
Abstract
Background
The effect of the thumb test for assessing the cancellous bone quality at the resection plane of the proximal humerus on determining the application of a stemless shoulder prosthesis remains unclear. This study was conducted to survey the current utilization of the thumb test among surgeons and to investigate biomechanical features of the thumb test.
Method
A survey among shoulder surgeons who had experience with stemless prostheses was conducted to investigate the current utilization of preoperative assessments and intraoperative thumb test when applying stemless prosthesis. Biomechanical experiments for the thumb test using artificial bone models were performed to assess the compression force, contact pressure and area. According to the preliminary survey, three compression techniques were assessed: compression perpendicular to the surface with thumb pad (P-pad technique) or tip of the thumb (P-tip technique), or compression in the vertical direction simulating compression along the longitudinal axis of the humeral shaft with tip-pad of the thumb (H-axis technique). The contact area was separated into three subregions (proximal, middle and distal) to assess the distribution of contact pressure.
Results
Among 38 surgeons, 66% utilized the thumb test intraoperatively. The P-pad technique was more frequently applied than the P-tip or H-axis techniques (80%, 4% and 16%, respectively). Although with wide variation among the examiners, biomechanical assessments revealed the P-pad technique showed larger contact area and less compression force than the P-tip technique. The P-pad technique provided no significant localized differences in the mean contact pressure on the compressed plane, whereas the P-tip and H-axis techniques showed significant differences among subregions.
Conclusion
This survey demonstrated relatively frequent application of the thumb test on applying the stemless shoulder prosthesis. Biomechanical assessment revealed the thumb test can hinder objective reproducibility among examiners; therefore, further investigations to identify feasible assessments of the bone quality is required.
Introduction
Anatomical total shoulder arthroplasty (aTSA) has been recognized as a favorable surgical option for achieving pain relief and facilitating functional recovery in patients who have recalcitrant glenohumeral arthritis with intact rotator cuff tendons. However, despite the satisfactory outcomes of aTSA, stem-related complications, including periprosthetic fracture following metaphyseal resorption due to stress shielding or implant-diaphyseal mismatch, stem loosening with the osteolysis or relatively large bone loss that may result in difficulty performing revision surgery have been reported.1–3 As an advanced concept to prevent these complications, stemless humeral implants have recently received focus for their ability to prevent meta-diaphyseal bone loss of the humerus. 4 Several studies have reported additional benefits of stemless aTSA, such as a shortened surgical time, decreased intraoperative blood loss and easy application with negligible influences on morphologic alteration, especially for patients with severe proximal humeral deformity.5,6
However, there are some concerns regarding the surgical indication of stemless aTSA. For example, to determine the application of stemless prosthesis, surgeons must carefully assess the bone quality at the humeral metaphysis where the stemless prosthesis is embedded. However, there are no objective tests available to determine the bone quality for a stemless prosthesis. 7 To this end, preoperative assessments using plain radiographs, computed tomography (CT) or bone density scan (BDS) and/or intraoperative confirmation of the bony condition at the resection plane have been attempted when performing stemless aTSA.8,9
The thumb test is commonly used as a simple technique to intraoperatively assess the cancellous bone quality at the resection plane of the proximal humerus.7,10 As Churchill et al. 10 first described, surgeons can predict the cancellous bone quality by compressing the resection plane of the proximal humerus with the thumb; if subsidence is absent at the compressed surface, it may be considered acceptable to apply a stemless prosthesis. 11 However, the feasibility of the thumb test remains unclear due to the lack of a detailed analysis of compression techniques. In particular, there have been no studies assessing the biomechanical properties in the thumb test that would be essential to evaluate in order to clarify the usefulness of the thumb test. Consequently, some surgeons doubt the utility of the thumb test for assessing the application of stemless prosthesis.
Therefore, we investigated the current utilization of preoperative assessments or the intraoperative thumb test to determine the bone quality for stemless shoulder prostheses based on a survey collected from shoulder arthroplasty surgeons in Japan. In addition, we conducted an in vitro experiment to investigate the biomechanical properties of a plane compressed with the thumb that simulated the conditions of the thumb test. In particular, we compared various compression techniques to clarify the most favorable technique for the thumb test that provided consistent stress distribution at the compressed site. We hypothesized that intraoperative thumb test as well as preoperative radiologic assessment might be frequently used to determine the surgical indication of stemless shoulder prosthesis; whereas, biomechanical properties corresponding to the thumb test might represent wide variation among the examiners.
