
Abstract
Orthopedic surgeries are associated with high-risk of thromboembolism which occurs in 40% to 60% of orthopedic patients in the absence of thromboprophylaxis. Conventionally heparin anticoagulants were used for thromboprophylaxis and currently direct oral anticoagulants (DOACs) are widely used due to their minimal complexity. Anticoagulant use carries bleeding risk and requires optimal laboratory monitoring through conventional thrombin-based assays, anti-Xa assay, anti-IIa assay and contemporary ecarin chromogenic assay (ECA) and rotational thromboelastometry. Monitoring requires multiple hospital visits and hence, the development of point-of-care assays is gaining momentum. Also, a thorough risk assessment model (RAM) is necessary for successful anticoagulant therapy since it enables personalized approach for better thromboprophylaxis outcomes. Despite welcoming changes, lack of guideline consensus, population-based thromboprophylaxis, deficiencies in risk stratification and non-adherence are still a concern. Stronger clinical and process support system with uniform guidelines approaches and patient-specific RAM can aid in the successful implementation of anticoagulant therapy.
Keywords
Introduction
Thromboembolism is a common complication in orthopedic surgical patients during and after hospitalization. Orthopedic surgeries such as joint replacement surgery or spinal surgery increases the risk of venous thromboembolism (VTE), which includes pulmonary embolism (PE) and deep vein thrombosis (DVT). Orthopedic patients have long been recognized as a high-risk population of VTE1,2 and they were primary patient groups studied in VTE prophylaxis trials. The risk of VTE in orthopedic surgery is significantly higher compared to general surgery (38.4% vs 2.1%, p < 0.0001). 3 The incidence of VTE ranges from 10% to 40% in general surgery compared to 40% to 60% in orthopedic surgery. In the absence of prophylaxis, PE is responsible for 5% to 10% of deaths in hospitalized patients and among orthopedic surgeries, PE fatality rate was 2% to 3% after elective hip replacement and 4% to 7% after hip fracture surgery. 4
Anticoagulants remain the mainstay for the prevention and treatment of thromboembolism. Pharmacological VTE prophylaxis in orthopedic surgery patients includes aspirin, unfractionated heparin (UFH), low molecular weight heparin (LMWH), adjusted dose vitamin K antagonists (VKA) and synthetic pentasaccharide factor Xa inhibitor (fondaparinux).1,5 Direct oral anticoagulants (DOACs) such as dabigatran, rivaroxaban, apixaban, and edoxaban have emerged and are increasingly being used in orthopedics. These novel oral anticoagulants are expected to replace conventional agents owing to their ease of use and more favourable pharmacodynamic profiles.5,6 The first trial on anticoagulant thromboprophylaxis was conducted in 1959 and demonstrated a reduction from 10% to 0% in the PE incidence 7 and since then, many clinical trials have been conducted to demonstrate the effectiveness of thromboprophylaxis. When thromboprophylaxis has been used prior to hospital discharge a reduction in the rate of VTE from 4.3% to 0.53% was noticed in patients 35 days following major orthopedic surgery. 8
The choice of anticoagulant depends on several risk factors, including the patient’s characteristics such as age, weight and medical history of VTE, risk of bleeding and the type of surgery performed.4,9 The risk factors and the choice of anticoagulant varies between different patients and hence individualized approaches become increasingly appealing which supports the assessment of an individual’s risk of developing VTE to guide tailored prophylaxis decisions. 2 The aim of this review is to discuss various challenges and opportunities of the current anticoagulant use in orthopedic surgery. This article also focusses on the application of anticoagulant drugs and the risks and benefits that are associated with anticoagulation therapy in orthopedic surgery.
Coagulation and thromboembolism
Thromboembolism has long been recognized as a risk factor for the development of venous thromboembolic complications. It occurs by coagulation process which involves the conversion of soluble fibrinogen to insoluble fibrin. Coagulation includes a cascade of extrinsic and intrinsic pathways intersects by the activation of factor X. In the extrinsic pathway, vascular damage exposes tissue factor which binds with factor VIIa and calcium to promote the conversion of factor X to Xa. In the intrinsic pathway, activation of factor XI leads to the activation of factor IX, which upon acting with factor VIII, forms a complex on a phospholipid surface to activate factor X. Activated factor X along with its cofactor (factor V), tissue phospholipids, platelet phospholipids and calcium converts prothrombin to thrombin which further converts circulating fibrinogen to insoluble fibrin and form platelets.1,10 Anticoagulants used for the treating thromboembolism acts on the coagulation cascade by directly inhibiting the enzymes or indirectly by binding to antithrombin or by preventing its synthesis.
11
Mechanism of anticoagulants are depicted in Figure 1 and characteristics of anticoagulants discussed are shown in Table 1. Mechanism of action of various anticoagulant drugs. Anticoagulant characteristics used in orthopedic surgery.

