
Abstract
Background
Total knee arthroplasty is the most effective treatment for advanced-stage knee arthritis, and the majority of knee prostheses are made of metal. Nevertheless, metal prostheses still have several problems. The objective of this study is to introduce new metal-free knee prostheses made of polyether-ether-ketone (PEEK) and to compare their cement bond strength with metal prostheses.
Methods
Twelve sets of knee prostheses were divided into four groups (unloaded PEEK, unloaded Metal, 10 million cycles (MC) PEEK, 10 MC Metal, N = 3 each), and then attached to composite bones using bone cement. Both the 10 MC PEEK and 10 MC Metal groups were subjected to dynamic gait simulations of 10 MC, whereas the other two sets were not. Afterwards, a pull-off strength test was performed on the femoral prostheses and a shear strength test was performed on the tibial prostheses.
Results
No apparent cracks were observed in the bone cement after subjecting the PEEK and Metal groups to 10 million cycles of dynamic simulation. No statistically significant differences were observed (p > .05) in the strength tests for unloaded PEEK vs. unloaded Metal, 10 MC PEEK vs.10 MC Metal in the femoral pull-off test, and for unloaded PEEK vs. unloaded Metal in the tibial shear test. The shear strength of 10 MC PEEK was significantly lower (p < .05) compared to that of 10 MC Metal.
Conclusions
By comparing the force analysis of previous investigations on knee prostheses with the failure pattern observed in the PEEK knee prosthesis of this study, which replicates that of the metal prosthesis. We believe that the combination of the peek knee prosthesis with bone cement is reliable. We anticipate that metal-free PEEK knee prostheses will find application in Total Knee Arthroplasty (TKA) in the future, thereby benefiting patients.
Keywords
Introduction
Total knee arthroplasty (TKA) is one of the most effective treatments for relieving pain and restoring function in patients with advanced-stage knee disease. Most knee prostheses available on the market are constructed from metal. 1 Although metal material prostheses are successful in practice, they still present some unavoidable problems, such as the prostheses loosing and metal hypersensitivity.1–3 Both prosthetic loosening and metal hypersensitivity can cause significant harm to patients and may lead to TKA failure.
The presence of infection and aseptic loosening are among the most important factors affecting the durability of knee prostheses.4–6 There are several factors that can contribute to infection after TKA, including the hospital environment, the procedure of the operation, management of perioperative period and the own physical condition of patients. Currently, the incidence of infection has decreased with advancements in medical treatment.7,8 However, early detection is crucial in determining subsequent treatment options and the patient’s overall outcome. While magnetic resonance imaging (MRI) is a valuable tool for early detection of local infection, it is limited in assessing postoperative intra-articular infection in TKA due to artifacts produced by the metal prostheses. 9 The main causes of sterile loosening are osteolysis caused by polyethylene precipitation and the large elastic modulus difference between metal and human bone that results in stress shielding. 6 In recent years, osteolysis caused by polyethylene particles has been effectively managed through the use of highly cross-linked polyethylene. 10 Stress shielding and subsequent bone resorption, attributed to the disparity in elastic modulus between metal and human bone, have been significant concerns.11–13 Particularly, patients who are undergoing TKA are gradually decreasing in age and increasing in activity requirements.14,15 Therefore, it is important to extend the life of the prosthesis and to preserve the amount of bone around the prosthesis for the revision surgery that may be needed later. 16 Consequently, efforts have been made to explore alternative materials to replace metal, such as polyacetal prostheses with a modulus of elasticity similar to that of human bone, or ceramic prostheses, which possess smoother surfaces that reduce the release of polyethylene particles.17,18 However, both of these protheses have a variety of disadvantages and do not effectively meet the needs of patients in clinical settings.
