
Abstract
Background
The combination of distal osteotomy with lateral dissection in joint-preserving surgery for severe hallux valgus deformity has recently begun to yield encouraging results. We examined the frequency of complications and risk factors of those for joint-preserving surgery in patients with and without rheumatoid arthritis (RA).
Methods
A retrospective, observational study of 72 feet (27 patients with RA) was performed. The inclusion criteria were patients who underwent joint-preserving surgery for hallux valgus deformity at our hospital between January 2008 and March 2016 who could be followed up with for longer than 12 months.
Results
The mean preoperative and immediate postoperative hallux valgus angles (HVA) were 41.8 and 4.4, respectively. The mean preoperative and immediate postoperative intermetatarsal angles between the first and second metatarsal bones (M1-M2A) were 14.6 and 5.8, respectively. At the final postoperative evaluation, the mean HVA was 8.8 and the mean M1-M2A was 6.4.
Data were compared among the patients with complications (recurrent valgus deformity, varus deformity), and those without complications (normal HVA) at the final postoperative evaluation. The rate of RA in the varus deformity group was 71.4%, which tended to be higher than in other groups (p = .058). The mean preoperative HVA were 48.2 and 52.6 in the group of recurrent valgus deformity and varus deformity, which was higher than the normal HVA group (p = .001).
Conclusions
High preoperative HVA was a risk factor for the recurrence of valgus deformity. Most of the varus deformities were observed in the RA group with high preoperative HVA; therefore, caution should be exercised in operating on patients with severe deformity or those with RA.
Level of evidence
III.
Introduction
Hallux valgus is more common in women than in men, and genetic and other various factors are believed to be involved in this multifactorial disorder.1–8
Nonoperative treatment, such as exercise and orthotics, is used for relatively mild deformity cases; however, in severe cases, it may be ineffective, in which case surgery is often needed. Proximal, metaphyseal, and distal osteotomies are all considered effective,9–15 and recently, encouraging results have been obtained from joint-preserving surgery for severe deformity by combining distal osteotomy with lateral dissection.16,17