Anticoagulants in orthopedic surgery
Aspirin
Aspirin (acetylsalicylic acid) is an oldest drug used by humans dating back to 1500 BC but its stable form was purified by Hoffmann in 1897. Aspirin’s therapeutic properties were described in 1899 and was introduced to medical use by 1900. It is a non-steroidal anti-inflammatory drug with a mechanism of action similar to other salicylates. 12 Aspirin suppresses the production of eicosanoids derived from arachidonic acids like prostaglandins and also involves in acetylation of platelet cyclooxygenase that inhibits thromboxane formation.12,13
Though aspirin has a long history used as an anticoagulant and has several advantages like lower bleeding risk, inexpensive, easy to use and wider availability, it is no longer a preference for orthopedic surgeons with the emergence and clinical use of new anticoagulants such as DOACs in recent years. However, 2012 American College of Chest Physicians (ACCP) guidelines and 2018 European guidelines, recommended aspirin for patients undergoing total hip replacement (THR), total knee replacement (TKR) or hip fracture surgery, compared to no pharmacologic prophylaxis.8,14
Unfractionated heparin (UFH)
UFH was the first anticoagulant discovered in 1916 by Jay McLean while studying the putative prothrombotic properties of dog liver and heart extracts. In the early years of its discovery, UFH was used without any real understanding of its mechanism of action.15,16 In 1970s it was discovered that UFH is a blend of polymorphic polysaccharide chains which are responsible for dramatically increasing the activity of antithrombin (AT), a glycoprotein accounting for the most of all naturally occurring anticoagulation. 17
UFH, a heterogeneous combination of glycosaminoglycans, inhibits thrombin, factor Xa, and other clotting enzymes by binding to antithrombin through a specific pentasaccharide sequence. Factors Xa, IXa, XI, and XIIa are inactivated by the heparin/AT complex, together with thrombin (factor IIa). Since heparin cannot be absorbed orally, it must be administered parenterally.1,18 Preferrable parenteral routes of UFH administration include intravenous (IV) infusion or subcutaneous injections. When given as an ongoing IV infusion, UFH has a short half-life of 30 min, while it has a longer half-life of 90 min when given subcutaneously. 19 However, subcutaneous doses need to be large enough (30,000 U/day) to overcome UFHs low bioavailability. 20 After injection, UFH is eliminated from the bloodstream by the saturable process, in which heparin attaches to endothelial cells with a high affinity before being cleared by the reticuloendothelial system and also by non-saturable process that is renal excretion. 21 ACCP guidelines recommend the use of UFH for VTE prophylaxis in patients undergoing THR, TKR or hip fracture surgery. 8
Lower molecular weight heparin (LMWH)
The focus on antithrombotic research was increased worldwide in the 1960s–1970s due to developing awareness of the contribution of thrombosis in diseases such as stroke, myocardial infarction, and VTE. Intense research on coagulation science led to the identification of new compounds and increased understanding of the mechanism of coagulation cascade. This improved understanding, led to the development of a subclass of heparins called LMWHs. These are derived from UFH by chemical splitting and have fewer side effects with a more predictable anticoagulant response. LMWH. such as enoxaparin, has now replaced heparin for most thrombotic indications. 17
Molecular weight of LMWH is approximately one-third of UFH (mean, 4000 to 5000 D; range, 2000 to 9000 D). In thromboprophylaxis settings, LMWH has superior pharmacokinetic properties and is preferred over UFH because of its greater bioavailability, longer half-life of 4 h, quicker absorption with less endothelial and protein binding. The inhibitory activity of LMWH against factor Xa is greater than thrombin and exhibits less binding to cells and proteins than UFH. Use of LMWH is more convenient as it allows for fixed-dose administration subcutaneously and less frequent monitoring since it has been shown to have better association between dosage and anticoagulant response.22,18,19 Hence, they provided an advantage of treating patients with VTE as outpatients, rather than in hospitalized settings. 17
In the last 2 decades, many studies have reported the advantages of LMWH over other anticoagulants in orthopedic surgery. The bleeding complications were reported to be significantly lower and minor with LMWH compared to UFH and warfarin. 23 Even when the doses of UFH and warfarin were adjusted, LMWH still fared better in preventing DVT in TKR patients. 24 In hip fracture surgery, a study has reported LMWH and UFH to be equally effective in preventing DVT 25 while the other study reported LMWH to be more effective compared to VKAs, without any significant difference in bleeding risk in orthopedic surgery patients. 26
Fondaparinux
With scientific advancements, structural chemists were able to fabricate smaller molecules that can antagonize specific clotting factors. These molecules are specific and react with active components of clotting enzymes and precursors which helps in reducing unnecessary off-target effects and drug-drug interactions. Fondaparinux is one such small molecule.