Materials and methods
Survey for the clinical application of the thumb test
A questionnaire regarding pre- and intraoperative assessment for the bone quality.

Note. BDS; bone density scan.
Compression techniques for the thumb test
After the review of the preliminary survey, compression techniques for the thumb test were classified into three groups: compression perpendicular to the surface with the thumb pad (P-pad technique) or with the tip of the thumb (P-tip technique) or compression in the vertical direction that simulated compression along the longitudinal axis of the humeral shaft (humeral axis) with the tip-pad of the thumb (H-axis technique, Figure 1). Compression techniques for the thumb test.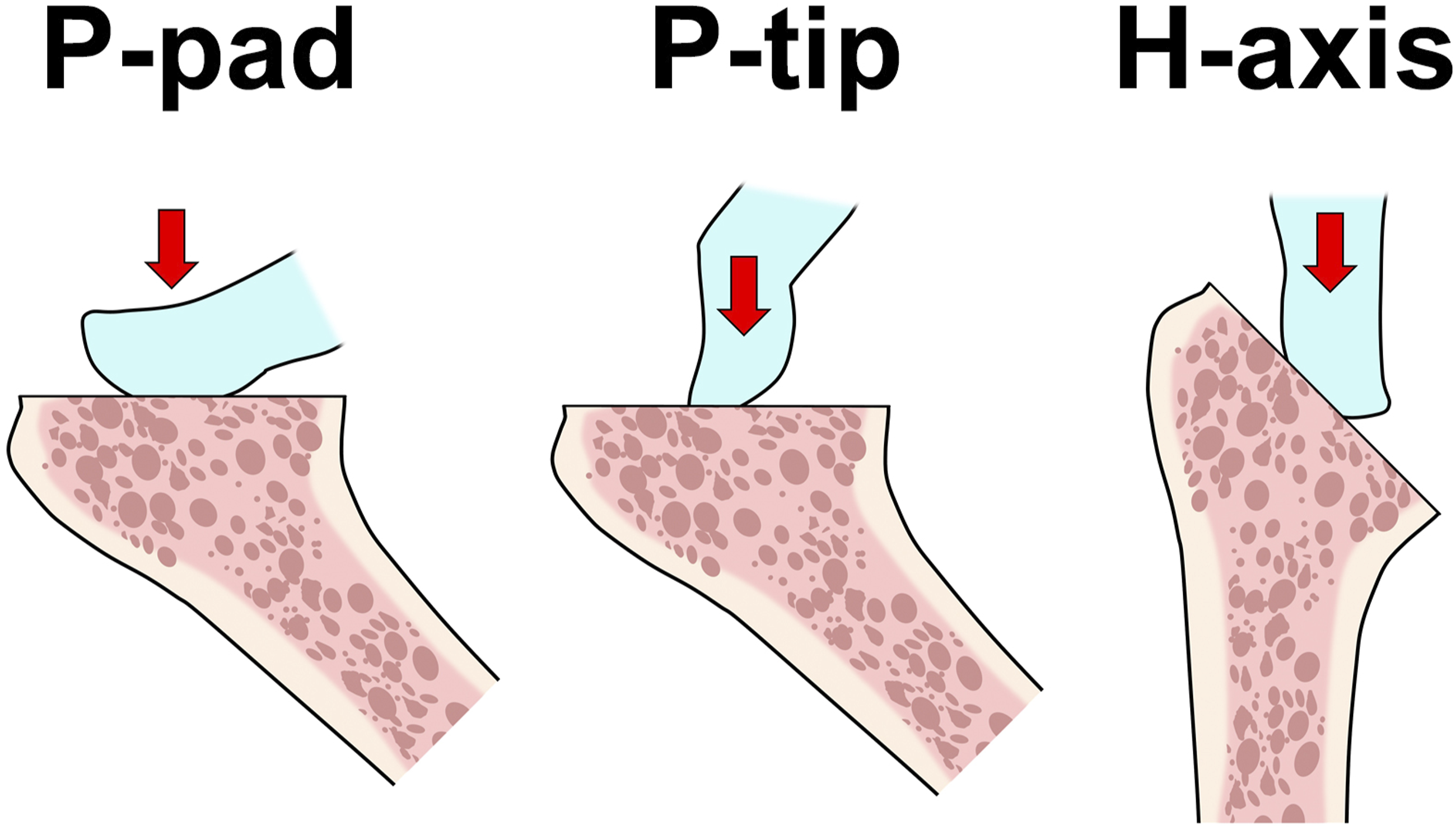
Biomechanical assessments for the thumb test
For the current biomechanical assessment, 3 synthetic cancellous bone models comprising solid rigid polyurethane foam of 0.16 g/cm3 (10 PCF-solid model: 1522-01; Sawbones, Pacific Research Laboratories, Vashon, WA, USA) and 0.24 g/cm3 (15 PCF-solid model: 1522-02; Sawbones) and cellular rigid polyurethane foam of 0.24 g/cm3 (15 PCF-cellular model: 1522-1300; Sawbones) were used. According to the literature conducting biomechanical testing, the bone models of 0.16 and 0.24 g/cm3 can be used to simulate the greater tuberosities of the normal human humerus.12,13 Each bone block was cut to 43 mm in width, 40 mm in depth and 90 mm in height and then fixed in a specific device that enabled stabilizing the bone with a tilt of 45° (Figure 2). The tilt angle was determined as the cutting angle of the humeral head during surgical procedure for aTSA. Subsequent experiments were examined by eight examiners, including five shoulder surgeons and three participants who had adequate knowledge regarding the thumb test and stemless aTSA. To minimize the weight-bearing effect during the compression procedures, the blocks were positioned with the height of the lower end of the sternum for each examiner. A device to stabilize the artificial bone block with a flexible force sensor.
