
Abstract
Purpose
To report the outcome of a novel fixation technique using three high-strength sutures which is including articular buttress suture, cerclage suture, and tension band with off-loading triceps suture (triple suture fixation) in the treatment of displaced comminuted olecranon fracture with a stable ulnohumeral joint (Mayo type IIB). The rationale of using this technique is that the sutures have been used to stabilize multiple fracture fragments in all sides of the olecranon.
Material and Methods
Between July 2018 and July 2021, 10 patients (7 women, 3 men; mean age, 49.9 years; mean follow-up duration, 27.8 months) with Mayo type IIB olecranon fractures who underwent triple suture fixation were included in the study. The elbow was immobilized in a splint for 2 weeks postoperatively. Range-of-motion exercises were initiated after splint removal and weight bearing was allowed at 6 weeks postoperatively.
Results
Average active range of motion of the elbow was 145° of flexion (range, 135°–150°), 6.5° of extension (range, 0°–30°), 83° of supination (range, 70°–85°), and 77.5° of pronation (range, 70°–80°). Mean MEPS was 98.3 (range, 85–100) and DASH score was 3.1 (range, 0–10) at the final follow-up. Radiographic data at the final follow-up analyzed by paired t test demonstrated that there was no statistically significant difference of proximal olecranon height (OH), trochlear notch width (TW), and OH/TW ratio between postoperative treatment and normal side (p-value >.05). No complication of implant prominence, fixation failure, nonunion, infection or heterotopic ossification was found postoperatively. Breakage of drill bit occurred during drilling a distal oblique hole for articular buttress suture in one patient.
Conclusion
The triple suture fixation is an effective treatment with low incidence of complications in treatment of Mayo type IIB olecranon fractures. Larger comparative studies are needed to confirm the value of such technique.
Keywords
Introduction
Olecranon fractures are common upper extremity injuries, representing approximately 10% of all elbow fractures. 1 Several surgical fixation techniques were described for the treatment of displaced olecranon fractures. 2 Favorable functional outcome is directly related with anatomic correction of the articular surface, repair of the elbow extensor mechanism, restoration of joint stability and motion, and prevention of stiffness and other complications. 3
A common complication of surgical reduction and fixation is discomfort from the prominent metal implants because of the limited subcutaneous tissue in this region. The meta-analysis revealed a high rate of implant removal due to the hardware irritation after TBW and plate fixation. 4 An alternative option to olecranon fracture fixation using high-strength suture was proposed to avoid such complication.5–8 In most of the previous reports, the suture fixation had been used in place of the tension band wiring in non-comminuted olecranon fractures. Due to the principle of converting distraction at the fracture site to compression of the articular surface around the fulcrum of trochlea, several authors suggested that the suture fixation should not be used in comminuted fracture as the fixation could cause articular collapse and loss of joint congruence.6,8 However, many biomechanical studies found a lack of compressive movement at the fracture site.9–11 For this reason, the suture fixation which is functional as a static compression device could also be utilized for comminuted olecranon fracture. 12 To our knowledge, the information regarding the treatment in this group is still limited.
In the present study, the triple suture fixation technique was described for the treatment of displaced comminuted fractures of the olecranon with a stable ulnohumeral joint (Mayo type IIB). The rationale of using this technique is that the sutures have been used to stabilize multiple fracture fragments in all sides of the olecranon. The components of triple suture fixation are following: 1. Articular buttress suture for anatomically restoring the articular surface of greater sigmoid notch 2. Cerclage suture for stably fixing the medially and laterally displaced fragments 3. Tension band with off-loading triceps suture for stabilizing the dorsally displaced fragments and counteracting the triceps distraction force
The purpose of this study is to report the clinical and radiographic outcomes of this fixation method.
Materials and methods
This study included the patients who has Mayo type IIB olecranon fractures treated with triple suture fixation between July 2018 and July 2021. Inclusion criteria were as follows: (1) age 18 or over; (2) minimum of 2 years of follow up; (3) good joint function before elbow injury. Exclusion criteria were as follows: (1) subluxation or dislocation of elbow joint; (2) pathological fracture; (3) previous injury, deformity, or disease at the contralateral elbow. Ten patients were met these criteria. Their medical records were reviewed for demographic data and for preoperative, intraoperative, and postoperative information. This study was approved by the Institutional Review Board; reference number IRBRTA 1239/2566, in accordance with the Declaration of Helsinki Ethical Principles for Medical Research involving human subjects. All patient signed informed consent regarding publishing their data and photographs.