Fondaparinux is a synthetic anticoagulant derived from a pentasaccharide sequence with a molecular weight of 1728D. It functions similarly to that of LMWH and has a specific anti-Xa activity that is higher than that of LMWH (approximately 700 units/mg compared with 100 units/mg for LMWH). Its half-life of 17 h is significantly longer than that of LMWH (4 h). Following subcutaneous administration, fondaparinux is absorbed completely and rapidly and reaches a steady state after the third or fourth once-daily dose. It is excreted unchanged in the urine and in patients with renal impairment its clearance is reduced. Pharmacologically, fondaparinux binds and brings a conformational change at the AT reactive site that enhances its reactivity with factor Xa.18,27 It inhibits factor Xa by binding to AT III with a greater affinity than UFH and LMWH, thereby it is called as an indirect factor Xa inhibitor. 28 A study in a large cohort of >144,000 patients showed a lower incidence of VTE with fondaparinux (1.5%) compared to LMHW enoxaparin (2.3%) and dalteparin (2.1%) and UFH (4.2%). 29 ACCP guidelines recommends VTE prophylaxis using fondaparinux for patients undergoing THR, TKR or hip fracture surgery. However, the guideline also stated that, a close balance between desirable and undesirable effects makes prolonged use of fondaparinux less appreciable, especially compared to LMWH. 8 Though fondaparinux is more expensive than UFH and LMWH, it has advantages like predictable pharmacokinetics that decreases the likelihood of dose adjustments and intensive monitoring. 17
Vitamin K antagonists (VKAs)
VKAs is a group of oral anticoagulants produces its effect by inhibiting vitamin K epoxy reductase, which is required for the conversion of vitamin K to its active form vitamin KH2. Vitamin K dependent proteins such as clotting factors II, VII, IX, and X require c-carboxylation by vitamin KH2 for biological activity. VKAs were invented in 1930 by biochemist Karl Paul Link while investigating the mysterious deaths of cattle in the farm surrounding his laboratory at the University of Wisconsin. Only by 1939, it was found that the dicumarol, a VKA, extracted from spoiled hay was the reason for the cattle deaths because of hemorrhages. Dicumarol competes with vitamin K epoxide reductase and results in anticoagulation. In contrast to other anticoagulants, VKAs are suitable for oral administration. 17
Two common VKA drugs are acenocoumarol (mean half-life, 9 h; range, 8 to 11 h) and warfarin (mean half-life, up to 2.5 days). 30 After its discovery in 1960s, warfarin later become the reference treatment for thromboembolic events. 17 The relationship between the dose of warfarin and the response varies between patients. Also, genetic and environmental factors (dietary intake, drug interactions, critical illness, etc.) might influence the absorption of warfarin, its pharmacokinetic and pharmacodynamic properties. 5 The latest ACCP guideline endorse the use of VKAs in patients undergoing orthopedic surgeries such as THR, TKR or hip fracture surgery. 8
Non-vitamin K antagonist novel oral anticoagulants (NOACs) - direct oral anticoagulants (DOAs)
Major changes in anticoagulation practices have evolved in the past decade and led to the development of non-vitamin K antagonist novel oral anticoagulants (NOACs) or DOACs which can overcome the drawbacks of conventional anticoagulants such as warfarin whose applicability is limited by unpredictable dose response, various food and drug interactions, and requirements for frequent monitoring. 31 Though VKAs have operational advantages in thromboprophylaxis, their anticoagulant effect can be delayed for days. To avoid VTE risk during the delay, heparin is administered to patients for the first five to 7 days. This substantially increases the risk of bleeding due to the presence of dual anticoagulants. DOACs were developed and introduced during the 2010s to overcome the issues pertaining to these clinical complexities. These can be administered orally and have rapid mode of action. DOACs bind to the catalytic site of either FXa or thrombin and inhibit their capacity to cleave and activate their substrates which allows for a wider therapeutic window, enables convenient monitoring, and has a lower risk of drug-drug interaction. 17 Currently USA FDA and EU regulatory agencies have approved four DOACs that include rivaroxaban, apixaban and edoxaban which are factor Xa inhibitors, and dabigatran, which is a direct thrombin inhibitor (DTI). Of these DOACs, guidelines do not recommend the use of edoxaban for preventing thromboembolism in orthopedic surgeries.1,27
Rivaroxaban
Rivaroxaban is an orally administered direct inhibitor of factor Xa. In 2008, rivaroxaban received marketing authorization in 2008 for VTE thromboprophylaxis in adult patients undergoing elective THR or TKR surgery. 32 Phase III clinical trials showed rivaroxaban to be more effective than LMWH enoxaparin in preventing VTE after THR or TKR.33–36 The latest ACCP guidelines recommend rivaroxaban for prevention of VTE in patients undergoing THR and TKR but not for hip fracture surgery. 8
Apixaban
Apixaban is another direct factor Xa inhibitor that has been approved for VTE prophylaxis following THR and TKR surgeries, for acute DVT or PE treatment, and for risk reduction for recurrent DVT and PE after initial diagnosis and treatment. 37 Studies performed confirmed the efficacy apixaban compared to enoxaparin, which led to the approval of apixaban for VTE prophylaxis.38–40 The latest ACCP guidelines recommend apixaban also as a method of VTE prophylaxis in patients undergoing THR or TKR but not for hip fracture surgery. 8
Dabigatran
Dabigatran etexilate mesylate is an orally absorbable prodrug and a DTI. Following oral administration, dabigatran etexilate is converted into the active anticoagulant, dabigatran through non-specific plasma and hepatic esterases hydrolysis. Phase III clinical studies evaluated the use of dabigatran etexilate with enoxaparin and found it to be efficacious for VTE prophylaxis after elective THR and TKR, for the treatment of VTE, and for the prevention of stroke or systemic embolism in nonvalvular atrial fibrillation.41,42 The drug has been approved in many countries for VTE prophylaxis in patients undergoing THR or TKR. 30 Similar to other newer DOACs, ACCP guidelines recommend dabigatran as a method of VTE prophylaxis in patients undergoing THR or TKR but not for hip fracture surgery. 8
Risk identification in thromboembolic orthopedic patients
Orthopedic surgeries such as joint replacement, spine surgery, etc., carry a high risk of post-operative thromboembolism which can be prevented by prophylactic anticoagulant therapy. On the contrary, anticoagulant therapy can also increase the risk of bleeding during and after surgery. Hence assessing the risk factors in orthopedic patients before VTE prophylaxis is mandatory.