Polyether-ether-ketone (PEEK) is a polymorphic biomaterial known for its excellent biological inertness and biocompatibility. It has been extensively utilized in orthopedic trauma and spine surgeries since the 1980s.19,20 Its modulus of elasticity is comparable to that of human bone, which can reduce the problem of sterile loosening caused by stress shielding.21,22 Thus, it was considered that PEEK could be used instead of metal to make a knee prosthesis. It is also a suitable option for patients with end-stage knee arthritis who are allergic to metals. In addition, PEEK knee prostheses can be monitored with magnetic resonance imaging to detect signs of infection or tumors around the implant. 23
However, PEEK is a relatively soft material compared to the rigidity of metal, and is more likely to deform under pressure. When introducing a new knee prosthesis, it is essential to verify the strength of its bond with the bone cement. In previous studies, Lennert de Ruiter et al. investigated the initial strength of the PEEK femoral prosthesis bonded to the bone cement and the changes in the bone cement after gait-simulated fatigue experiments.24,25 They found that although the fixation strength of the PEEK femoral prosthesis with bone cement was lower than that of the metal prosthesis with bone cement, it is adequate for human needs. 24 However, they only studied the initial bond strength of the femoral prosthesis to the bone cement, and did not investigate whether the bond strength of the femoral prosthesis to the bone cement remained reliable after dynamic loading to simulate prolonged human activity. Additionally, the study did not assess the bond strength of the PEEK tibial prosthesis to the bone cement.
In the present study, we evaluated femoral and tibial prostheses for their initial bond strength, together with the strength of the prosthesis separately to bone cement after fatigue test simulating 10 years of human activity. This study presents the first metal-free knee prosthesis constructed entirely from PEEK material, including both the femoral and tibial components.
Materials and methods
Groups
This study consisted of four established groups: the Unloaded PEEK group, the Unloaded Metal group, the 10 Million Cycles PEEK group (10 MC PEEK), and the 10 Million Cycles Metal group (10 MC Metal). In order to simulate approximately 10 years of normal activity of an individual, Group 10 MC PEEK and 10 MC Metal prostheses were subjected to 10 million cycles of compressive loading after installation of the prostheses and composite bone. All the prostheses were then subjected to a fixation strength test which included a pull-off test for the femoral component and a shear test for the tibial component.
Materials
This study employed fourth-generation medium-sized composite femur and tibia bones, chosen for their structural resemblance to natural bone. All the knee prostheses were posterior stabilized, left knee prostheses. They were identical in appearance and differed only in terms of material (PEEK vs. Metal). The Unloaded Metal group (n = 3) and the 10 MC Metal group (n = 3) consisted of commercially available universal metallic prostheses (Legion TKA System, femoral component, PS5L, Metal alloy; tibial component, 4L, Ti-6Al-4V alloy; bearing, PS3-4/09, HXLPE). The Unloaded PEEK group (n = 3) and the 10 MC PEEK group (n = 3) were comprised of PEEK prostheses (SinoMed, femoral component, PS5L, ZenivaRPPEK; tibial component, 4L, PEEK; bearing, PS3-4/09, HXLPE), which have the identical geometry with the metal protheses. However, due to the injection molding process, the inner surface of the PEEK prostheses underwent special treatment involving the application of a large rib macrotexture and laser-etched microtexture to facilitate mechanical interlock and enhance surface roughness (Figure 1). We used a high viscosity bone cement (PALACOS®R + G, Heraeus Medical GmbH, Germany) in this procedure. An experienced surgeon performed the installation of composite bone and prosthesis. After the installation of the prostheses, it is imperative to maintain a bone cement thickness of 1-2 mm, adhering to clinical standards (Figure 2). Polyether-ether-ketone (PEEK) prostheses. The inner surface of the PEEK prostheses features a large rib macro-texture and laser-etched micro-texture to achieve mechanical interlock and enhance surface roughness. PEEK prostheses and Metal prostheses. The prostheses have been installed, and the thickness of the bone cement is maintained at 1-2 mm in accordance with clinical standards.

