
Abstract
Background
Proper coronal alignment of the limb is of vital importance in the progression of knee osteoarthritis even in the long-term survivorship of component after total knee arthroplasty (TKA). Nevertheless, to the best of our knowledge, the relationship between coronal fibular axis and tibial mechanical axis had not reached a consensus in the literatures available. The current study aimed to explore the anatomic relationship between tibia and fibula alignment.
Methods
A total of 100 patients with knee osteoarthritis scheduled for total knee arthroplasty were enrolled in this study (Group A), and radiographic measurement was compared to a control group of 100 healthy volunteers without knee osteoarthritis (Group B). Full-length standing hip-to-ankle radiographs were used to assess limb alignment. The angle between coronal proximal fibular anatomic axis and tibia mechanical axis (PFTA) was used to represent the anatomic relationship between tibia and fibula alignment. A negative value indicates fibula varus relative to tibia mechanical axis, while a positive value indicates fibula valgus.
Results
The mean PFTAs were −0.9° ± 0.9° and −1.0° ± 0.8° in Groups A and B. There was no significant difference between the two groups. No significant difference was detected in PFTA distribution in the group A and B. When the mean value of PFTA is used as baseline data, the percentage of subjects in which the PFTA deviation was within 0.5°, 1°, and 1.5° was 51%, 84%, and 94% in Group A and 53%, 87%, and 96% in Group B. There was also no significant difference in distribution deviation between the two groups. No patient-specific factors were correlated with the PFTA.
Conclusions
The proximal fibular anatomic axis is a reliable landmark for tibial mechanical axis in the coronal plane in patients with or without knee osteoarthritis.
Introduction
Proper coronal alignment of the limb is quite important because malalignment is not only related to aberrant biomechanical loading on the articular cartilage of the knee that leads to degeneration and osteoarthritis but also correlated with poor long-term survivorship of component after TKA.1–4 Due to the development and other factors, large anatomic variation of the knee joint in different patients makes it difficult to evaluate alignment in clinical work, especially in the outpatient clinic, and intraoperative assessment, and there is even no consensus regarding the definitions of tibial mechanical axis. 5 Although some techniques are fairly accurate to help surgeons evaluate limb alignment, such as full-length standing digital anteroposterior radiography, computed tomography (CT), and robot-assisted surgery system, additional devices and software increase economic burden and examination time and labor costs, which limit their widespread application in the clinic, especially in developing countries.6–8 Furthermore, plain radiography of the knee is the most common approach in the clinic, especially in the outpatient clinic, and is almost the only method used to assess limb alignment during intraoperative fluoroscopy in TKA, high tibial osteotomy, and reduction of tibial plateau fracture. Thus, it is practical guiding significance to find a reliable landmark on plain radiography to determine the coronal tibial mechanical axis.
The fibular axis has gained extensive attention in this field.9–12 The fibular axis has been recognized as a reliable landmark for tibial sagittal alignment and is used as an important reference for tibial posterior slope cut and component implantation.9,10 However, the correlation between coronal fibular anatomic axis and tibial mechanical axis lacks evidence and is controversial in limited literatures. Some authors reported that the fibula is a reliable landmark for coronal tibial mechanical axis,1,9 while others thought it is not.5,11 The different ethnic origins of patients, imaging examinations, and definitions of tibia and fibula axes may be the major reasons. Meanwhile, all these studies enrolled patients with advanced knee osteoarthritis who underwent TKA, and there is no information on the relationship between the fibula and tibia axes in subjects without knee osteoarthritis.
Therefore, we conducted this study to determine (1) the correlation between coronal anatomic axis of proximal fibula with 10 cm and tibial mechanical axis in patients with advanced knee osteoarthritis and (2) whether there is a difference in the relationship between proximal fibular anatomic axis and tibial mechanical axis in patients with or without knee osteoarthritis. We hope that our study findings will reveal the anatomic relationship between proximal fibula and tibial mechanical axes, which can help surgeons evaluate coronal tibial alignment on common plain radiography of the knee.