Individual VTE risk factors
Individual risk factors of VTE include previous VTE, high BMI, cardiovascular disease and older age, malignancy, hematological disorders, chronic renal failure, prolonged immobilisation, varicose veins, early ambulation within 48 h after surgery and Charlson comorbidity index ≥3.2,43,44 Among the risk factors age, previous history, major orthopedic surgery were studied as high-risk VTE factors in orthopedic patients. A recent Japanese study concluded age >68 years (adjusted odds ratio: 1.06, 95% confidence interval [CI]: 1.03–1.09; p < 0.001) as a high-risk factor for VTE in orthopedic patients undergoing lower limb surgery. 45 Multiple Environmental and Genetic Assessment of Risk Factors for Venous Thrombosis (MEGA) study prominently highlighted previous history of VTE in orthopedic patients as a major risk factor of VTE and emphasized importance of collecting VTE history as part of the preadmission inquiry. Recurrent VTE after major orthopedic surgery was also identified as a highest-risk factor (hazard ratio [HR], 4.0; 95% CI: 1.3–12.4 for recurrence at 1 month), with a cumulative incidence of recurrent VTE of 2% at 1 month, 3% at 3 months, 5% at 6 months, and 10.5% at 1 year 46 A major drawback in assessing the VTE based on individual risk factors is the lack of uniformity. Few studies have even identified smoking as one of the risk factors of VTE.47,48 Hence a combination approach involving multiple risk factors could be of more advantage for efficient and adequate thromboprophylaxis.
Combination risk factors of VTE
List of variables in various risk assessment tools.
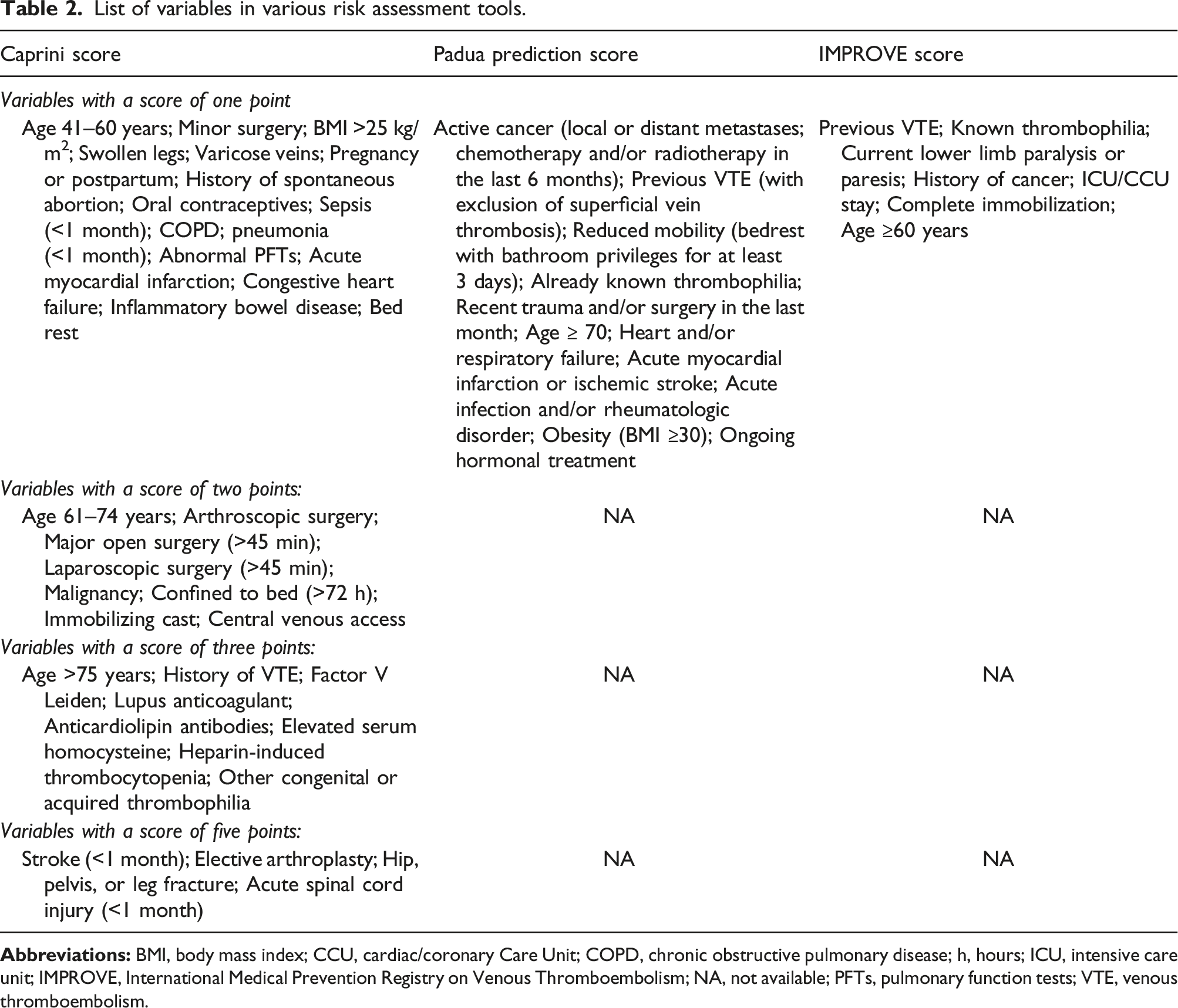
The assessment of VTE risk becomes crucial when the number of risk factors increases in the RAM tool used. A Japanese study evaluated the point-scoring, system-based, computerized clinical decision support system (CCDSS) for assessing VTE risk factors. A total risk score was generated based on the relative scores for individual risk factors that identified VTE risk level of the patients. Though CCDSS provides appropriate recommendations for VTE prophylaxis, few patients who underwent lower limb orthopedic surgery still developed VTE. 45 Evaluation of bleeding risk is as important as evaluating other risk factors but no RAMs have been validated until now for evaluating the bleeding risk in orthopedic patients. 2 The ACCP 2012 guidelines suggest assessing previous major bleeding, severe renal failure, concomitant use of antiplatelet agents, and surgical factors, such as history of difficult-to-control surgical bleeding for evaluating bleeding risk during the current operative procedure, extensive surgical dissection, and revision surgery. 53 Individualized approach on VTE risk prediction might inform better thromboprophylaxis in orthopedic surgery but it is yet to be implemented in the clinical practice due to the absence of standardized guidelines. With the availability of current VTE risk prediction tools and a battery of anticoagulants, better risk assessment and monitoring of anticoagulant therapy could be implemented uniformly in the future, for a tailored VTE risk management approach.
Monitoring of anticoagulation therapy
Anticoagulation carries the risk of bleeding complication which at times can be life threatening. Therefore, adequate monitoring of anticoagulation therapy is necessary to ensure effective medication, preventing blood clots and to prevent bleeding complications following orthopedic surgeries. Several laboratory tests are used for monitoring the anticoagulant therapy which varies with the type of anticoagulant used.
Prothrombin time (PT)
PT is the widely used laboratory methodology for monitoring anticoagulant therapy. In the 1980s, World Health Organization (WHO) developed a standardized ratio called International normalized ratio (INR) specifically for VKA monitoring, to avoid variations when testing PT between laboratories. 54 INR is derived from prothrombin time (PT) which is calculated as a ratio of the patient’s PT to a control PT standardized for the potency of the thromboplastin reagent. 