Strength test
All prostheses were commissioned to a specialized laboratory facility (Orthotek Lab., Shanghai, China) for subsequent dynamic compression loading and fixation strength tests. Groups 10 MC PEEK and 10 MC Metal were subjected to a compression loading of 10 MC, simulating the activity of a common person for approximately 10 years (Figure 3). A uniaxial hydraulic testing rig, part of the fatigue testing machine (Dynamo-Eco15), was employed for the reconstructions. The loading was slightly biased towards the medial direction and ranged from 2600 N to 260 N at 10 ± 0.5 Hz. The protocol for the fatigue test was based on the national industry standard for knee replacements. In a prior study, Lennert de Ruiter et al. investigated the effects of cyclic loading and motion on bone cement wear using a similar device.
25
After fatigue test completion, all of the four group protheses suffered from bond strength testing on an electronic universal testing machine (AGS-X-300kN). The components were separated using a displacement-controlled loading (0.05 mm/s). In the femoral prosthesis pull-off test, the femoral prosthesis was fixed to a special device and the force was applied axially to the joint surface of the composite femur and the prosthesis by means of the universal testing machine until the prosthesis separated from the composite bone (Figure 4). Philipp Bergschmidt et al. used a similar device and method to examine the lightness of bonding of metal and ceramic femoral prostheses to bone cement under different conditions.
26
In the tibial prosthesis shear test, after the tibial prosthesis was firmly fixed, the force was applied vertically to the joint of the tibial prosthesis and the composite bone to achieve a shearing effect until the tibial prosthesis separated from the composite bone (Figure 5). Diagram and product picture of the dynamic compression device. The uniaxial hydraulic test stand of the fatigue tester (Dynamo-Eco15) was used to apply a cyclic load of 10 million cycles (10 MC) to simulate 10 years of human knee joint activity. Diagram and product picture of the pull-off test. Clamping claws at both the anterior and posterior ends of the femoral components applied the necessary retention force. Diagram and product picture of the shear test. The applied force acts perpendicularly to the tibia prosthesis until debonding of the component.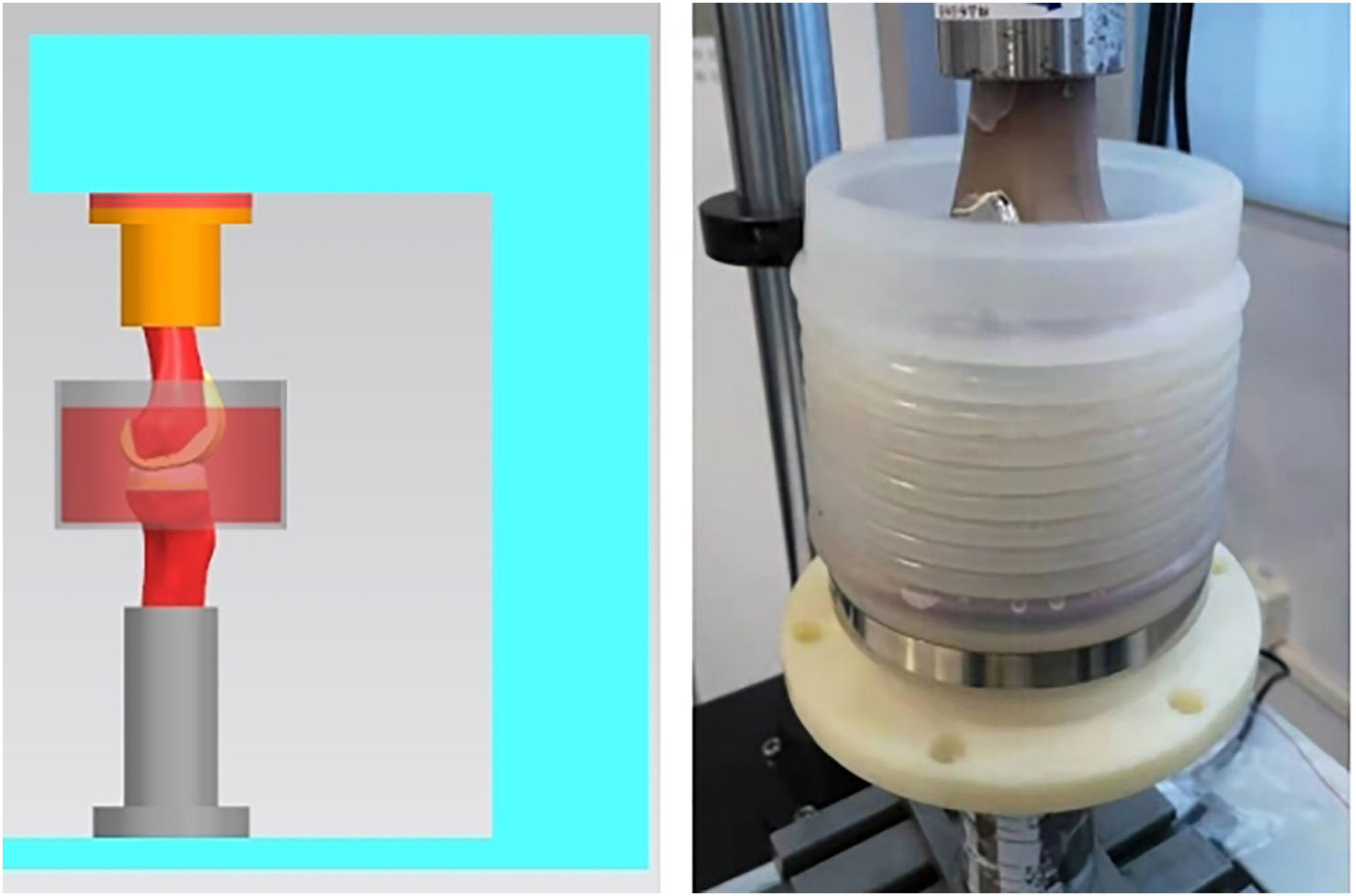


Observation records