Foot surgery is increasingly common in patients with RA, and joint-preserving surgery is becoming mainstream in the treatment of hallux valgus with the improvement of inflammation control by drug therapy.18,19
Complications such as recurrent valgus deformity, varus deformity, and osteonecrosis of the metatarsal head have been reported in joint-preserving surgery.17,20
The purpose of this study was to examine the frequency of complications and risk factors.
Materials and methods
Study design and patient population
Patient characteristics and parameters of deformity.

*mean ± SD, BMI: body mass index; RA: rheumatoid arthritis; HVA: hallux valgus angle; M1-M2A: intermetatarsal angle between the first and second metatarsal bones; M1-M5A: intermetatarsal angle between the first and fifth metatarsal bones.
Surgical procedure
First, a 2 cm skin incision is made on the dorsolateral side of the metatarsophalangeal (MTP) joint of the great toe to identify and dissect the adductor tendon. Second, a skin incision is made medially along the metatarsal of the great toe from the MTP joint to the tarsometatarsal joint. Third, a 1 cm wide, 4 cm long flap of the medial capsule and the medial metatarsal periosteum is created, protecting the nerve to expose the MTP joint surface. Fourth, a distal osteotomy is performed at approximately 2 cm proximal from the articular surface, with an approximately 3 mm step created in the middle of the bone width to shorten the metatarsal. Two Acutrak mini (Acumed, Oregon, USA) or one Acutrak mini and one Acutrak micro (Acumed) were used for fixation. The medial flap was sutured to the metatarsal with traction, aiming for HVA of 0-5°, being careful not to overcorrect (Figure 1). Representative (a), (c) preoperative and (b), (d) postoperative radiograph.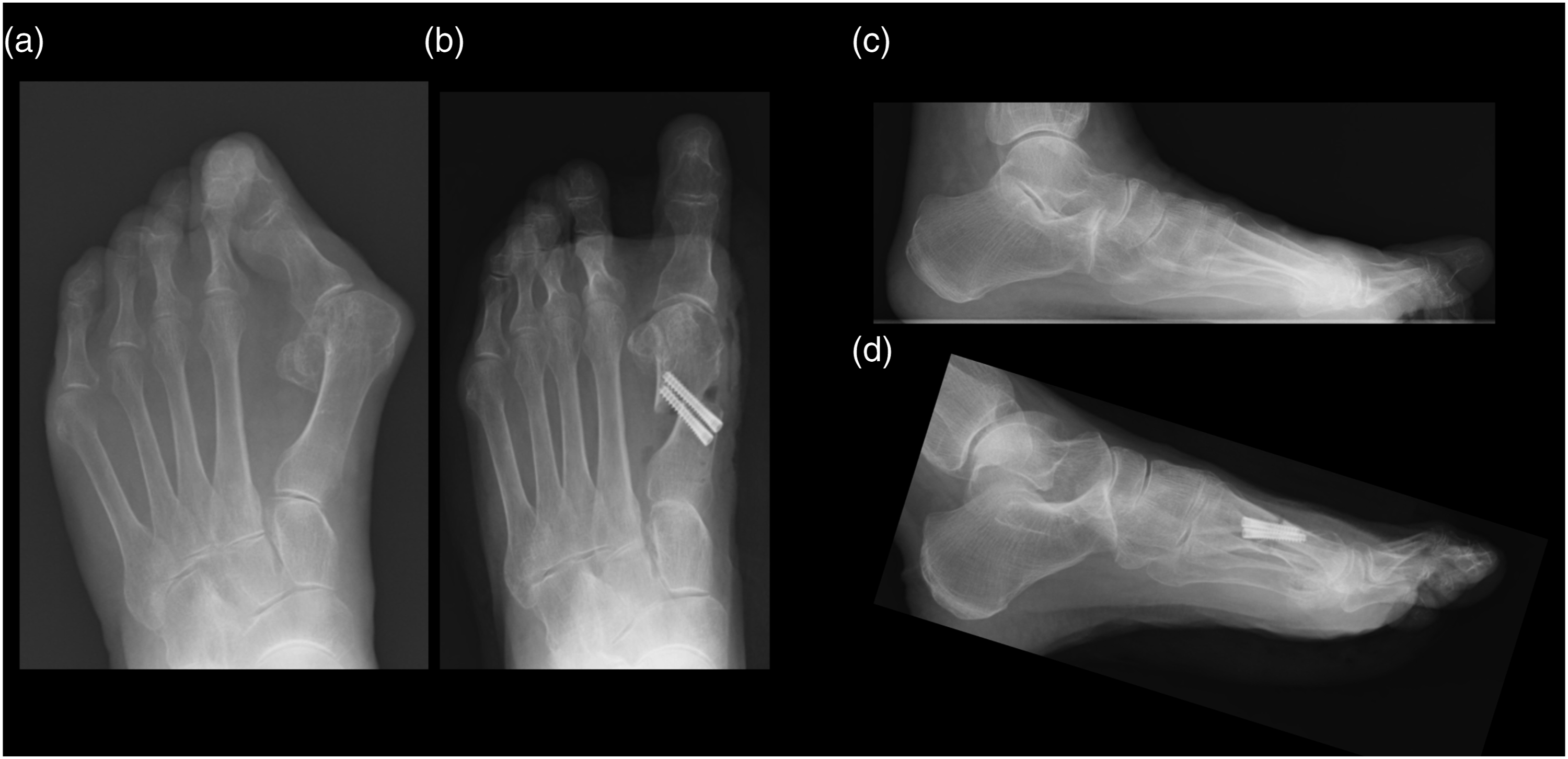
Radiographic assessment
Dorsoplantar or anteroposterior weight-bearing radiographs were taken, and the radiographic assessments were performed as described previously.23–25 Measurements were taken of the HVA, the M1-M2A, and the angle between the first and fifth metatarsal bones (M1-M5A). The HVA and M1-M2A were evaluated on preoperative and immediate postoperative radiographs. For the HVA, data at the last follow-up were also included. The lateral talocalcaneal (TC) angle and the calcaneal pitch angle (CPA) were measured on the weight-bearing lateral foot radiographs to evaluate the level of hindfoot and flatfoot deformity. In addition, the first MTP (MTP1) joint space narrowing (JSN) ratio and the MTP1 joint erosion ratio were investigated.