55 INR was developed to eliminate the variation in tissue factor (TF) activity amongst PT reagents and enable the expression of PT data using a common scale. INR is developed from the International Sensitivity Index (ISI), which measures the individual PT reagents and analyzers’ reactivity. In addition, each testing laboratory might have its own geometric mean PT (MNPT), which is the average PT calculated from a least 20 normal donors of both sexes, tested on the same local analyzer and under the same testing conditions as the patient PT. The formula for INR is, INR = (patient’s PT/MNPT)ISI.54,56 To calculate the therapeutic target and properly assess INR after initiation of VKA therapy, the baseline PT, activated partial thromboplastin times (aPTT), and INR values are required. The patient’s liver function also should be assessed to identify potential issues related to VKA metabolism. 27
An INR of 2.0–3.0 is the therapeutic index for VKA and the dosage of anticoagulant required to achieve this range varies based on the patient treated. Genetic and environmental factors such as diet and nutritional intake, drug interactions, illness and injury might influence the INR and based on the variations, the dosage of VKA can be altered during treatment. 5 Monitoring PT using INR is usually recommended at VKA therapy initiation. It is suggested to perform once daily in hospitalized patients, and 1-3 times/week in outpatient settings until the dosage of VKA is properly adjusted. Frequent monitoring should be practiced in patients for whom achieving the therapeutic of INR is difficult. Once stabilized, monitoring frequency can be gradually reduced to intervals between every two to 4 weeks. 27 The INR system is not suitable for monitoring other anticoagulants except VKA therapy, since INR calculation is corrected for reagent sensitivity toward several coagulation factors. Hence when INR was used for anticoagulants that target only one coagulation, it might result in errors. Also, PT cannot be used for DTIs, since they will prolong the PT which is not suitable for the assessment of the drug concentrations. 56
Activated partial thromboplastin time (aPTT)
aPTT is a simple, reproducible, cost-effective test which is the gold standard choice for monitoring UFH. It is typically used frequently that is, within 2 h of initiation of continuous IV infusion, and every 6 h thereafter. The therapeutic range is approximately 1.5–2.5 times the patient’s baseline aPTT. Once the target range is attained and maintained, the UFH dosage may then be altered in relation to the aPTT, and the frequency of monitoring can be reduced. The test can be fully automated and helps in obtaining a relatively linear association between the therapeutic concentration of UFH (0.2–0.4 IU/mL anti–IIa or 0.3–0.7 IU/mL anti–Xa activity) and aPTT.27,56 aPTT reflects the activity of coagulation factors of the intrinsic and common pathway (XII, XI, IX, X, VIII, II and I). In this test, plasma is incubated with a contact activator, such as silica or ellagic acid, and phospholipids. Coagulation is triggered with calcium and time to clot formation is recorded. Monitoring of aPTT is challenging and unreliable due to several complicating factors. 57 For example, baseline aPTT could be prolonged due to confounding factors such as coagulation factor deficiency, high-molecular weight kininogen or prekallikrein deficiency, presence of coagulation factor inhibitors (including lupus anticoagulants), liver disorders, von Willebrand disease and in the presence of interferences such as lupus anticoagulant.58,59 It should be noted that there is a wider variability in the sensitivity of aPTT reagents, and hence it is advisable that individual laboratories should devise their own therapeutic aPTT ranges for safe and reliable heparin monitoring. 60
NOACs have different mode of action than VKAs and UFH and therefore conventional coagulation tests should not be used to monitor their anticoagulant effect. APTT is sensitive to rivaroxaban but the sensitivity is reagent-dependent and correlates with aPTT in a non-linear manner. Though apixaban has less effect on aPTT, its concentration also correlates non-linearly with aPTT. Hence aPTT cannot be reliably used for these anticoagulant drugs. 56 Dabigatran causes steep aPTT prolongation at low concentrations and reaches a plateau at the expected maximal blood dabigatran concentrations. Despite the fact, dabigatran monitoring can be performed using aPTT during emergency situations but aPTT may not reflect supratherapeutic dabigatran levels. Hence, it is advised that each laboratory should be aware of the sensitivity of their aPTT assays to dabigatran using commercially available dabigatran plasma calibrators. 58