Debonding, cracking, deformations, and total failure were observed during the pull-off phase. Throughout the test, we recorded displacements and strengths. Outcome measures included the maximum pull-off strength and failure patterns. Primary failure modes were characterized by the most substantial loss of strength following peak force, including occurrences like cement–femur debonding, cement–implant debonding, or femur fracture. During each pull-out test, a strength versus displacement curve was plotted and the peak load achieved prior to catastrophic failure was recorded as the strength at failure. During the shear phase of the tibial component, we observed debonding, cracking, deformations, and total failure of the component. Additionally, a strength vs. displacement curve was plotted for each shear test.
Statistical analysis
A summary of the data is presented as a mean (±standard deviation) for bond strength. Statistical analysis was performed in SPSS 26.0 using a t test to compare the PEEK and Metal groups. It was hypothesized that PEEK prostheses would exhibit lower bond strength than Metal prostheses. A significance level of p < .05 was applied for statistical significance.
Results
Following 10 MC gait simulation in both the 10 MC PEEK and 10 MC Metal groups, no debonding of the prostheses from the composite femur and tibia was observed, and there were no noticeable macroscopic changes in the bone cement. A crack was observed in one set of composite femurs from both the 10 MC PEEK and 10 MC Metal groups, respectively.
Pull-off testing of PEEK and metal femoral prostheses revealed similar failure patterns, such as femur fracture, debonding between the prosthesis and femur, and the presence of cement residue on the prosthesis (Figure 6). The average maximum pull-off strength of each group when failure occurred was 2920N (±109N) for the unloaded PEEK group, 4669N (±1622N) for the unloaded Metal group, 2885N (±584N) for the 10 MC PEEK group, and 3837N (±642N) for the 10 MC Metal group, respectively. The bond strength of PEEK femoral prostheses with cement was slightly lower than that of metal. However, this difference was not statistically significant (p > .05) (Figure 7). (a) Typical failure mode of PEEK femoral prothesis after pull-off test; (b) Typical failure mode of metal femoral prothesis after pull-off test. It displays the same failure pattern of femur fracture and prosthesis-femoral debonding, accompanied by cement residue. Histogram of the statistical analysis of the pull-off strength. The bond strength between PEEK femoral prostheses and bone cement was slightly lower than that of Metal. However, the difference between them was not statistically significant (p > .05).