The compression force as well as the contact pressure and area between the block surface and the thumb were measured with a flexible force sensor (I-SCAN40; Nitta, Tokyo, Japan). A thin-film transducer with a saturation pressure of 500 MPa was secured at the surface of the bone models. To prevent the occurrence of shear stress, upper and lower edges of the flexible force sensor were stabilized with adhesive-backed tape. For the biomechanical assessment of the thumb test, the surface of the blocks was compressed with the thumb of the dominant hand for 20 s to minimize the effect of the creep. The compression force, average and maximal contact pressure and contact area at 20 s were recorded. For each bone model, compression was repeated 3 times with a 30-min interval. The mean values obtained from repeated measurements were used for the subsequent analyses. In this study, the examiners performed compression tests using the P-pad, P-tip and H-axis techniques (Figure 3). The compression tests were examined with a randomized order using an envelope method, and the examiners did not ascertain the contact pressure during the experiment. Quantified images of the contact pressures on the plane compressed with the thumb. Each image represents the pressure pattern with P-pad, P-tip or H-axis techniques.
To compare the biomechanical properties of pressure techniques, the maximal contact pressure and area among three techniques were analyzed. In addition, to assess the distribution patterns of the contact pressure for three techniques, the contact area was divided into three regions according to the length: proximal, middle and distal one-third regions of the contacting thumb area (Figure 4). The differences in the mean contact pressure among these three regions were then compared for each technique. Contact area divided into 3 regions (proximal, middle and distal).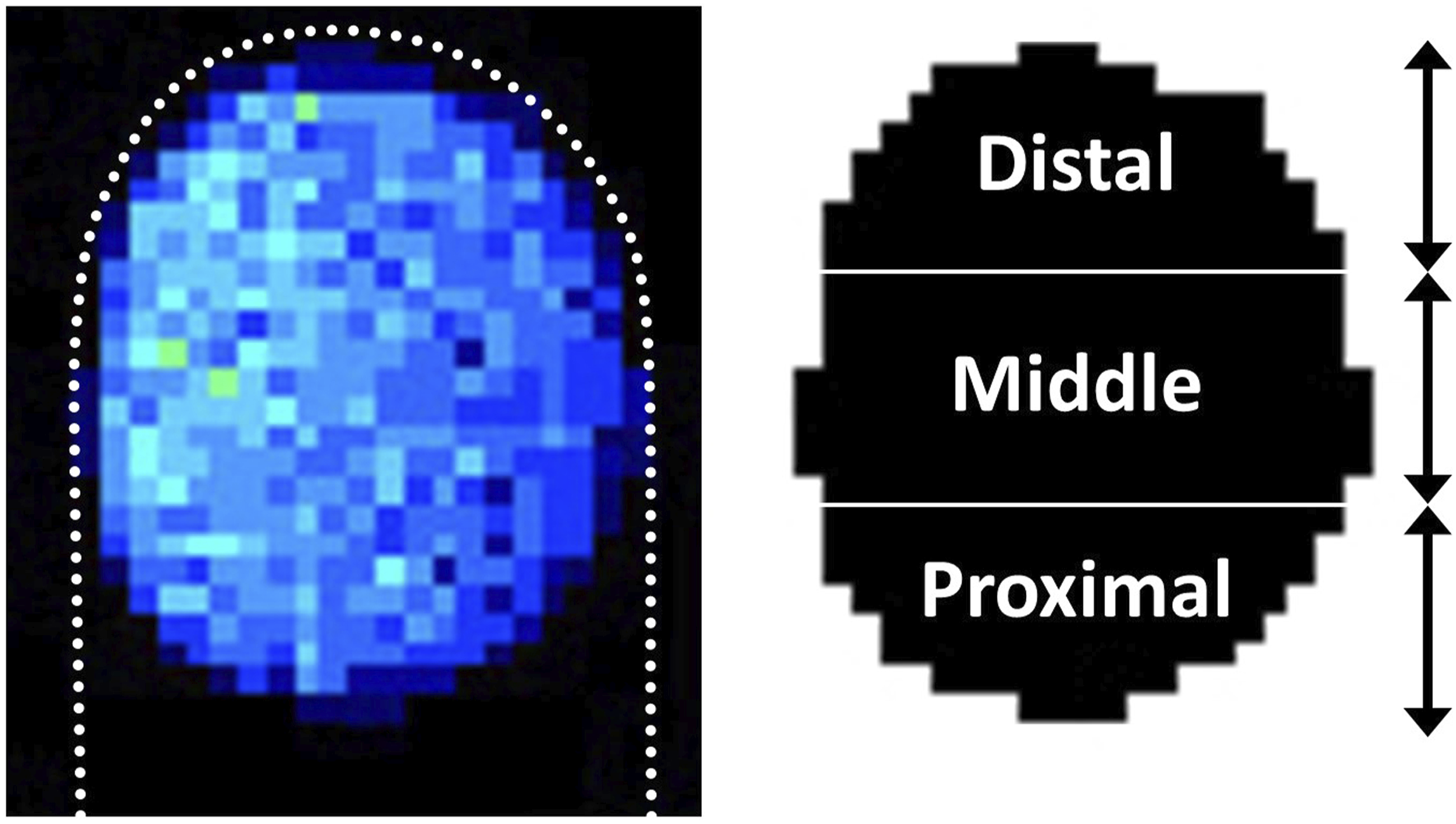