Anti-Xa assay
Anti-Xa is the gold standard for monitoring LMWH therapy and also a reference method for measuring UFH concentration which is performed using spectrometry. Anti-Xa is not routinely used for monitoring UFH and is used especially in situations when heparin resistance or the interfering factors such as intrinsic factor deficiency and presence of lupus anticoagulant since using aPTT during heparin resistance and other aforementioned conditions might lead to UFH overdosing. 56
Due to fixed-dose administration, longer half-life, and improved bioavailability of LMWH, it does not require frequent monitoring compared to UFH. Also, plasma anti-Xa levels were consistently found to be correlating with anticoagulant effect and risk of bleeding and weight-adjusted LMWH dosing has proven to be safe and effective, necessitating minimal monitoring.56,61 After subcutaneous injection of LMWH, it reaches maximal blood concentration in 4 h when given twice daily and in 5–6 h when given once daily. The therapeutic range for the twice-daily application is between 0.5 and 1.0 IU/mL, and for the once-daily application, it is between 1.0 and 2.0 IU/mL. Regarding fondaparinux, anti-Xa is the only available methodology. The therapeutic range for fondaparinux is not known and it is suggested to calibrate the test with a known concentration of fondaparinux before testing patient samples.62,63 Monitoring of NOACs such as rivaroxaban can also be performed by anti-Xa assay by calibrating the assay with a rivaroxaban calibrator. The test principle is similar to indirect factor Xa inhibitors, but rivaroxaban requires no antithrombin for estimation. 56 A study reported that the addition of antithrombin results in the overestimation of rivaroxaban levels 64 but in contrast, another study reported that overestimation might be related to other factors and not due to the antithrombin factor. 65 Similar to rivaroxaban, anti-Xa assay can be calibrated and used for measuring apixaban concentration. The principle is similar to that of rivaroxaban and apixaban also does not require antithrombin for its action. The results are expressed in mass concentration (ng/mL or μg/L). In patients treated with apixaban (2.5–5 mg twice daily) with plasma concentration ranging between 40 and 120 ng/mL. 66
Thrombin time (TT) and modified thrombin time
Thrombin time (TT) measures the time taken for the conversion of fibrinogen to fibrin clot by thrombin. Time to clot formation is noted by adding a standard concentration of thrombin to citrated plasma. UFH uses considerable elongation of thrombin time hence TT is not routinely used for UFH monitoring rather it is used for qualitative evaluation and in a situation where heparin contamination in the blood is noted. DTIs such as bivalirudin, argatroban and dabigatran also prolongs TT considerably. Therefore, TT cannot be used for monitoring therapy with DTIs. 56
Modified thrombin time or diluted thrombin time (dTT) is mainly used for the determining plasma concentration of dabigatran. This test follows the same principle as that of conventional TT but a diluted plasma is used. 67 Concentrations of other direct thrombin inhibitors, such as bivalirudin and argatroban can also be assessed by dTT with the use of specific calibrators with known respective drug concentrations. 56
Anti-IIa assay
Anti-IIa assay is performed by adding thrombin to citrated plasma along with a specific chromogenic substrate. The spectrophotometer measures the chromophore that is released by the interaction between the substrate and the thrombin that is not inhibited by the thrombin inhibitor. Since anti-Xa and aPTT is the most widely used test for UFH monitoring, usage of anti-IIa assay is very rare. But the test has been revived recently due to the arrival of DTIs such as dabigatran, however, not much data is available supporting its usefulness in routine clinical practice. 56
Ecarin chromogenic assay