Patients
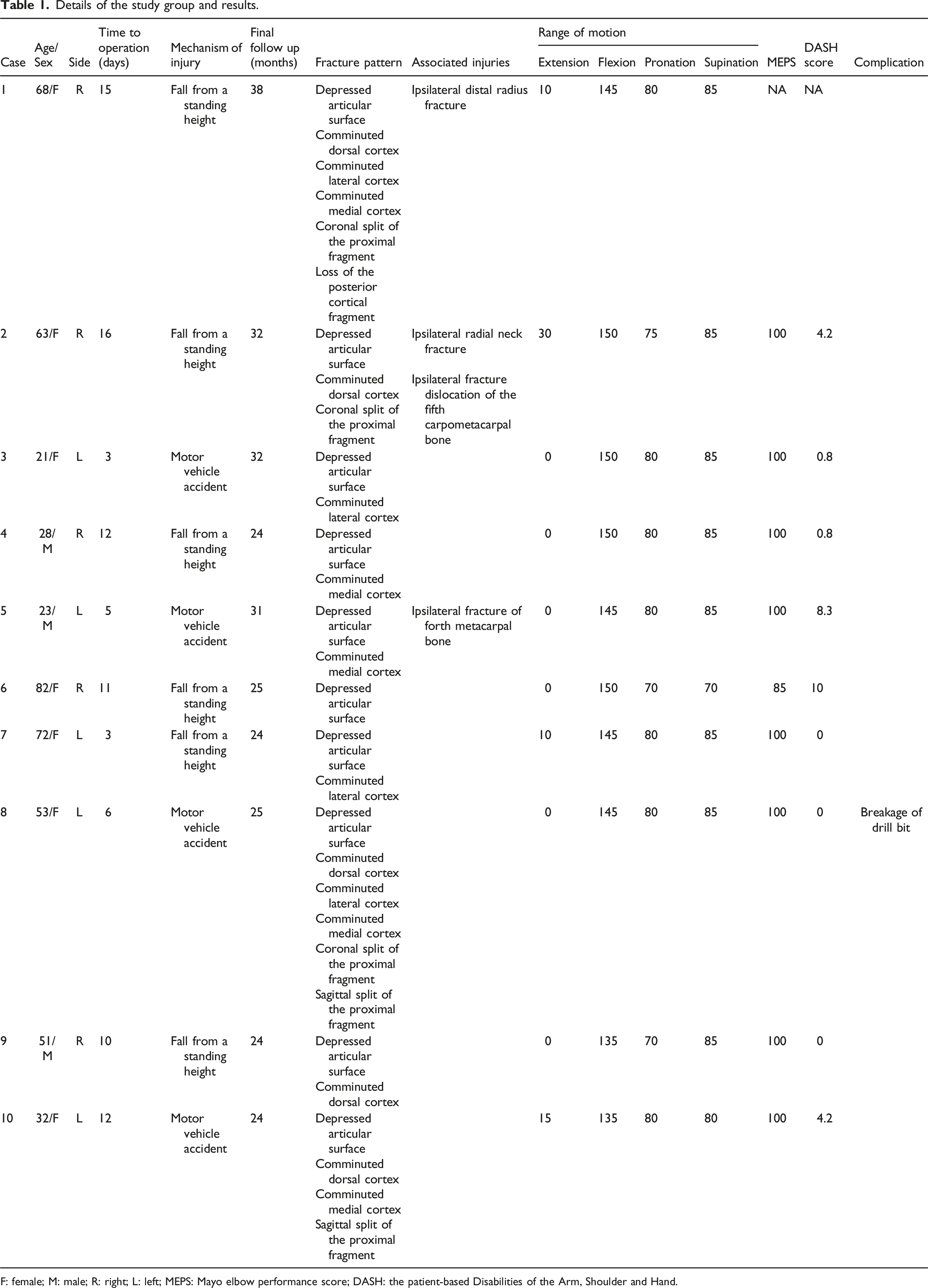
The study group consisted of 7 women and 3 men with a mean age of 49.9 years at the time of surgery (range, 21–82 years). All patients are right hand dominant. The right elbow was involved in 5 cases, the left in 5 cases. The average duration of postoperative follow-up was 27.8 months (range, 24–38 months).