Complications
We defined the recurrence of valgus deformity as HVA exceeding 20 degrees, and the varus deformity as HVA of less than -5 degrees at the final postoperative evaluation.
Furthermore, we examined the frequency of metatarsal head necrosis and nonunion.
Statistical analyses
Statistical analyses were performed using GraphPad Prism 9 (GraphPad, California, USA). Differences with p values of <.05 were considered significant.
Results
The mean age of the patients in this study was 62 years, 89% of patients were women, mean body mass index was 22.6, 27 toes had RA as an underlying disease, the rate of simultaneous lesser toe surgery was 29.2%, and the mean postoperative follow-up period was 33.2 months. The mean preoperative and immediate postoperative HVA were 41.8 and 4.4, respectively, and the preoperative and immediate postoperative M1-M2A were 14.6 and 5.8, respectively. Moreover, the mean preoperative M1-M5A was 33.4. At the final postoperative evaluation, the mean HVA was 8.8 and the mean M1-M2A was 6.4 (Table 1).
Characteristics and parameters of deformity in each deformity group.

*mean ± SD, BMI: body mass index; RA: rheumatoid arthritis; HVA: hallux valgus angle; M1-M2A: intermetatarsal angle between the first and second metatarsal bones; M1-M5A: intermetatarsal angle between the first and fifth metatarsal bones; lateral TC angle: lateral talocalcaneal angle; CPA: calcaneal pitch angle; MTP1 JSN: first metatarsophalangeal joint space narrowing.
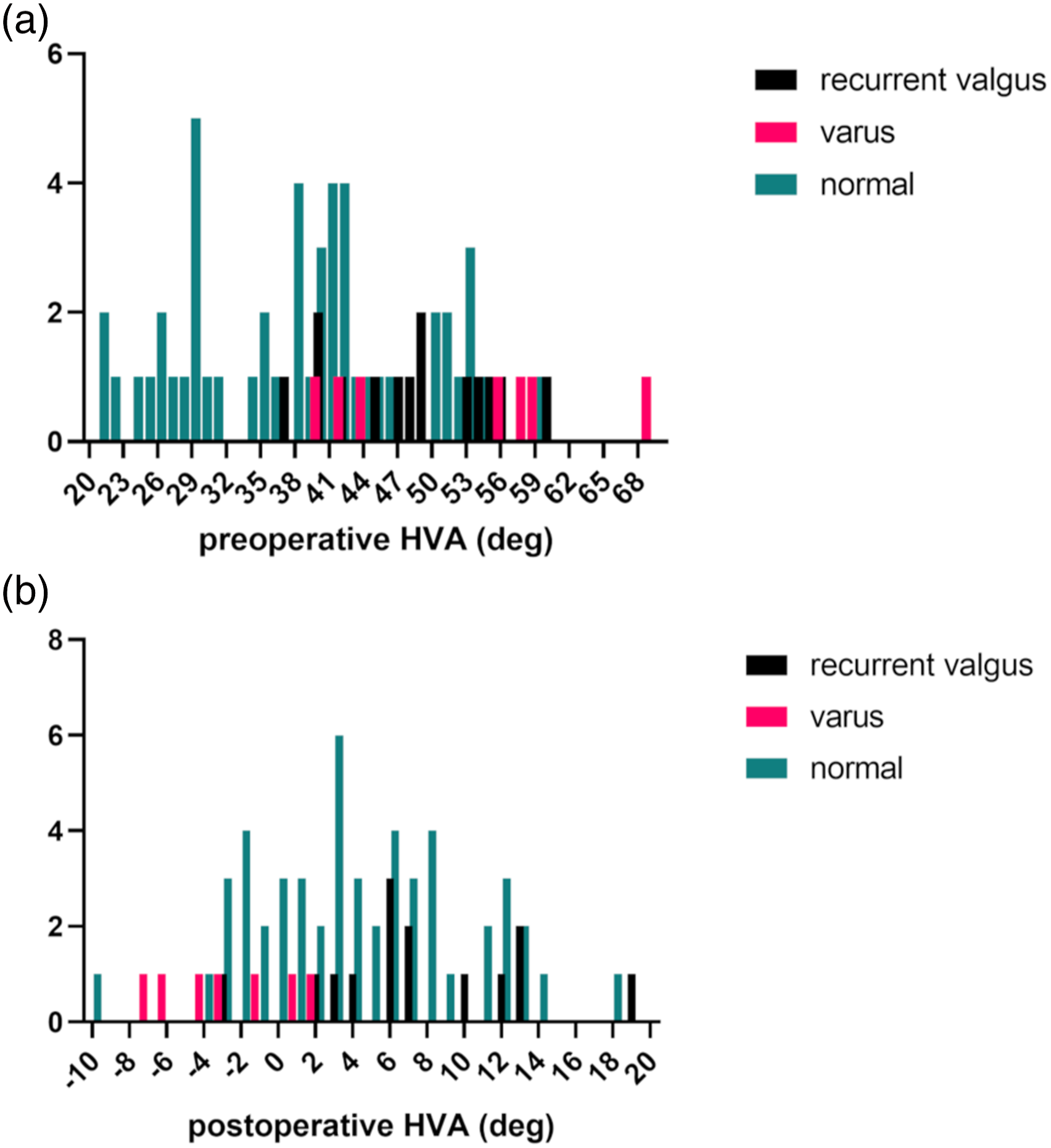
The histogram of (a) preoperative hallux valgus angle (HVA) and (b) immediate postoperative HVA.
Characteristics and parameters of deformity in each disease group.

*mean ± SD, BMI: body mass index; HVA: hallux valgus angle; M1-M2A: intermetatarsal angle between the first and second metatarsal bones; M1-M5A: intermetatarsal angle between the first and fifth metatarsal bones; lateral TC angle: lateral talocalcaneal angle; CPA: calcaneal pitch angle; MTP1 JSN: first metatarsophalangeal joint space narrowing; RA: rheumatoid arthritis.