Ecarin chromogenic assay (ECA) was developed for the determination of DTIs. A purified metalloprotease, ecarin is used in the assay, was isolated from the venom of the saw-scaled viper Echis carinatus. Prothrombin is activated by eacrin via a different mechanism that results in the creation of meizothrombin, which resembles prothrombin but has an active site which difficult to access by natural substrates. Hence, meizothrombin’s procoagulant activity is only around 10% of the equimolar thrombin mass. 68 Similar to the principle of anti-IIa assay, excess prothrombin was measured using spectrophotometry where the increase in absorbance is inversely proportional to the concentration of prothrombin. ECA assay is mainly used to evaluate dabigatran concentration but with the use of specific calibrators other thrombin inhibitors can also be evaluated. 69
Rotational thromboelastometry
Rotational thromboelastometry (ROTEM) is based on thromboelastography that involves monitoring the viscoelastic properties of clot formation and its dissolution and provides analysis in a point-of-care manner. Since the analysis can be performed in a point-of-care manner and provides insights on clot stability, ROTEM is considered to be superior to other coagulation tests such as PT and aPTT.70,71 In the ROTEM assay, a small amount of citrated blood is added to a cuvette containing a rotating pin. As the pin rotates, the blood forms a clot around it and the resistance to rotation produced by the viscoelastic changes associated with fibrin clot formation is captured using an optical. This is used for identifying several parameters such as clotting time (CT), clot formation time (CFT), speed of clot formation, amplitude 10 min after CT (A10), maximum clot firmness (MCF), fibrinogen contribution, lysis index 30 min after CT (LI30) and maximum lysis (ML). UFH and LMWHs are monitored using ROTEM but data on direct oral anticoagulants remain scarce. 56
Optimal anticoagulant use
Anticoagulants are “high alert medications” and if not monitored or managed properly results in adverse events in both inpatient and outpatient healthcare settings. 72 Optimal anticoagulant management in the era of DOACs continue to highlight provider expertise, patient difficulties with adherence, imparting anticoagulant knowledge to patients, adequate communication amongst the healthcare providers and respective patients, and role of healthcare system in supporting communications and monitoring. 73
Since there is a strong increase in the number of patients taking anticoagulant therapy and attending the clinic for anticoagulant management, web management through telemedicine has gained attention besides anticoagulant clinics, patient counselling. 74 Telemedicine applied to anticoagulated patients offers several advantages such as increased accessibility to higher volume of patients, integration among different specialists and health structures, immediate data collection and patient’s clinical history update, and the possibility of managing the patients under different anticoagulant drugs. The possibility to shift patient populations into other healthcare locales, whose medical services could otherwise go underutilized, is provided by a decentralized approach via telemedicine technology. Hence, the implementation of telemedicine systems can help in efficient anticoagulation management and reduces the cost burden of patients in anticoagulation treatment.
Timing and duration of anticoagulant therapy
As per the American Society of Regional Anesthesia (ASRA) 2018 guidelines and American College of Surgeons 2018 guidelines, timing of anticoagulant changes with its type. During the preoperative period, warfarin should be discontinued 5 days before the surgery and depending on the renal function, subcutaneous LMWH or UFH should be initiated. If the INR is > 1.5, VKA can be provided at a dose of 1 to 2 mg. LMWH and UFH should be discontinued before 24 h and 4 to 6 h, respectively. During the postoperative period, warfarin can be reinitiated after 12 to 24 h if the patients show no surgical issues that would increase the bleeding risk. LMWH or UFH can be reinitiated after 24 h in case of minor surgeries or after 48 to 72 h in case of major surgeries after assessing the bleeding risk. 75 Depending on the type of surgery, anticoagulation usually lasts 10-14 days (non-joint replacement) or 35 days(joint replacement) after surgery.
