
Abstract
Background
The hallux valgus deformity is made up of misaligned first metatarsal, hallux, and sesamoids. Their angular deformities are well-studied, but not their positional displacements. A few available reports claimed the proximal end of the proximal phalanx and sesamoids were not shifted medially along with the first metatarsal head. However, the general observation is otherwise. This study revisits the issue.
Methods
A radiological study of 189 feet with and without the hallux valgus deformity was carried out to analyze the first metatarsal, hallux, and sesamoid positional changes in relation to the second metatarsal and among themselves. A total of 194 X-ray images with all relevant measurements that formed the raw database for this study were submitted for online viewing and reference.
Results
There was a statistically significant change in the first metatarsal, hallux, and sesamoid positions of feet with hallux valgus deformity compared to normal feet. All have migrated medially but to different degrees. It was contrary to the past findings of no change in sesamoid and hallux positions.
Conclusions
We agree with past findings that the metatarsus primus varus deformity is directly related to the failed medial metatarsosesamoid ligament. We also believe in the failure of the deep 1-2 transverse metatarsal ligament responsible for the sesamoid migration.
Introduction
The hallux valgus deformity condition of the foot is a deformity complex comprised of three interrelated skeletal misalignment deformities in the first ray, the metatarsus primus varus (MPV) deformity, hallux valgus (HV) deformity, and metatarsal-sesamoid dissociation (MSD) deformity. MPV has been regarded as the primary deformity of the three.1,2 As the first metatarsal deviates medially, the hallux and sesamoids can be pulled laterally by the lateral head of the flexor hallucis brevis and adductor hallucis muscles3–5 coupled with the failure of their medial stabilizing collateral and metatarsosesamoid ligaments to develop the HV and MSD deformities respectively. 6 MPV is an acquired deformity. The common pathology underlying its development is the incompetent stabilizing ligaments of the first metatarsal.6–8 Several precipitating factors for ligamentous failure have been proposed, such as female gender, 9 heredity, 10 shoes, 11 and degeneration.
Stainsby
7
described a ligamentous tie-bar system that maintains the five metatarsals’ stability by keeping their heads together (Figure 1). He found it was mainly the medial metatarsosesamoid ligament at the medial end of this tie-bar system attenuated and failed. Without the ligamentous constraint, the first metatarsal head may gradually be pushed away from the second metatarsal under the stress of daily activities. Later, Khaw et al
8
found that the deep transverse metatarsal ligament (DTML) portion of the tie-bar system was also an important stabilizer of the first metatarsal and suggested its possible failure in developing MPV deformity. If the 1-2 DTML of MPV feet also failed and stretched, the sesamoids would also migrate medially with the first metatarsal. However, past studies reported that sesamoids did not move in relation to the second metatarsal when HV feet were compared to normal feet.12,13 Hence, the structural integrity of the DTML has not been questioned. Furthermore, postoperative studies have shown that the first metatarsal head was moved closer to the second metatarsal head but not the sesamoids.14–16 This unchanged postoperative sesamoid position may have also suggested a normal DTML that was not elongated or stretched. (a) Cross section of normal foot illustrating the Tie-Bar System. (b) Mild MPV deformity showing greater 1st metatarsal (c’-c) than medial sesamoid (b’-b) displacement. (c) Severe MPV deformity showing greater 1st metatarsal displacement than 1B (c” vs c’), but no change in medial sesamoid position (b” vs b’).
However, the surgeon-author had frequently noticed the different radiological sesamoid-second metatarsal distances between normal and HV feet (Figures 2 and 3). Normal feet showing radiological IMA (Intermetatarsal Angle), MPA (Metatarsophalangeal Angle) and MSP (Medial Sesamoid Position) parameters within their normal ranges and their HMD (Hallux to Second Metatarsal Distance), 12MD (First to Second Metatarsal Distance) and SMD (Sesamoid to Second Metatarsal Distance). All five parameters (MPA, MSP, H2MD, 1-2MD, S2MD) of this patient’s feet correlated well to their IMAs (ESM 1, Case 1632). The different S2MD between feet suggest different lengthening of their 1-2 deep transverse metatarsal ligaments. A = H2MD (Hallux to Second Metatarsal Distance), B = 1-2MD (First to Second Metatarsal Distance), C = S2MD (Medial Sesamoid to Second Metatarsal Distance).