Patients and methods
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. 13 This study was approved by the Institutional Review Board (IRB) of the authors’ affiliated institutions. Before examination, written informed consent and research authorizations were obtained from all participants. What’s more, they were informed that data from the research would be submitted for publication and gave their content.
Study population
A consecutive series of 324 patients with knee osteoarthritis who underwent 336 TKAs at the current center from August 2019 to November 2019 were prospectively enrolled in the study. A total of 224 patients were excluded based on the exclusion criteria. Therefore, 100 knees in 100 patients were included in the study as the experimental group (Group A). Another consecutive series of 100 volunteers were recruited as the reference group (Group B) during the same period.
Exclusion criteria
The exclusion criteria were as follows: (1) knee flexion contracture >15°; (2) ipsilateral hip or ankle joint disease; (3) secondary osteoarthritis due to history of trauma, infection, tumor, or congenital disorders; (4) previous history of surgery or fracture in the ipsilateral lower limb; (5) aberrant internal or external rotation of the limb for any reason; and (6) valgus knee.
Inclusion criteria
The following were the inclusion criteria for OA group (Group A): 14 (1) Repeated knee joint pain over the past month; (2) X-ray images (standing position or weight-bearing position) show narrowing of the knee joint space, subchondral bone sclerosis, and/or cystic changes, and formation of osteophytes at the joint edges; (3) Morning stiffness lasting less than 30 min; (4) Audible bone crepitus during activity. The inclusion criteria of control group (Group B) were as follows: (1) age >70 years with no history of knee pain; (2) absence of lower extremity deformity; (3) and absence of radiographic osteoarthritis (KL-0/I) on radiography according to the Kellgren-Lawrence classification. 15
Date collected
Demographic information was collected for all participants, including age, sex, weight, and height. Body mass index (BMI) was calculated as the weight in kilograms divided by height in meters squared (kg/m2). Full-length standing hip-to-ankle anteroposterior radiographs were obtained from all participants using a standardized radiographic technique as previously described.16,17 All radiographs were reviewed by the sophisticated joint surgeon with the strongest criteria for adequacy, and the fibular head and lesser trochanter were used as landmarks to determine excessive rotation of the limbs. All radiographic measurements were performed on anteroposterior radiographs using the onscreen cursor (Philips Extended BrillianceTM Workspace), with an accurate measurement within 0.1°. 16
Definition
The coronal tibial mechanical axis was defined as a straight line from the lateral border of the tibia eminence to the center of the distal tibial plafond on anteroposterior radiography (Figure 1). The proximal fibular axis was defined as the anatomic axis of the proximal fibula 10 cm distal to the apex of the fibular head (Figure 1). The PFTA was designated as the proximal tibiofibular angle, which represents fibula varus compared with tibial mechanical axis when it is assigned a negative value, while fibula valgus appeared as a positive value. The hip-knee-ankle (HKA) angle was used to determine knee alignment.
16
The tibia and fibula lengths were also measured to perform correlation analysis. The tibia length was defined as the straight-line distance between the apex of the lateral tibia eminence and center of the distal tibia plafond (Figure 1). The fibula length was defined as the straight-line distance between the apex of fibular head and most distal end of the fibula (Figure 1). Lower limb X-ray. (a) The PFTA was shown. (b) The tibia length and the fibula length were presented.
Statistical analysis
The intra- and inter-observer measurement reliabilities were determined using intra-class correlation coefficients (ICCs). To test inter-observer reliability, the radiological measurements were independently performed by two investigators according to the same method. To test intra-observer reliability, all measurements were repeated three times at intervals of 2 weeks. The mean values of the angles between the individual axes obtained by taking repeated measurements were used in the following statistical analysis. Continuous data were presented as means and standard deviations, and categorical data were presented as frequency. We used the Mann–Whitney U test or Student’s t-test to compare the differences in continuous variables for two groups after normality tests using chi-square test for each dataset. Categorical variables were compared using chi-square test or Fisher’s exact test, as appropriate. The Pearson’s correlation analysis was performed to determine the relationship between the PFTA and other individual variables, such as BMI, HKA, and tibia length. A two-tailed p-value <.05 was considered statistically significant. Statistical analysis was performed using SPSS® software version 19.0 (IBM, Armonk, New York, USA).