The mechanism of injury included a fall from a standing height in 6 patients, and a motor vehicle accident in 4 patients. One patient had undergone two previous operations for olecranon fracture but the fixations were failed (Patient 1). Preoperative and intraoperative evaluation showed the depressed articular surface in all patients, comminuted dorsal cortex in 5 patients (Patient 1, 2, 8, 9, and 10), comminuted lateral cortex in 4 patients (Patient 1, 3, 7, and 8), comminuted medial cortex in 5 patients (Patient 1, 4, 5, 8, and 10), coronal split of the proximal fragment in 3 patients (Patient 1, 2, and 8), sagittal split of the proximal fragment in 2 patients (Patient 8, and 10), and loss of the posterior cortical fragment in 1 patient (Patient 1). The mean period from injury to operation was 9.3 days (range, 3 - 16 days). The associated injuries of ipsilateral upper extremity were revealed in 4 patients: radial neck fracture (Patient 2), distal radius fracture (Patient 1), fracture dislocation of the fifth carpometacarpal bone (Patient 2), and fracture of forth metacarpal bone (Patient 5). A metal plate due to previous treatment of the ulnar diaphyseal fracture was present in one patient (Patient 9).
Surgical technique
Patients were placed in supine position after anesthesia. The tourniquet was applied on the upper arm. Prophylactic antibiotics were administered before inflation of the tourniquet. A posterior approach centered on the olecranon was performed. The skin and subcutaneous tissue were raised as a single flap. The fracture was exposed. The muscles attached to the proximal ulna were gently elevated from the bone surface only to the extent that it is necessary for the required exposure. A stay suture was placed just above the triceps insertion to manipulate the proximal fragment(s) during the operation. The suture fixation with No. 2 Fiberwire (Arthrex, Naples, Florida, USA) was performed as follows:
Articular buttress suture
Articular surface was addressed by lifting and repositioning of the depressed fragment(s) using a periosteal elevator. Two 2.0 or 2.5-mm holes were drilled in oblique fashion from the fracture site, entered the intramedullary canal and exited the medial and lateral cortices of ulna distally at least 1 cm away from the fracture line. The corresponding holes were drilled in the proximal fragment from the fracture surface, exited the superior surface of olecranon, and passed through the triceps insertion. These holes were made as volarly as possible to buttress the depressed articular fragment(s). A transverse drill