This study was to collect evidence on whether the sesamoids of HV feet are displaced medially or not. If so, the implication is that both the medial metatarsosesamoid and 1-2 DTM ligaments are compromised in HV feet. Then, surgical results may benefit from including proper realignment and re-stabilization of the sesamoids,17,18 in addition to the first metatarsal head.
We also investigated and discussed the possibility of medial displacement of the proximal phalangeal base and the correlation between all three displaced bones.
Materials and methods
This study reviewed and analyzed past X-rays of 97 individuals’ 194 feet. Fifty-five individuals were consecutive HV patients from the surgeon-author’s practice. The other 42 individuals were solicited from the staff of a private hospital. Everyone’s standing AP-view X-ray of both feet was taken on the same platform of a computerized digital podiatric X-ray machine (20/20 Imaging®, Lake in the Hills, IL, USA) with its cathode tilted 30° posteriorly. Hardy’s mid-axial method 19 with a built-in software program (Opal-RAD, Viztek, USA) was used for measuring the first intermetatarsal (IMA) and metatarsophalangeal (MPA) angles. Their medial sesamoid positions (MSP) were assessed with Hardy’s 7-position method. 19
We also measured the distances from the first metatarsal, hallux, and medial sesamoid to the second metatarsal. The distance between the first and the second metatarsals (1-2 MD) was measured from the point where the first metatarsal mid-axial line intersected with the metatarsal head joint line perpendicular to the second metatarsal mid-axil line. The distance between the hallux and second metatarsal (H2MD) was measured from the proximal phalanx mid-axial line intersecting with its proximal joint line perpendicular to the second metatarsal mid-axial line. The medial sesamoid and second metatarsal (S2MD) distance was measured from the medialmost border point of the medial sesamoid perpendicular to the second metatarsal mid-axial line (Figure 2). The distances were determined with the online desktop ruler, https://www.arulerforwindows.com/. It was chosen for its fine unit to produce three-digit measurement numbers to detect small differences for a more sensitive comparison. Five feet from three individuals (Supplemental Material 1, Cases 1631, 1653, and 1661) did not have medial sesamoids and were excluded from this study. The total number of studied individuals was 94, and their 189 feet. The non-patient group had 27 feet with IMA greater than 9°. The HV-patient group had 10 contralateral feet with IMA equal to or less than 9°. Sixty-seven feet with IMA equal to or less than 9° and 127 feet with IMA greater than 9° were studied. We did not consider age, gender, and foot symptoms because we felt the investigation of this study was independent of these variables, and they were irrelevant to the results.
Supplementary material (SM)
We presented 194 X-ray images of the entire cohort showing every individual’s feet with their IMA, MPA, MSP, 1-2MD, H2MD, and S2MD measurements for electronic online viewing and reference in the supplementary material file (Supplemental Material 1). We also presented the working Excel table of the cohort as in Supplemental Material 2, the subgroup IMA ≤9° Excel table as in Supplemental Material 3, the subgroup IMA greater than 9° and equal to or less than 15° Excel table as in Supplemental Material 4, and the subgroup IMA greater than 15° Excel table as in Supplemental Material 5.
Statistical analysis
The data were analyzed using JMP Pro 15.0.0 (SAS Institute). The Pearson correlation coefficient was used to assess the strength of the association between the two measurements. Independent t-tests and one-way ANOVA were used to test for differences in means among separate groups. Multiple comparisons were performed using Tukey-Kramer Honestly Significance Distance.
A paired t test was adopted to compare S2MD and 1-2MD of the same foot. All tests were two-tailed, and a p-value <0.05 was considered statistically significant.