Statistical analyses
The mean values of the contact pressure, compression force and mean and maximal contact pressure and the standard deviation were analyzed. Statistical analyses were performed using the GraphPad Prism 9.0 software program (GraphPad Software, La Jolla, CA, USA). The Friedman test with the post hoc Dunn test was used to assess statistical differences in the contact area, compression force and mean and maximal contact pressures among the three techniques for the thumb test. This test was also used to compare the differences in the mean contact pressure among the three regions (proximal, middle and distal regions) within the contact area.
Results
Responses from 38 arthroplasty surgeons among 95 institutions that had experience with applying stemless shoulder prostheses were received. According to the current surgery, 95% (36/38) of surgeons assessed the bone quality to determine the surgical indication of stemless prosthesis. Among the assessment tools for the bone quality, CT, magnetic resonance imaging (MRI) and X-ray were frequently applied preoperatively. In contrast, BDS to assess the systemic bone mineral density was chosen by only 8% of surgeons. Intraoperatively, 66% (25/38) of surgeons used the thumb test to assess the bone quality at the resection plane of the proximal humerus. Regarding the compression techniques performed by surgeons who adopted the thumb test intraoperatively, the P-pad technique was more commonly used than the P-tip or H-axis techniques (80%, 16% and 4%, respectively, Figure 5). Outcomes to survey the current application of preoperative assessments and intraoperative thumb tests for determining the indication of stemless shoulder prostheses. (a) Assessment of bone quality for steamless prothesis (b) preoperative assessment tools (c) clinical assessment of thumb test (d) compression techniques for thumb test.