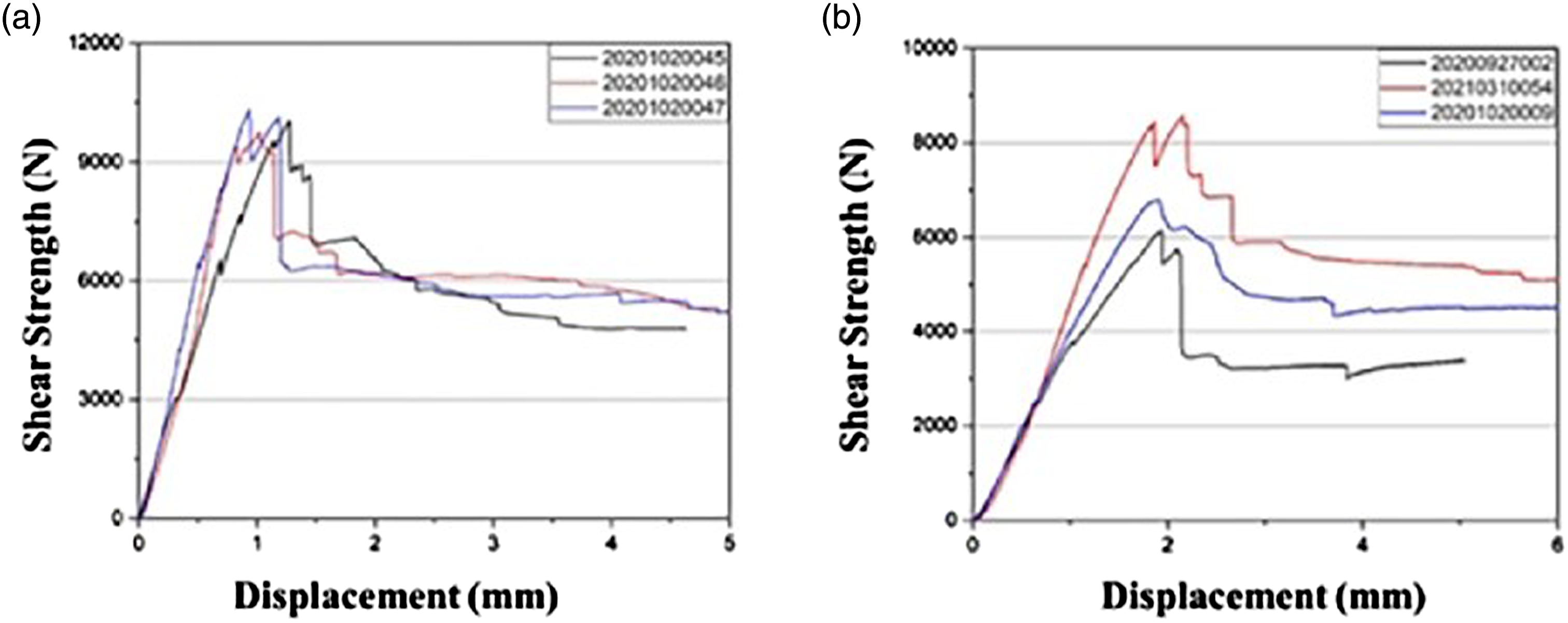
The four groups of tibial prostheses were subjected to shear test, the failure mode was the same tibial brace detached from tibial prostheses (Figure 8), accompanied by a peak force of 5905N (±1046N) for the unloaded PEEK group, 7674N (±942N) for the unloaded metal group, 7160N (±1260N) for the 10 MC PEEK group and 10,034N (±284N) for the 10 MC Metal group. There were no statistically significant differences (p > .05) in the shear strength between the unloaded PEEK group and the unloaded Metal group (Figure 9). While the shear strength of the 10 MC PEEK group was significantly lower than that of the 10 MC Metal group (p < .05) (Figure 9), both strengths improved after dynamic compression. The curves exhibited a similar trend, further affirming the consistency of the failure mechanism (Figure 10). (a) Typical failure mode of PEEK tibial prothesis after shear test; (b) Typical failure mode of metal tibial prothesis after shear test. The failure mode was the same tibial brace detached from tibial prostheses. Histogram of statistical analysis of shear strength. The difference between the unloaded PEEK and Metal groups was not statistically significant (p > .05), but it was statistically significant (p < .05) between the 10 MC PEEK and Metal groups. (a) Shear strength vs. displacement diagram for 10 MC PEEK; (b) Shear strength vs. displacement diagram for 10 MC Metal. The shear strength vs. displacement curves exhibited a similar trend, further validating the consistency of the failure mechanism.