hole was made at 1 cm distally to the distal exits of oblique holes. A Fiberwire suture was folded in half. A Nitinol shuttle loop had been used to pass a free end and a loop end of a double-stranded Fiberwire suture through each side of triceps tendon and bony hole from the proximally to distally. One suture end was passed through the transverse hole to exit the opposite side (Figure 1(a)). Triple suture fixation technique in the treatment of displaced comminuted fractures of the olecranon with a stable ulnohumeral joint. (a) Articular buttress suture. (b) Cerclage suture. (c) Tension band with off-loading triceps suture. (d) All knots were designed to be on either medial or lateral border of ulna.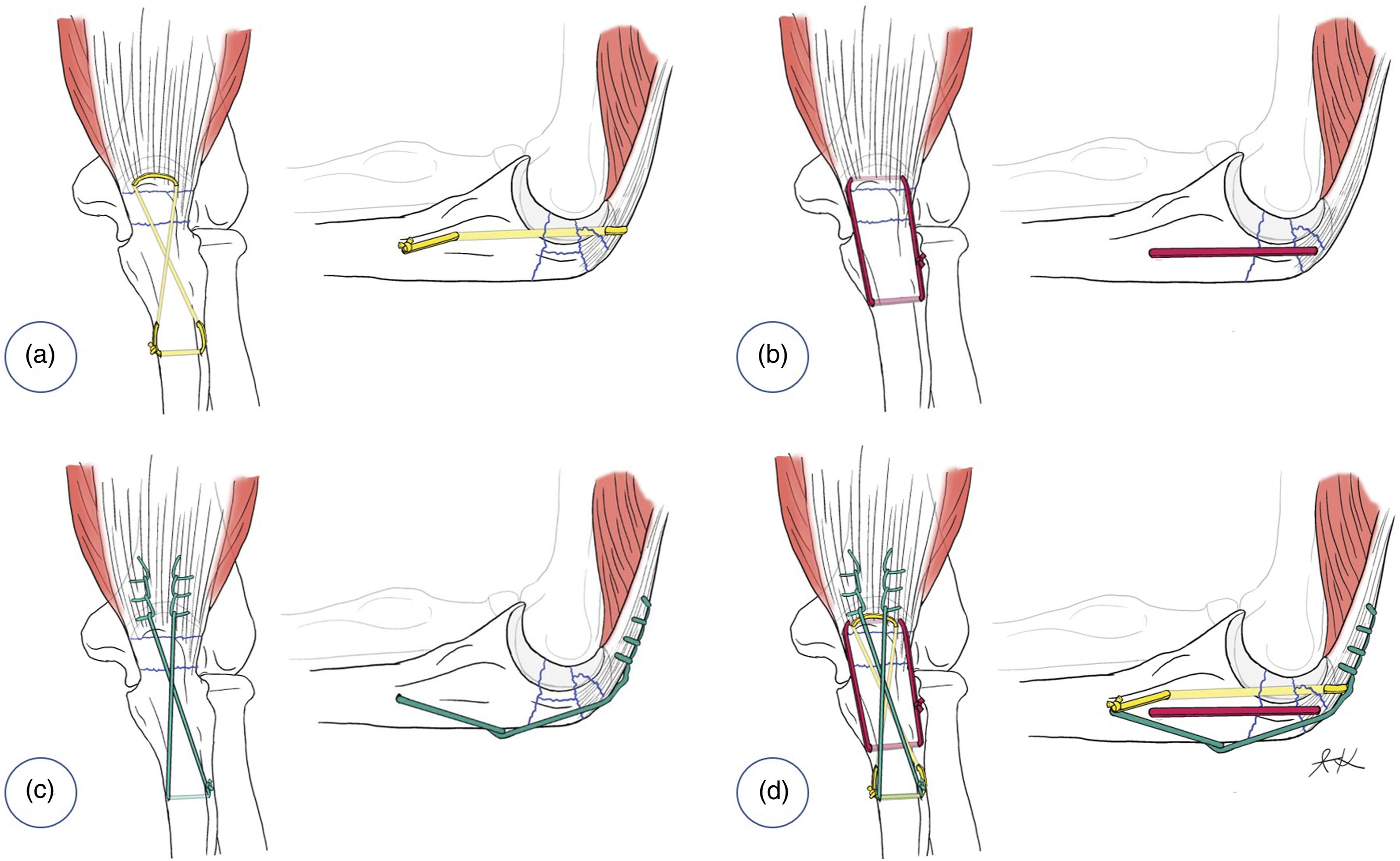
Cerclage suture
Two transverse drill holes for a cerclarge suture were positioned along the dorsoventral axis. One was though the triceps tendon and proximal fragment just distal to the superior surface of olecranon and the other was at 2 cm distal to the fracture. A double-stranded Fiberwire suture was passed through the holes in a circular configuration (Figure 1(b)).
Tension band with off-loading triceps suture
A Fiberwire suture was stitched into the medial and lateral sides of the triceps tendon in a running locking configuration. Each free suture end was passed across the dorsal aspect of the proximal ulna in a figure-of-eight configuration. One suture end was fed through a transverse hole used for articular buttress suture to exit the opposite side (Figure 1(c)).
Nice knot for double-stranded suture and the first throw of a square knot for single-stranded sutures were made. Each suture loop was tensioned while the alignment and geometry of olecranon were assessed using intraoperative fluoroscopy. After appropriate tension was obtained, all knots were locked. The Nice knots was backed up with three alternated half-hitches and the square knot was followed by four alternated half-hitches. To prevent prominence, all knots were designed to be on either medial or lateral border of ulna underneath the forearm muscles (Figure 1(d)).
Postoperative management
The elbow was immobilized with a plaster splint in 90° of flexion for 2 weeks after the surgery. Gentle range-of-motion exercises were initiated after splint removal and progressed as pain allows. Weight bearing was allowed at 6 weeks postoperatively.
Evaluation
The evaluation consisted of range of motion, Mayo elbow performance score (MEPS), the patient-based Disabilities of the Arm, Shoulder and Hand (DASH) score, complication, and radiographic assessment.