Results
Measurement of intra- and inter-rater reliability.

PFTA: the angle between coronal proximal fibular anatomic axis and tibia mechanical axis; HKA: hip-knee-ankle angle.
Demographic data of the subjects with and without knee osteoarthritis.

HKA: hip-knee-ankle angle.
*p values were calculated using student’s t-test or Mann–Whitney U test.
ap values were calculated using chi-square test or fisher’s exact test.
Distribution of PFTA in subjects with and without knee osteoarthritis.

PFTA: the angle between coronal proximal fibular anatomic axis and tibial mechanical axis.
*p values were calculated using Student’s t-test or Mann–Whitney U test.
ap values were calculated using chi-square test or fisher’s exact test.
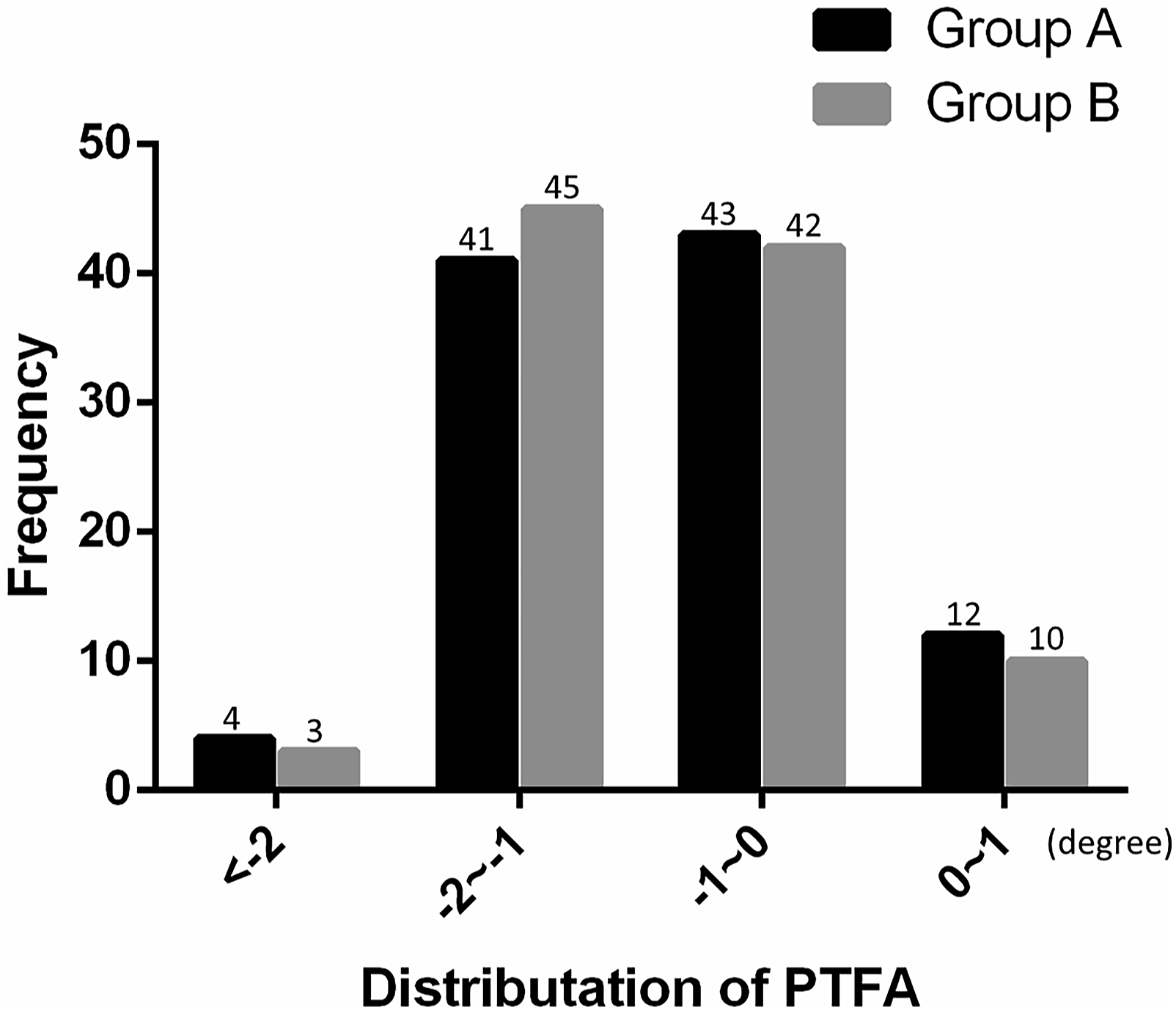
The neutral distribution of PFTA was presented.