Biomechanical measurements for the thumb test.

Median (minimal and maximal) values.

Contact area on the plane with the compression techniques for the thumb test.

Compression force on the plane with the compression techniques for the thumb test.
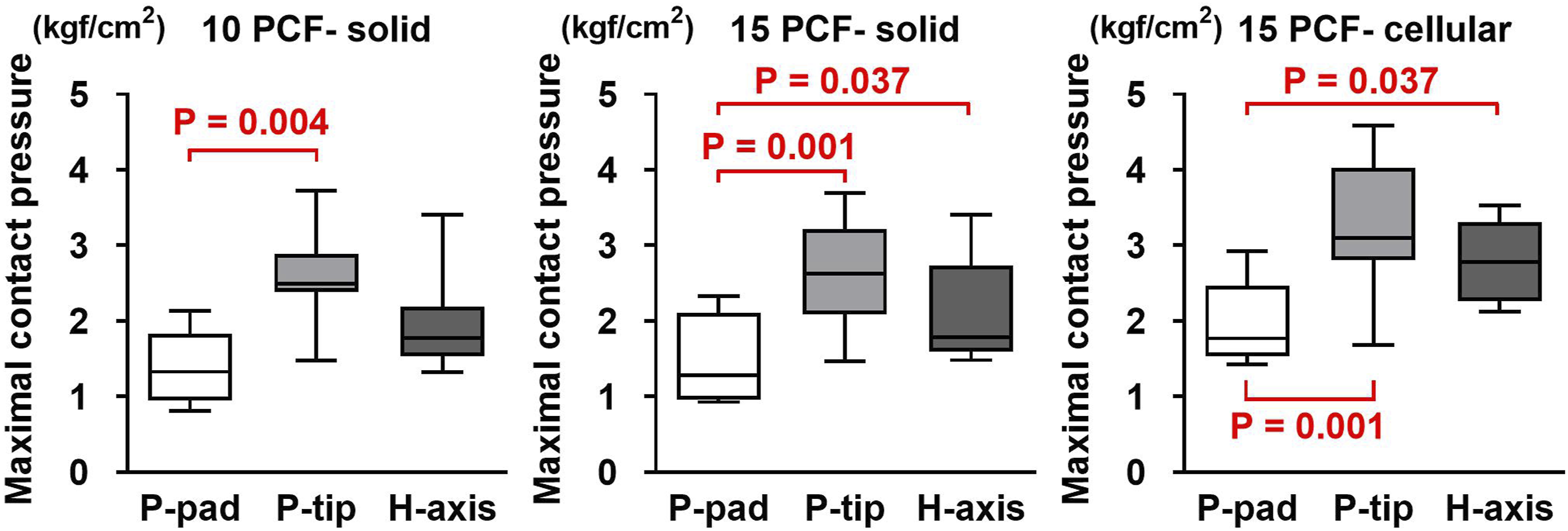
Maximal contact pressure on the plane with the compression techniques for the thumb test.

Distribution of the mean contact pressure on the plane with the compression techniques for the thumb test. P: proximal, M: middle, D: distal.
Discussion
Although stemless shoulder prostheses have recently received focus with showing efficacy in preventing stem-related complications, no criteria for the surgical indication have yet been defined. The current survey assessed the clinical application of pre- and intraoperative assessments among shoulder arthroplasty surgeons in Japan. Most surgeons reported performing a pre- and/or intraoperative assessment of the bone quality at the proximal humerus when applying stemless shoulder prostheses. According to the survey, in addition, most surgeons used multiple assessment tools, including MRI, CT and X-ray, for the preoperative assessment. In contrast, systemic bone mineral density assessed with the BDS was less frequently used, with only 8% of surgeons adopting this approach. The systemic bone mineral density may not correspond to the local bone mineral density, since the localized decrease may be associated with inactivity in the extremity. A recent biomechanical study revealed the importance of a local bone density assessment at the proximal humerus as a predominant factor for determining the mechanical resistance to pressure. 14 Therefore, the current trend in surgeons to prefer to assess the local bone quality at the proximal humerus rather than perform a systemic assessment with BDS may be considered reasonable.