Anteroposterior and lateral radiographs of the elbows were reviewed. The reduction quality of greater sigmoid notch including contour defect and intraarticular step-off, olecranon geometry including proximal olecranon height (OH), trochlear notch width (TW), and OH/TW ratio, and posttraumatic arthritis (PTA) were evaluated. Contour defect of greater sigmoid notch was assessed from lateral elbow radiograph using the method described by Murphy et al.
13
. Two perfect circles were formed by the olecranon and by the coronoid process. The distance between the centers of the olecranon and coronoid circular arcs was considered to be the contour defect. Acceptable contour defect was less than 1 mm. Measurement of OH, TW, and OH/TW ratio was performed according to the method proposed by Wadia et al.
14
(Figure 2(a)–(d)). The difference of OH, TW, and OH/TW ratio between postoperative treatment and normal side was evaluated and analyzed by paired t test. A p-value of less than 0.05 was considered statistically significant. Radiographic measurements of the olecranon. (a) Preoperative x-ray showing contour defect of greater sigmoid notch which is a distance (yellow line) between the centers of blue and orange circles formed by the olecranon and coronoid circular arcs, respectively. (b) Postoperative x-ray showing anatomical reduction of greater sigmoid notch combining both circles into one. (c) Preoperative OH (red line) and TW (white line). (d) Postoperative OH and TW. OH: Proximal olecranon height; TW: Trochlear notch width.
The radiographic union has been defined as bridging fracture callus visualized at three cortices on both radiographs. Posttraumatic arthritis was assessed according to the criteria of Broberg and Morrey as grade 0 (normal joint), grade 1 (slight joint-space narrowing and minimum osteophyte formation), grade 2 (moderate joint-space narrowing and moderate osteophyte formation), and grade 3 (severe degenerative changes and destruction of the joint). 15
Representative cases
Olecranon fracture with displaced articular fragment and medial comminution
A 23-year-old male sustained a right elbow injury from a motorcycle accident. Preoperative imaging studies demonstrated a comminuted olecranon fracture with significant intraarticular step-off and disruption of the articular surface of the greater sigmoid notch. Intraoperatively, the displaced articular fragment and medial comminution was seen. The triple suture fixation was performed (Figure 3(a)–(f)). Postoperatively, the patient was satisfied with the surgical outcomes. The x-ray demonstrated that the articular surface was restored with normal contour of greater sigmoid notch. At 31 months postoperatively, the elbow extension was 0°, flexion was 145°, pronation was 80°, and supination was 85°. The MEPS was 100 and DASH score was 8.3. The follow-up x-rays showed that the alignment was well maintained and there was no evidence of posttraumatic arthritis (Figure 4(a)–(g)). Olecranon fracture with displaced articular fragment and medial comminution (Patient 5). (a) Preoperative three-dimensional reconstructed CT images. (b) Intraoperative finding of vertically-oriented depressed articular fragment (c) Articular buttress suture placement after reduction of the displaced articular fragment. (d) Cerclage suture and tension band with off-loading triceps suture placement. (e) Reduction of the fracture from tensioning of all sutures. (f) Tying of all sutures with the suture knots on the medial and lateral aspects of ulna. Postoperative range of motion and plain x-ray of Patient 5. (a) Elbow extension. (b) Elbow flexion. (c) Forearm supination. (d) Forearm pronation. (e) Preoperative elbow x-ray showing displaced articular fragment (yellow arrow). (f) Elbow x-ray obtained at 3 months postoperatively showing the restored articular surface with normal contour of greater sigmoid notch. (g) Elbow x-ray obtained at 30 months postoperatively showing well maintained articular alignment.