Correlations between the PFTA and patient-specific factors.

PFTA: the angle between coronal proximal fibular anatomic axis and tibia mechanical axis; R: pearson’s correlation coefficient.
*Pearson’s correlation coefficient is used to evaluate the relationship between PFTA and height, weight, BMI, HKA, tibial length, fibula length.
Discussion
The tibial joint line is an important anatomic characteristic affecting knee joint biomechanical loading that is directly associated with the development and progression of knee osteoarthritis as well as long-term survival rate of TKA components,1–4,7 and the objective assessment of the tibial joint line is dependent on tibial mechanical alignment, which may be difficult to measure sometimes due to requirement of special devices, such as intraoperative fluoroscopy, in community hospitals and some developing countries. Routine knee radiography is widely used in the clinic because it is an easy and convenient approach to detect bone and joint lesions without additional equipment and manpower, thus exploring reliable anatomic landmarks on knee radiography to help surgeons in making a meaningful preliminary judgment on abnormal tibial plate development and tibia malalignment is dramatically necessary. The current study found that there is little variation in the angle between the proximal fibular anatomic axis and tibial mechanical alignment in the coronal plane; moreover, the anatomic parameter is relatively stable and there is no significant difference among patients with or without knee osteoarthritis. The mean value between the PFTA was −0.9° of varus, and the percentages of subjects with a PFTA deviation within 0.5°, 1°, and 1.5° were 51%, 84%, and 94%, respectively. None of the patient-specific factors, such as height, BMI, HKA, and tibial/fibula length, was correlated with PFTA. Therefore, the proximal fibular anatomic axis may be an appropriate landmark for representation of the tibial mechanical axis.
The anatomic relationship between the tibial mechanical axis and fibular axis in the coronal plane is ambiguous. It is controversial in different literatures even in the same ethnic origin using the same 3D CT measurement technique with the same definition of tibia and fibular axes.5,11 Tsukeoka 5 reported fibular shaft axis as a landmark for coronal tibial mechanical alignment and defined fibular shaft axis as a tangential line connecting the most prominent parts of the fibular head with the lateral malleolus. The mean angle between the fibular axis and tibial mechanical axis was 2.9° ± 0.6° of valgus (range, 4.3° valgus to 1.6° of valgus) without large variation among individuals. When the fibula is used as a reference guide with 3° of varus, all knees can possess proximal tibial cutting guide within 2° of the tibial mechanical axes. However, Kuroda 11 reported that the mean angle between the tibial mechanical axis and fibular shaft axis was 0.9° ± 2.0° (range, >3° varus–>3° of valgus) with large variation among individuals. The percentage of subjects in which the fibular shaft axis was within 2° of the tibial mechanical axis (range, −2°–2°) was 69.3%, and the percentage of subjects in which the fibular shaft axis was within 2° of the mechanical axis with a 3° varus inclination was 45.2%.