Discussion
This study introduces a novel metal-free PEEK knee prosthesis. We conducted in vitro tests to assess the strength of PEEK prostheses bonded to bone cement, comparing them with the commonly utilized metal prostheses. Besides designing the initial bond strength test, we also tested the bond strength of the prosthesis with the bone cement after fatigue test.
Following the 10 MC gait simulation in both the 10 MC PEEK and 10 MC Metal groups, no debonding of the prostheses from the composite femur and tibia was observed, and there were no apparent macroscopic changes in the cement. In a prior study, Lennert de Ruiter et al. demonstrated that the changes occurring between the PEEK femoral prosthesis and the cement under cyclic loading were not significantly different compared to metal femoral prosthesis. 25 Therefore, in our present study, we focused solely on the macroscopic aspect of the bone cement, assessing it for fragmentation and debonding from the prosthesis.
During bond strength tests with bone cement, the new PEEK prostheses replicated the failure pattern of the metal prostheses, although at a slightly lower strength. No statistically significant differences were observed in the strength tests between unloaded PEEK and unloaded Metal, 10 MC PEEK and 10 MC Metal for femoral pull-off strength, and between unloaded PEEK and unloaded Metal for tibial shear strength (p > .05). While there was statistical significance (p < .05) in the tibial shear strength test between 10 MC PEEK and 10 MC Metal, the bond strength of both PEEK and Metal prostheses with bone cement increased after dynamic compression (5905N ± 1046 N vs. 7160N ± 1260 N; 7674N ± 942 N vs. 10,034N ± 284 N). The PEEK femoral prosthesis replicated the failure pattern of the metal prosthesis and exhibited a fracture of the femoral condyle and separation of the cement from the composite femur after a pull-off test, with the cement and fractured portion remaining on the prosthesis. In terms of initial fixation strength, the bond strength of the PEEK femoral prostheses with bone cement in our experiments was similar to the results of the study by Lennert de Ruiter et al. (2920N vs. 2525 N). 24 Based on a previous in vitro strength-related study of ceramic knee prostheses and a follow-up study of ceramic implants in vivo18,26 Lennert de Ruiter et al. concluded that the bond strength of the PEEK femoral prostheses to the bone cement is fully adequate for the body’s needs. 24
Additionally, in this study, we conducted tests to evaluate the bond strength of PEEK tibial prostheses with bone cement. Previous studies have investigated the factors that influence aseptic loosening of the tibial prosthesis, which is a major cause of long-term TKA failure.13,16,27 Thus, this was a problem that could not be ignored when we introduced the metal-free PEEK prosthesis. The tibial prosthesis is mainly subjected to compression and shear forces during human activity in vivo. 28 In previous studies, push-out test was used to investigate the bond strength between the prosthesis and cement. 29 For this study, we used shear test to verify the bond strength.30,31 After shear testing, PEEK tibial prostheses demonstrated a slightly lower bond strength to bone cement compared to metal prostheses. Regarding initial bond strength, there was no statistically significant difference (p > .05) between PEEK and metal tibial prostheses. However, after fatigue testing, the shear strength of the PEEK group was significantly lower than that of the metal group (p < .05). While the shear strength of Group 10 MC PEEK is slightly lower than that of Group 10 MC Metal, the failure mode was the same. All tibial prostheses were separated from the composite bone accompanied by cement residue. And the curves show a similar trend, further validating the consistency of the failure mechanism. In addition, based on the force analysis of the knee implant by Georg Bergmann et al. they simulated the maximum force on the knee prosthesis in the range of 3372-4218 N for walking, climbing stairs and standing in a single group in a 100 kg weight patient, with a maximum value of 5165 N when jogging, and the shear force on the intra-articular implant is much less than the axial force.28,32 Therefore, the strength of PEEK tibial protheses bonded to bone cement in our experiments is adequate for human needs (7674N ± 942 N vs. 5165 N).