Revision in a case of fixation failure
A 60-year-old female who has the underlying of progressive supranuclear palsy with cognitive deficit had a ground level fall. She sustained a Mayo IIB olecranon fracture of the right elbow. The patient presented to us with two failed open reduction and internal fixation (ORIF) procedures. Implant cut-out of the proximal fixation following both procedures was revealed. The first ORIF involved the use of K-wire fixation with tension band wiring. The second ORIF procedure involved double plate fixation. As surgical wound dehiscence at the tip of olecranon with persistent drainage occurred, a surgical debridement with implant removal was done. Intraoperatively, highly comminuted proximal fracture fragment with further fragmentation from previous surgical fixation and loss of some dorsal cortical bony fragments were detected. After we made sure that there was no evidence of infection, the revision with triple suture fixation was performed. Early postoperative radiograph showed reduced articular surface with normal contour of greater sigmoid notch. Decreased olecranon height and OH/TW ratio from cortical bone loss compared with the normal side was revealed. At the follow-up of 3 months after surgery, the elbow extension was 25°, flexion was 115°, pronation was 65°, and supination was 70°. Due to the motor deficit from advanced neurological condition, the functional outcome related to the treatment of olecranon was unable to evaluate at the latest follow-up which was 38 months postoperatively. Range of motion was assessed passively. The elbow extension was 10°, flexion was 145°, pronation was 80°, and supination was 85°. The x-rays demonstrated good maintenance of articular congruity and there was no evidence of posttraumatic arthritis (Figure 5(a)–(f)). Revision in a case of fixation failure. (a) Plain x-ray showing failure of tension band wiring fixation. (b) CT scan after tension band removal showing comminuted dorsal medial and lateral cortex with coronal split of the proximal fragment. (c) Plain x-ray showing double plate fixation. (d) Intraoperative finding of failed plate fixation with screw cut-out of the proximal fragment. (e) Plain x-ray obtained 3 months after triple suture fixation. (f) Plain x-ray obtained 36 months after triple suture fixation.
Results
Details of the study group and results.
F: female; M: male; R: right; L: left; MEPS: Mayo elbow performance score; DASH: the patient-based Disabilities of the Arm, Shoulder and Hand.
The measured postoperative radiographic parameters.

OH: Proximal olecranon height; TW: Trochlear notch width; SD: Standard deviation.
The paired differences of proximal olecranon height, trochlear notch width, and proximal olecranon height/trochlear notch width ratio between postoperative treatment and normal side.
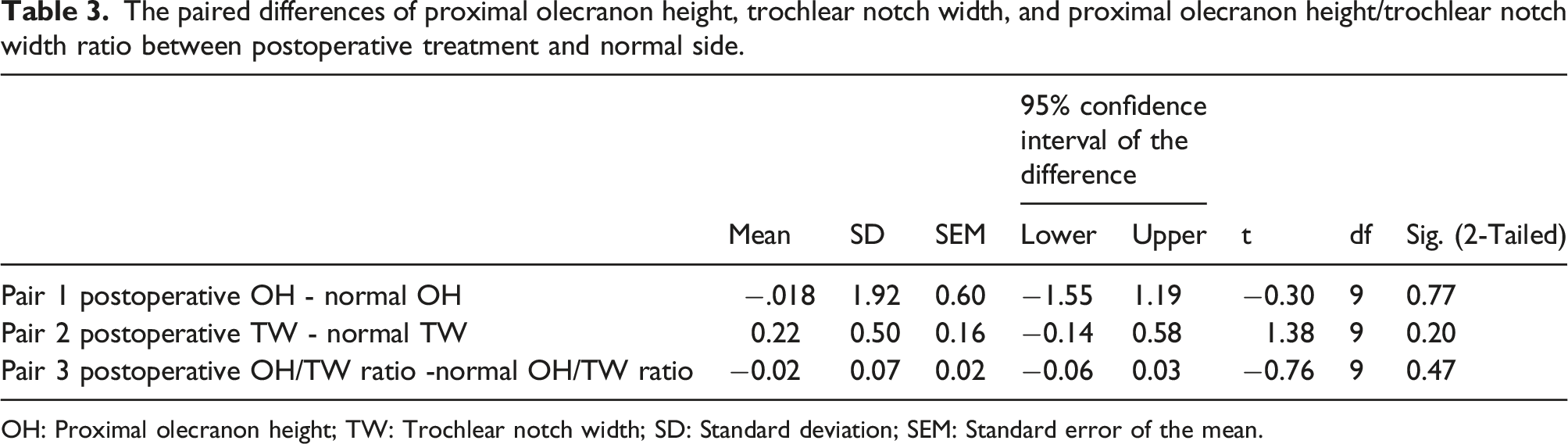
OH: Proximal olecranon height; TW: Trochlear notch width; SD: Standard deviation; SEM: Standard error of the mean.
Radiographic union was achieved in all patients at a mean of 6.1 weeks (range, 5–12 weeks). The radiographs taken at the last follow-up demonstrated a well-maintained ulnotrochear and radiocapitellar joint spaces with no sign of arthritis (grade 0) in all patients.