Results
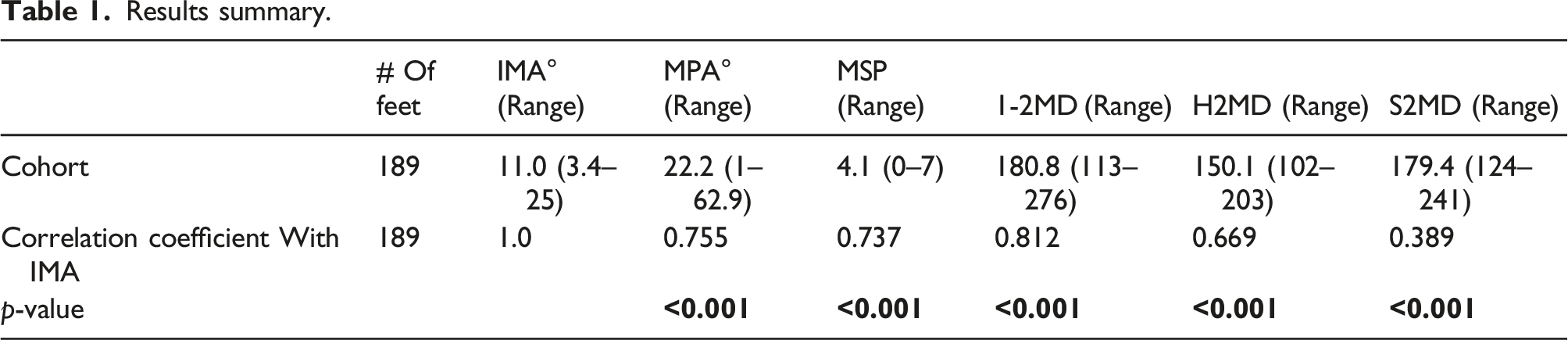
Results summary.
Parameters comparison between mormal and HV feet.

Since the medial sesamoid is located medial to the mid-axial line of the first metatarsal, the S2MD was, as expected, greater than the 1-2MD in normal feet (Table 2). However, despite the medial sesamoid of MPV feet having significantly migrated medially, the fact that the first metatarsal had migrated medially even more than the medial sesamoid had so that their 1-2MD would become greater than S2MD. To confirm the above conjecture, a paired t test was performed (as we should compare S2MD and 1-2MD of the same foot. So define D = S2MD – 1-2MD. For the whole sample, the mean of D is −1.41 (range: −75 to 42). When testing for mean = 0, p = 0.474 indicates that the mean of D is insignificantly different from 0. When performing the paired-t test separately for the two severity groups, it is found that the mean difference in the normal group is 20.28 (range: −14 to 42, p < 0.001) and that in the HV deformity group is −12.77 (range: −75 to 37, p < 0.001) that the two means are significantly different from 0, but in different directions which supports the above conjecture. (Supplemental Material 8)
Parameters comparison between IMA subgroups.

Discussion
MPV deformity has always been regarded as the primary underlying development that initiates a cascade of secondary changes in the development of the HV deformity complex. It invariably consists of the HV and metatarsosesamoid dissociation (MSD) deformities. Furthermore, as the MPV deformity worsens progressively, clawing of lesser toes, collapsing of the metatarsal20,21 and longitudinal22–25 arches, and metatarsalgia26,27 may develop.
While MPV deformity is the common denominator of all acquired hallux valgus deformities, ligamentous failure is the common denominator of acquired MPV deformities. The medial metatarsosesamoid ligament at the medial end of the tie-bar system described by Stainsby 7 for maintaining metatarsal heads together was deemed the primary failure site. As the unprotected first metatarsal head migrates, medially, away from the second metatarsal head, the IMA and gap between them increase (Figure 1(b)).
Our study found that as the 1-2 metatarsal gap distance (1-2MD) increased, the medial sesamoid-second metatarsal (S2MD) and proximal phalanx-second metatarsal (H2MD) distances would also increase, although not as much but still a strong correlation with IMA of the MPV deformity (Table 1). It also confirmed strong IMA-MPA and IMA-MPS correlations, as reported in the past. The differences between normal and HV feet of all their six radiological parameters were also statistically significant (Table 2).
To our best knowledge, this current study demonstrated for the first time in the literature in direct contradiction to the few available past studies that reported the sesamoids12,13 and proximal phalangeal base 28 were not displaced medially in relation to the second metatarsal in the HV deformity. Other than the different assessment methods, the reason for this stark difference is unclear.