The transition of hallux valgus angle (HVA). The preoperative HVA, the immediate postoperative HVA and the HVA at the final postoperative evaluation in the patients (a) without or (b) with rheumatoid arthritis.
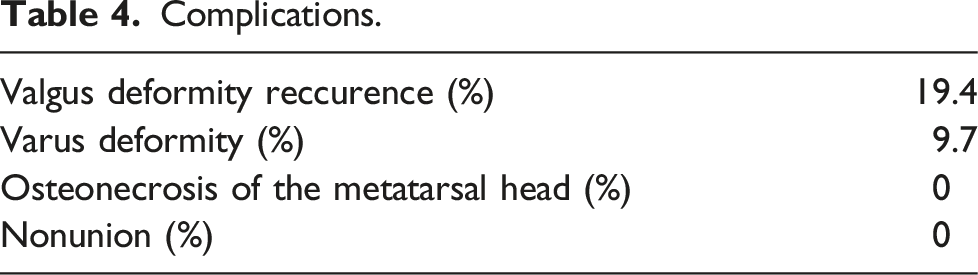
Complications.
Discussion
In this study, 19.4% of the patients had recurrent valgus deformity and 9.7% had varus deformity. Complications were a little more frequent than in other recent reports, partly due to the high preoperative HVA in this study.20,26
High preoperative HVA was a risk factor for the recurrence of valgus deformity. This was consistent with previous reports. 27 If the preoperative HVA was high, the risk of recurrence of deformity was high even if the postoperative HVA was appropriate. In such cases, additional assessment may be needed about the overall deformity, including cases of hindfoot deformity.28–30
High preoperative HVA was also identified as a risk factor for varus deformity. In addition, overcorrection of HVA was considered a possible cause. Most of the varus deformities were observed in the RA group, so it is necessary to be careful about overcorrection, especially in patients with RA and with high preoperative HVA.
Limitations of this study included the limited single-center retrospective data, the small number of cases, the lack of functional evaluation, and the lack of data about RA inflammation control.
In addition, it would be more useful to evaluate the hindfoot deformity as a part of the imaging evaluations. In the future, the addition of these data and the accumulation of cases will contribute to the prevention of complications in this surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.