Challenges of thromboprophylaxis in orthopedic surgery
While anticoagulation therapy has been shown to be effective in thromboprophylaxis in orthopedic surgery, it is also associated with several challenges. After orthopedic surgery, VTE and the accompanying morbidity and mortality remain an issue, despite the availability advanced thromboprophylaxis.
The usage of anticoagulants to prevent VTE were based on many evidence-based guidelines among which ACCP (ninth edition) published in 2012 53 and the American Association of Orthopedic Surgeons (AAOS) published in 2012 offers substantial insights into the risk of VTE as well as appropriate prophylaxis measures in orthopedic patients. 74 But these widely used guidelines primarily focused on using a population-based approach rather than an individual approach. The population approach is based on the idea that, in the case of major orthopaedic surgery, the contribution of procedure-attributed risk outweighs the patient-specific risk factors, and that, as a result, the choice of prophylaxis is made based on the major surgery itself. Population-based approach simplifies the clinical practice and facilitates easy implementation. However, “one size does not fit all’ and it is ideal that the treating physician should use validated RAMs specific to patients undergoing orthopedic surgery, similar to risk stratification and RAMs recommended by various national and international guidelines for use in hospitalized medical and non-orthopedic surgical patients. To guide thromboprophylaxis, taking into consideration the individual risk factors for VTE and bleeding along with surgery itself should be highly welcoming.76,77
Majority of patients undergoing orthopedic surgery are given thromboprophylaxis but still there is a significant proportion of patients were affected by thromboembolism which is due to inadequate usage of anticoagulants. A study from UK showed that 55% of surgeons used LMWHs, but 30% used acetylsalicylic acid (ASA) only, and a minor proportion of surgeons used mechanical prophylaxis following orthopedic surgery. In patient requiring emergency orthopedic surgery, decision to initiate can be challenging because of the potential requirement for spinal or epidural anaesthesia and high chances of bleeding during the surgery. In these scenarios, there reported an under-utilization of thromboprophylaxis and initiation of anticoagulation therapy can be delayed for days. Although ACCP guidelines have clearly indicated the appropriate thromboprophylaxis measures, these challenges compromise the effectiveness of thromboprophylaxis in orthopedic patients. 78
Though there is a vast development in the past decade in terms of the guidelines on thromboprophylaxis by the AAOS and the ACCP, still a lack of consensus exists on the preferred thromboprophylaxis or an optimal regimen.79,80 Also, it is difficult to establish the balance between the anticoagulant and bleeding complications. 81 Surgeons have cited bleeding as a prominent reason for not prescribing anticoagulants for at-risk surgical patients and for patients completing hospitalization following surgery. 78
Nonadherence to anticoagulant therapy is associated with increased hospitalizations and emergency visits. 82 The Pharmacy Quality Alliance endorsed DOAC adherence as a potential quality measure for managed care plans in 2015. 83 Though higher adherence to DOACs were reported in the randomized controlled trials real-word evidence show that the rate of adherence were sub-optimal. 84 It can further lead to anticoagulation treatment related complexities which should be avoided by engaging patient with optimal resources to improve adherence.
Conclusion
Patients undergoing complex orthopedic surgeries are at high-risk of thromboembolism both during and after hospitalization and requires adequate VTE thromboprophylaxis. Earlier, with the availability of conventional anticoagulants such as heparin and with the absence of evidence-based guidelines, anticoagulant treatment management is challenging. But it has become manageable with the advent of oral anticoagulants and DOACs in the last two decades. Even with recent advancements, research on thromboprophylaxis in orthopedic surgery still shows several gaps in terms of risk assessment, monitoring and adherence of anticoagulant therapy. To overcome this, key strategies should be formulated and implemented based on international and national guidelines. Moreover, individual risk assessment strategies should be developed based on individual patient characteristics which could make the assessment models more robust and highly effective. Focus on involvement of clinical decision-support tools such as point-of-care testing devices, rapid laboratory assays and monitoring charts should be welcoming. Further, process support systems such as telemedicine to support implementation and monitoring of prophylaxis and feedback should be developed in orthopedic surgery settings. These factors can help to improve adherence to guidelines and individual patient requirements which can make the clinical management of high-risk orthopedic patients less challenging.
Footnotes
Acknowledgments
The authors acknowledge Swathirajan CR, PhD and Ramandeep Singh, PhD of Indegene Pvt. Ltd for providing medical writing and editorial services.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Y.W., and X.X. The first draft of the manuscript was written by Y.W. which was supervised and reviewed by W.Z. All authors commented on previous versions of the manuscript, and read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.