The average medial displacement of the medial sesamoid in HV feet compared to its position in normal feet was about 40% (21.9/54.7) of the first metatarsal’s medial displacement. This limited sesamoid displacement is likely due to its connection to the DTML and adductor hallucis muscles. It still implied a structural loosenig of the DTML. The exact nature of any DTML failure will need future histological studies to clarify. There was also a proximal phalangeal base medial shift, about 53% (29.1/54.7) of the first metatarsal. It was greater than the sesamoid’s, possibly due to its attachment to the first but not the second metatarsal head. Its limited displacement was probably also restricted by adductor hallucis muscles. Since neither the sesamoids nor the proximal phalanx shifts medially as much as the first metatarsal head, they would gradually dissociate from it and become laterally subluxated and incongruent.
Past studies reported that osteotomy procedures14–16 could relocate the first metatarsal head closer to the second metatarsal to restore the normal metatarsal-sesamoid relationship, however, without relocating the displaced sesamoids. Since this study has demonstrated that sesamoids of MPV feet are actually displaced medially, it implies that the present surgeries have not been realigning either the first metatarsal or sesamoids to their pre-HV deformity positions in relation to the second metatarsal. Studies have shown the importance of proper metatarsal-sesamoid realignment for mechanical function restoration 17 and deformity recurrence prevention.18,25 Moreover, past pedobarographic studies showed inconsistent mechanical function restoration of the foot after osteotomy procedures.29–32 Future studies may investigate its relation to the incomplete anatomical realignment of the first metatarsal head and sesamoids.
This study also reports, for the first time in literature, that an unexpected phenomenon of severe MPV deformities was not associated with greater sesamoid medial displacement than milder MPV deformities (Table 3). Therefore, while the overall S2MD’s mean of HV feet with IMA >9° was significantly greater than normal feet, the S2MD of more severe MPV feet was no longer correlated to their IMA as the mild-moderate MPV feet (Figure 4). We feel this phenomenon was due to two possible situations. One is a severe failure of the medial metatarsosesamoid ligament that could not stretch DTML anymore to allow further medial displacement of the medial sesamoid. The other is the first metatarsal pronation rotation deformity associated with more severe MPV deformities. The first metatarsal pronation can espouse the same rotation of the lateral sesamoid and negate its further medial traction on the medial sesamoid. Four parameters (MPA, MSP, H2MD and 1-2MD) but not S2MD of this patient’s feet correlated well with their IMAs. Her left foot had greater 1-2MD and IMA but less S2MD (the medial sesamoid medial displacement) than her right foot (ESM 1, Case 1656). This discrepancy was likely the result of a weaker and more elongated medial metatarsosesamoid ligament of the left foot. A = H2MD (Hallux to Second metatarsal Distance), B = 1-2MD (First to Second Metatarsal Distance), C = S2MD (Medial Sesamoid to Second Metatarsal Distance).
This study’s limitations were no reliability study was conducted on its measuring technique for the 1-2MD, H2MD, and S2MD, and a weight-bearing CT scan study was not available to help a 3D understanding of the relationship of the sesamoids to the MT heads displacements of HV feet. This study’s strength was its highly standardized X-ray documentation at a single facility with the same foot-specific imaging equipment and technique for the entire cohort.
Conclusion
This radiological study demonstrated that MPV feet’ first metatarsal heads were significantly displaced medially, as well as medial sesamoid and hallux, although not as much. These findings inferred that not only the medial metatarsosesamoid ligament but also the DTM ligament was stretched and gave way. The medial sesamoid’s medial displacement of more severe MPV deformities was limited, possibly by the first metatarsal pronation rotation.
Supplemental Material
Supplemental Material - Are sesamoids and proximal phalanx of metatarsus primus varus deformity of hallux valgus feet displaced? A radiological study
Supplemental Material for Are sesamoids and proximal phalanx of metatarsus primus varus deformity of hallux valgus feet displaced? A radiological study by Daniel Yiang Wu, and Eddy Kwok Fai Lam in Journal of Orthopaedic Surgery
Footnotes
Author contributions
That all authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and that all authors are in agreement with the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.