Additionally, our study had some limitations. Firstly, each group included a small number of prostheses (n = 3), which is a recognized constraint in this experiment. However, in a previous validation study by Cristofolini L et al. on the long-term fixation of prostheses in TKA, it was found that three prostheses per group could already clearly distinguish between well-fixed and loosened prostheses. 33 Secondly, the femur and tibia components we used were composite bones. Although they resemble the human skeleton, they may not entirely replicate the true conditions in the human body. Finally, in this study, we only simulated the normal human walking duration of 10 years without considering a longer time frame. Additionally, we did not account for knee motion under special circumstances or the influence of the patellofemoral joint. Both PEEK and metal prostheses have undergone the same experiments, so the results we observed were able to illustrate some phenomena. The above issues could be considered in subsequent experiments.
Based on our results, it seems that while the bond strength of the PEEK total knee prosthesis to bone cement is slightly lower than that of the metal prosthesis, the PEEK prosthesis exhibits a failure pattern similar to that of the metal prosthesis. No statistically significant difference was observed in the initial bond strength to the cement, whether in the femoral or tibial prosthesis. Following fatigue testing, neither the PEEK nor the metal prosthesis exhibited any debonding from the cement, and no cracks were observed in the cement sleeve. No statistically significant difference was found in the bond strength of the PEEK and metal femoral prostheses to the bone cement. These strengths align with previous studies and meet the requirements for human use. While there is a statistical difference in the bond strength of the PEEK tibial prosthesis to bone cement compared to the metal tibial prosthesis after fatigue testing, considering the observed strength changes, the trend in load-displacement curve separation, and previous studies on force analysis of knee prostheses, we confidently assert that both are suitable for human use.
In conclusion, we believe that the metal-free PEEK knee prosthesis designed in this study is reliable and adequate for human needs in combination with bone cement. We anticipate that metal-free PEEK knee prostheses will find application in Total Knee Arthroplasty (TKA) in the future, thereby benefiting patients, although additional trials will be required to verify this.
Footnotes
Acknowledgments
We thank the Suzhou SinoMed Biomaterials Co.,Ltd for providing part of the materials for this study. The PEEK prostheses were completely designed and manufactured by the company.
Author contributions
Conception and design of the work: QJ and ZHX; Data collection: DGZ and SZ; Supervision: QJ and ZHX; Analysis and interpretation of the data: HKT and QJW; Statistical analysis: DXW and HKT; Drafting the manuscript: DXW and QJW; Critical revision of the manuscript: QJ and ZHX; All authors contributed to the article and approved the submitted version.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82272492 and 82002294), National Key Research and Development Project (2021YFA1201404), Major Project of NSFC (81991514), Jiangsu Province Medical Innovation Center of Orthopedic Surgery (CXZX202214), Jiangsu Provincial Key Medical Center Foundation, Jiangsu Provincial Medical Outstanding Talent Foundation, Jiangsu Provincial Medical Youth Talent Foundation and Jiangsu Provincial Key Medical Talent Foundation, the Fundamental Research Funds for the Central Universities (14380493 and 14380494).