across nearly all age groups. This suggests that although older adults were statistically less represented in the participant cohort, many older invitees still participated in the digital MPP.
MPP is a holistic digital initiative designed to inform and support individuals to self-direct prehabilitation while awaiting a joint replacement. Early feedback (2-weeks post registration) saw most participants either undecided or agreeable that MPP was acceptable, appropriate and feasible. Despite relatively high levels of neutrality, fidelity to the intended use of the MPP platform was observed, particularly at the beginning of the pathway, and many indicated engagement with desired health behaviours. Interestingly, participants who received a joint replacement in the study period reflected more positively about the acceptability, appropriateness, and feasibility. With preliminary surgical outcomes also suggesting a reduction in the length of stay of up to one day, definitive scores of acceptability, appropriateness and feasibility early in the program may not be required to achieve desired outcomes.
The presence of surgical risk factors in this cohort was high; notably chronic pain (4 in 5, four times the national average), obesity (3 in 5, two times the national average), frailty (2 in 5, two times the national average) and diabetes (1 in 5, four times the national average).35–38 Physical activity levels were also concerningly low, highlighting that individuals with a poor functional baseline were being placed on long waitlists. While this is understandable in a cohort who are waiting for a joint replacement, frail and inactive people waiting for months to years without intervention is likely to have detrimental consequences to quality of life and eventual surgical outcomes. With a median age at referral of 65, increasing age will also contribute to the development of additional risk factors and the surgical complexity of this cohort.
Given the potential for optimisation in the identified risk areas, access to information on relevant evidence-based management options should be offered to all surgical candidates, especially with the ability to do this digitally at large scale and low-cost. With the information provided by MPP having a health promotion focus and epitomising good ‘general health’ advice, the program is also relevant and likely to be beneficial for those who do not proceed with surgery. Having core content available to the public on our companion website (www.calhn-prehab.sa.gov.au) helps to disseminate information more broadly to those without access to the digital pathway. It also acknowledges the pivotal role the GP has in coordinating care by supporting access to relevant evidence-based information and existing community programs.
By providing hospital-initiated guidance at the time of referral patients know what to work on, why it is important, and where they can access support. Additionally, health screening following triage assisted clinicians to identify cases of category 3 obesity (BMI
Although there may be limitations in quantifying patient reported intention or action to optimise health, or if GP assistance was sought, high response rates are promising. With over half of participants reporting that they required ‘no’ or ‘a little’ support to improve their health before surgery, it is possible that interventions that support a self-management approach may be appropriate. However, low confidence levels to achieve this prior to engaging in MPP may also suggest many participants did not believe, or were unaware, that improvements were possible and may hint at the presence of an external locus of control (i.e., surgery is the only solution). It is acknowledged that some people require individual assistance and others may not wish to engage, however, by supporting those who are able and want to ‘self-serve’, there will be positive flow-on effects to others (e.g., shorter hospital admissions improving bed capacity).
Modifiable risk factor and general medical screening were collected via a patient reported questionnaire (HAQ). There consequently may have been over-reporting (e.g., level of functional disability) or under-reporting (e.g., emotional wellbeing) by participants to improve the likelihood of earlier treatment or due to stigma. 39 To reduce response burden, overarching questions were used to determine if subsequent questions were required to elicit further details. Consequently, there may have been an underrepresentation of the true number of some subcategories reported on (e.g., alcohol consumption and mobility aid use).
As this paper is an initial exploration of MPP and given the small number of participants who progressed through to surgery during the study period, a full matched sample analysis or comparison of hospital acquired complications has not yet been undertaken. Similarly, although preliminary length of stay data are positive, the authors acknowledge the preliminary nature of this study as a limitation and plan to examine any possible effect of MPP on LOS in a statistically robust and controlled fashion when more participants complete their surgery. However, this paper highlights the extended time patients experience on waitlists, with only 6.6% having surgery during the reporting period, of which the majority were from the surgical waitlist (n = 20). The overall high adoption of MPP could result in broader societal benefits, including general health optimisation, improved awareness of hospital expectations (for both referring GPs and patients) and surgical avoidance.
Conclusion
This paper highlights the prevalence of modifiable risk factors in individuals referred for joint replacement surgery and opportunities to optimise care and provide choice through a digital prehab program (MPP). MPP demonstrated high adoption, fidelity, and participant engagement. It is acceptable, appropriate and feasible and has the potential to be scaled-up digitally at low-cost. Early indications suggest this preoperative intervention may benefit both patients and the healthcare system.
Supplemental Material
Supplemental Material - Opportunities to optimise care and choice in joint replacement surgery using a digitally delivered, holistic PreHab pathway
Supplemental Material for Opportunities to optimise care and choice in joint replacement surgery using a digitally delivered, holistic PreHab pathway by Eleanor Bills, Anastasia Dimopoulos, Anne L. J. Burke, Kathryn L. Collins, Ecushla Linedale, Vicki Hume, Jackie Yeoh, Sharyn Coles, Mandy Nolan, Kate Southam, Lesley Thomas, Melanie Ramsey, and Jane M. Andrews in Journal of Orthopaedic Surgery.
Footnotes
Acknowledgments
The authors would like to thank the Royal Adelaide Hospital and The Queen Elizabeth Hospital Orthopaedic Departments for their support of this initiative, Health Translation SA for providing expert support and consultancy, and CALHN for its contribution to the digital technology and time of team members. Thank you to Kirri Riley for her ongoing support and involvement in website development.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hospital Research Foundation Group [2021/57-QA25315].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.