An intraoperative assessment with the thumb test was adopted in 66% of surgeons. Among them, variable compression techniques were used for the test. According to the current survey, the P-pad technique was used more frequently than the P-tip and H-axis techniques. To our knowledge, this is the first attempt to analyze the compression techniques for the thumb test. To date, several studies have mentioned the clinical application of the thumb test7,10; however, detailed explanations regarding the procedure for the test are scarce. Therefore, this study may provide a useful focus with a novel prospective to reveal the preferred compression technique for the thumb test.
We biomechanically investigated the thumb test using synthetic cancellous bone blocks. In our study, detailed biomechanical features, including the contact pressure as well as the contact area and compression force, were demonstrated. In particular, we evaluated the utility of three compression techniques for the thumb test. According to the current results, the P-pad techniques compressing perpendicular to the plane with the thumb pad provided a wider contact area with a more consistent mean contact pressure on the compressed site than the other pressure techniques. Accordingly, our results can be used to determine the most favorable technique in terms of biomechanical efficacy; whereas, the current study also demonstrated that the contact pressure as well as compression force during the test widely differed among the examiners, regardless of the technique used. Accordingly, it should be noted that the thumb test has an unavoidable limitation with regard to objective reproducibility for assessing the bone quality on the resection plane.
There have been a few recent attempts to predict the local bone quality at the proximal humerus for determining the surgical indication of a stemless prosthesis. Levin et al. 8 compared the radiographic characteristics between patients receiving stemless and stemmed prostheses. They reported that the deltoid tuberosity index measured with X-ray and the Hounsfield units on CT were significantly different between the groups. Hayden et al. 9 assessed preoperative CT in patients who underwent shoulder arthroplasty to compare the Hounsfield units at the proximal humerus between those were diagnosed as positive and negative thumb test. They showed significantly decreased values of the Hounsfield units in patients with positive thumb test compared to those with negative thumb test. Chen et al. 15 focused on the local bone mineral density measured at the center of the humeral head, suggesting that stemless prosthesis should be avoided if the local bone mineral density is lower than 0.35 g/cm2. However, the optimal measurement tools for determining the indication of stemless prosthesis remain unclear. Tulner et al. 16 showed that surgeons’ subjective haptic assessments of the bone quality may significantly diverge and, more importantly, may not correspond to the actual bone quality. Based on these findings, further efforts to assess the bone quality are needed in order to determine the surgical indication for a stemless prosthesis.
Several limitations associated with the present study warrant mention. First, we conducted this survey using data from 38 surgeons among 95 institutions that participated in the current survey. Therefore, we were unable to obtain an accurate response rate for the current survey. Second, we used artificial bone models for biomechanical assessments. The utility of artificial bones for biomechanical testing has been reported in the literature. We aimed to assess the biomechanical features of the thumb test under uniform condition, but the potential for geometric variations in cancellous bone structures when utilizing such tests for the proximal humerus should be noted. Third, we did not perform sample size calculation for the current biomechanical study. Although we determined the number of examiners according to the relevant biomechanical studies utilizing artificial bone blocks or assessing the manual test,17–19 we should note potential effect of small sample size for this study. Fourth, there was a lack of reproducibility among the examiners for the current biomechanical analysis. Although we aimed to assess the variation of biomechanical properties corresponding to the thumb test among the examiners, the values of each measurement should be carefully used for the further studies.
Conclusion
The current survey demonstrated the clinical application of the thumb test with relatively frequent use for determining the indication of stemless shoulder prostheses. A biomechanical analysis revealed that the thumb test remains limited in its utility for an objective assessment of the mechanical strength on the plane. Regarding the pressure techniques, the P-pad technique for the thumb test was used with consistent distribution of contact pressure. Further investigations to reveal the feasibility of such assessments for the bone quality are required.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Taku Hatta, a corresponding author, received the provision of study materials from Zimmer Biomet (Warsaw, IN, USA). All authors, immediate family, and any research foundation with which they are affiliated did not receive financial payment or other benefits from any commercial entity related to the subject of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB statement
This study was approved by our institutional review board (JSSCI-R0402).