Discussion
This study reported the outcome of triple suture fixation in treatment of comminuted olecranon fracture. The clinical and radiographic results showed that this technique is an effective treatment with low incidence of complications.
Although most of the previous studies recommended the suture fixation for the simple transverse fracture, a recent study demonstrated that such method could also be used for the comminuted fracture. 12 Based on the existing published data, several surgical techniques were revealed. Das described the suture fixation technique for olecranon fracture using a high-strength suture passed the dorsal and medial-lateral aspects of the proximal ulna to support the fracture. 8 Henseler et al. reported how to use sutures as Kirschner wire and tension and wire for olecranon fractures on 3 elderly patients. 5 One suture was passed as near to the ventral ulna as possible and the other on the dorsal aspect of proximal ulna. Rodríguez et al. performed the suture wiring in the figure-of-eight and circular configurations. 16 An off-loading triceps suture technique was proposed by Izzi and Athwal for augmentation of locking plate for fixation of comminuted proximal fragments. 17 A high-strength non-absorbable suture was stitched into the triceps tendon using a modified Krackow technique and secured to the plate by passing it through the available screw hole or proximal K-wire holes. In the present study, the authors had modified and combined all mentioned techniques for circumferential support multiple small fracture fragments of the proximal ulna.
According to the current concept in surgical management of proximal ulna, precise restoration of the anatomy and stable fixation is essential to enable early functional training of the elbow and inhibit posttraumatic stiffness. 2 Bailey et al. also emphasized the importance of repairing the normal contour of the greater sigmoid notch, especially the anterior and posterior facets of the olecranon. 18 Murphy et al. evaluated the clinical outcome in treatment of displaced olecranon fractures and found that malreduction with an intraarticular step-off greater than or equal to 2 mm was associated with poorer results. 13 Association of symptomatic arthrosis with articular diastasis exceeding 2 mm of olecranon fracture was also reported. 19 In contrast to other surgical options such as plate fixation, intramedullary screw and tension band wiring, the reports regarding postoperative radiographic alignment after suture fixation is limited.13,20 In the present study, the intraartricular step-off could be well restored without the need of bone graft augmentation. The averaged step-off was 0.18 mm and no patient had step-off greater than 2 mm after suture fixation. Lee et al. observed that the more the accompanied preoperative contour defect, the more the postoperative residual contour defect. 20 In their series, an acceptable restoration was achieved only in 43.8% among the cases with preoperative contour defect greater than 2 mm. In our study, all patients obtained adequate restoration despite having contour defect greater than 2 mm preoperatively. We hypothesized that articular buttress suture was possible the key of the positive outcome in reparation of the articular step-off and contour defect.
Several kinds of high-strength sutures were described for olecranon fixation.5–8,12,21 In this study, Fiberwire which is a high-strength braided suture composed of polyester and polyethylene had been used. Carofino et al. revealed that Fiberwire has similar biomechanical characteristics and fatigue patterns to metal wires utilized for tension band wiring. 22 Triple sutures in the present study consists of two of double-stranded sutures and one of single-stranded sutures. Double-stranded sutures have been proven to increase the strength of fixation compared with single-stranded sutures.23,24 Double-stranded sutures performed in this study were tied with Nice knot which is a lockable sliding knot. 25 According to its properties, we could adjust and maintain that length of the comminuted fragments from tensioning and locking of the sutures, respectively. The appropriate dimension of olecranon can be assessed using intraoperative fluoroscopy based on the reference of parameters from a previous study or contralateral elbow radiographs. Wadia et al. performed a radiographic study of the normal elbows and demonstrated the average proximal olecranon height (OH), trochlear notch width (TW), and OH/TW ratio which could be applied to guide the maintenance of geometry during the fixation of comminuted olecranon fractures. 14 A retrospective study with pre- and postoperative CT analysis showed that reduction based on the posterior ulnar cortex in cases presenting with minimal dorsal cortex comminution could restore acceptable greater sigmoid notch in 14 of 23 patients (60.9%). 20 Success rate of such technique in significant comminuted fracture of dorsal cortex have never been investigated.