Although several studies have explored the association between the fibular axis and tibial mechanical axis, the different selected anatomic landmarks and definition criteria of fibular axis and tibial alignment in various studies make the truth far and near. Moreover, all these studies only included patients with knee osteoarthritis.5,9–12 The lack of a clear definition of normal knee anatomic structure may be the main barrier to designing a research program including the normal knee.9,11,12 Therefore, the anatomic relationship between the fibular axis and tibial mechanical axis in the normal population is unclear. Meanwhile, whether the PFTA is affected by lower extremity alignment is also unknown. This study selected the anatomic axis of the proximal 10 cm of the fibula as landmark based on clinic experience and literatures,5,12,18–20 and we enrolled patients without lower extremity joint diseases as a control group, which defined age >70 years as the fundamental inclusion criteria. Although the cause of knee osteoarthritis is unclear, it’s believed that age is one of the most evident risk factors for osteoarthritis. The increasing incidence of osteoarthritis with age is a result of cumulative exposure to various risk factors and biological age-related changes in the joint structures,21–23 and the aberrant anatomic structure and biomechanical loading is thought to be an important pathogenic factor; thus, we choose old individuals without radiographic knee osteoarthritis rather than young volunteers to represent probable normal knee anatomic structure. We found that there was no significant difference in PFTA value between patients with knee osteoarthritis and those without osteoarthritis; furthermore, the correlation analysis demonstrated that there was no correlation between the PFTA and HKA. Our results in the current study were nearly the same as those of other studies, based on knee osteoarthritis population. Xie et al. 12 reported that the tibiofibular angle was not influenced by individual variables, such as BMI and HKA. These results suggest that the PFTA is an anatomic parameter without large variation, which is not influenced by lower extremity alignment or knee degeneration. Therefore, the proximal fibular anatomic axis is a reliable landmark for coronal tibial mechanical axis. The PFTA was designated as the anatomic relationship between tibia and fibula alignment, which represents fibula varus compared with tibial mechanical axis when it is assigned a negative value, while fibula valgus appeared as a positive value. The result of this study could be used to assess limb alignment during intraoperative fluoroscopy in TKA, high tibial osteotomy, and reduction of tibial plateau fracture. Our study has several limitations. First, all participants in this study were ethnically Chinese. Our findings might be difficult to directly extrapolate to patients from different ethnic groups because anatomical features of the tibia and fibula can vary with the ethnic origin of patients. Second, there was no consensus regarding the definition of the tibial mechanical axis. Some authors defined the tibial mechanical axis as the straight line from the center of the tibial component to the center of the distal tibial plafond based on 3D CT measurement,5,11 while others defined it as a straight line from the center of the tibial proximal plateau to the center of the ankle on radiography.9,12 In this study, we defined the tibial mechanical axis as the straight line from the lateral border of tibia eminence to the center of the distal tibial plafond on anteroposterior radiography. This definition is based on projection of Akagi’s line on the coronal plane, which is used as an important reference for tibial component position during TKA.24,25 If the definition of these axes changed, the results would also change. Third, although we used strict criteria to complete radiographic test, excluded participants with low-quality radiographs, and obtained a satisfactory measurement reliability, we did not evaluate the actual effect of minor internal or external rotations of the lower extremity on the results. This may lead to error when our finding is applied in the clinic based on radiography with minor rotation of the limb. Fourth, due to limited sample size and low incidence of valgus knee, all subjects recruited in the present study showed neutral or varus alignment, patients with a valgus knee were not evaluated, and the results may not be generalized to patients with valgus knee deformity.
Conclusion
From the literatures analyzed and with our study, it is possible to confirm that the proximal fibular anatomical axis is a reliable landmark for the tibial mechanical axis in the coronal plane in patients with or without knee osteoarthritis. We provided a simple auxiliary method, which does not require additional time or surgical equipment, to assess the coronal tibial mechanical alignment on anteroposterior plain radiography of the knee or intraoperative fluoroscopy.
Footnotes
Acknowledgements
What’s more, we want to express our sincere appreciation to all participants joined this study.
Author contributions
Shangkun tang and Xuelin pan were the major contributors to the study design and revision. Shangkun tang and Xuelin Pan wrote the original draft of the manuscript. Renyuan Xu and Xiaojun Shi critically revised and edited the manuscript for the significant intellectual content. Shangkun Tang was responsible for the data curation and formal analysis. All authors approved the final manuscript and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No. 81871780, 82072420) and the Special Scientific Research Projects of China — The safety and effectiveness evaluation of arthroplasty (No. 201302007).