The main purpose of using suture fixation in treatment of olecranon fracture is to minimize the risk of implant prominence which is the leading cause of reoperation.26,27 Nimura et al. knotted Fiberwire on the dorsal surface of the proximal ulna. 7 Das et al. are buried the knots beneath the anconeus muscle laterally. 8 Henseler et al. tied one suture knot lateral to the triceps insertion and one suture knot volar to the triceps insertion. 5 Xu et al. experienced knot prominence which required removal and suggested placed the knot at the location which has good soft tissue coverage. 12 As the triple suture technique which had been used in this study formed multiple knots, a distal transverse drill hole was made for placement the knots on the medial or lateral border of ulna underneath the forearm muscles to avoid the knot prominence. We were aware that extended surgical incision and further soft tissue dissection was required in creating an additional drill hole; however, a compromise in wound healing and functional outcomes was not observed. A comparative study demonstrated that nice knot of double stranded suture provided less bulkiness than square knot of single stranded suture. 24
For displaced comminuted proximal ulna fractures, open reduction and internal fixation with a locking plate is usually recommended for the treatment of choice. 2 However, as fragment size decreases, the ability to achieve fixation with a plate becomes difficult and screw placement may lead to further fragmentation. 28 Loss of fixation was found in 8.3% of the patients with geriatric olecranon fractures managed operatively with a locking plate. 29 Revision in a case of fixation failure is challenging due to the bone fragmentation and presence of previous screw holes. Excision of the comminuted fragments and triceps advancement was described as a salvage procedure if internal fixation fails. An in vitro study demonstrated that excision and triceps advancement resulted in abnormally elevated intraarticular contact stresses, whereas open reduction and internal fixation restored restores the normal biomechanics of the elbow joint. 30 In this study, favorable outcome was obtained from triple suture fixation in a patient who had failed double plate fixation.
In elderly with osteoporosis, there is a concern about using suture fixation because the suture may cut-through the bone.8,31 A case of dorsal cortical fracture of the suture tunnel leading to loss of reduction and subsequent malunion was reported. Phadnis and Watts highlighted that care must be taken not to leave too small bone bridge between the suture holes in osteoporotic bone. 31 Suturing through triceps tendon to recruit it as part of the construct instead of passing the suture solely through the soft bony fragments was advocated to reduce the possibility of cut-through.12,17 In the present study, triple suture fixation was consistent with both suggestions. The locations of the suture holes were set to provide sufficient bone bridge in the distal part, and all three sutures were passed through triceps tendon in the proximal part. Favorable results were obtained in treatment of the elderly patients (Patient 1, 6 and 7). Owing to the directions of transosseous tunnels in triple suture fixation which resulted in acute or right angle of suture passage, suture abrasion and bone wear around the tunnels may occur. 32 Although these possibilities could compromise the fixation strength, satisfactory radiographic outcome in restoration of the olecranon alignment was still obtained in the present study.
In this study, surgical drill bit breakage occurred in one patient. The possible reason for breakage was deflection of drill bit due to the oblique angle hole drilling on thick cortical bone of proximal ulna with a small diameter of drill bit (2.0 mm). In addition, such drill bit was re-used. No migration or change in position of retained metalwork was observed with the follow-up x-rays at 25 months postoperatively. Several reports demonstrated that the drill bit fragments that left in situ do not cause any complication if they are entirely within the bone.33,34 A single-use drill bit with larger diameter (2.5 mm) and optimal directional drilling may prevent this complication.
The limitations of this study are small sample size and no comparison with other fixation techniques. In addition, the quality of fracture reduction was evaluated with plain radiographs which may not as accurate as the CT scan.20,35 Although some of the data of suture fixation in comminuted olecranon fracture were published previously,12,17 our study presented the different technique in fixation of the articular portion and outer surface. Furthermore, this study is the first to focus on quality of reduction from suture fixation in olecranon fracture. Larger comparative studies are needed to confirm the value of triple suture fixation technique.
Conclusion
The triple suture technique is a viable option in treatment of displaced comminuted olecranon fracture with a stable ulnohumeral joint. Effective restoration of greater sigmoid notch contour and olecranon geometry was obtained with this technique. Fixation without the metal implant could avoid the hardware complications and may reduce the operative cost.
Supplemental Material
Supplemental Material - Triple suture fixation for displaced comminuted olecranon fracture with a stable ulnohumeral joint
Supplemental Material for Triple suture fixation for displaced comminuted olecranon fracture with a stable ulnohumeral joint by Suriya Luenam, and Arkaphat Kosiyatrakul in Journal of Orthopaedic Surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.