
Abstract
Objective
Pharmacotherapy is the most common strategies to reduce pain for osteoarthritis (OA) patients. To analyze the trend and pattern of prescription analgesic medication use in American OA patients. Besides, our study also tried to figure out the demographic characteristics of opioid use among OA population which may helpful for managing the use of opioids.
Methods
We included 2214 OA patients from 2007 to 2018. We extracted data from National Health and Nutrition Examination Survey (NHANES) database. We compared analgesics and anti-depression medications use by category between survey participants with OA and without.
Results
For OA patients, NSAIDs, acetaminophen and gabapentinoid were the mostly highly used analgesics (10.2%, 9.0% and 8.9%, respectively). However, we also found that opioids use was very common in OA patients (7.7%) and the duration of opioids use was significantly long. In addition, the opioids use did not decrease from 2007 to 2018, while gabapentinoid increased rapidly from recent decade (From 5.0% to 12.1%). The common analgesic combination used by OA population was opioids with acetaminophen and gabapentinoid with selective serotonin reuptake inhibitors (SSRIs) (2.9% and 2.7%, respectively).
Conclusion
The use of gabapentinoid increased rapidly from recent decade, while opioids use did not decrease. The long-term excessive use of opioids was also a serious problem for OA pain control. More improvements such as focusing more on healthcare education and paying more attention on non-pharmacotherapy and the psychological situation of patients are needed.
Highlights
• Understanding the trend and pattern of prescription analgesic medications use for OA patients could be helpful for further pain management and guidelines developing. • We found that opioids use was very common in OA patients and the duration of opioids use was significantly long. In addition, the opioids use did not decrease from 2007 to 2018, while gabapentinoid increased rapidly from recent decade • Patients with higher BMI, higher depression score, lower income level and more medical comorbidities were more likely to use opioids for pain relief.
Introduction
Osteoarthritis (OA) is a very common condition which leads to pain, disability and wide healthcare costs.1,2 Because increasing obesity rates and aging populations, OA is becoming more and more prevalent globally. 3 Nowadays, OA affecting more than 240 million people worldwide. 4 Previous studies pointed that OA patients utilized much more healthcare resources compared to patients without OA.5,6
Pain is the most common symptom of OA, which may lead patients to seek medical treatment, contribute to functional limitations and decrease quality of life. 7 Moreover, pain is the leading reason for OA patients to seek healthcare. 8 Currently, OA treatment is mainly focusing on pain relief which was considered as palliative. Among them, pharmacotherapy is the most common strategies to reduce pain for OA patients, including paracetamol, non-steroid anti-inflammatory drugs (NSAIDs), opioids, gabapentinoid and some antidepressants.9,10 The US Centers for Disease Control and Prevention recommended that non-pharmacologic therapy and non-opioid pharmacologic therapy should be the preferred treatments for chronic non-cancer pain control. 11 However, excessive opioid use is very common among OA patients.12,13 Understanding the trend and pattern of each prescription analgesic medication use in clinical practice can help develop further guidelines and improve quality of OA management.
The trend and pattern of prescription analgesic medication use among US adults with OA is scarce. Real-world evidence is really helpful for decision-making process related to therapeutic regimens, prescribing behavior and patients’ management. 14 Examining the trend and pattern of prescription analgesic medication for pain release in real-world clinical practice can help us learn the trend and shortage in OA management. Therefore, the aim of precent study was to analyze the trend and pattern of prescription analgesic medication use in American OA patients. Besides, our study also showed the demographic characteristics of opioid use among OA population which may helpful for managing the use of opioids.
Methods
We collected data from the National Health and Nutrition Examination Survey (NHANES) database. The National Center for Health Statistics (NCHS) research ethics board evaluated all survey protocols used by the NHANES and informed consent must be provided. 15 For this study, we used data extracted from the 2007–2018 survey cycle. All data were obtained from NHANES directly in deidentified form, and thus this study did not require additional Institutional Review Board approval.
The OA samples were defined as participants in the survey who reported current osteoarthritis at the time of the survey. OA was diagnosed according to the International Classification of Diseases, 10th revision (ICD-10) diagnosis codes for OA (Table S1). Because some comorbidities might affect the use of pain related prescription analgesic medication, for total participants (with or without OA), we excluded participants who with gout (n = 521), cancer (n = 1261), fracture (n = 2896), rheumatoid arthritis (n = 538), psoriatic arthritis (n = 73), other arthritis (n = 296), iritis/uveitis (n = 87), ulcerative colitis (n = 268), and Crohn’s disease (n = 48) from our study to avoid the bias. Because methadone, buprenorphine, buprenorphine and naloxone were usually used to treat opioid dependence or withdrawal. 16 To decrease the bias of opioid dependence, we excluded samples who used these opioids in this study. We extracted data including demographic characteristics (age, sex, race, body mass index [BMI]), education and income level, Patient Health Questionnaire 9 (PHQ9) score, work pattern (vigorous and moderate work), exercise pattern (vigorous and moderate exercise) and health conditions (medical comorbidities).
Information about prescription analgesic medications use was collected by interviewers at the participants’ house. The interviewers recorded the name and duration of each prescription analgesic medications that had been used by the participants. Interviewers also requested to see the prescription bottles when it was available. We mainly studied the common analgesics used for OA such as acetaminophen, NSAIDs, cyclooxygenase-2 (COX-2) inhibitors, opioids, gabapentinoid, topical lidocaine, muscle relaxants, duloxetine, benzodiazepines and tricyclic antidepressants.
Besides, common anti-depression medications which were not typically used for pain relief were also included in our analysis, including selective serotonin reuptake inhibitors (SSRIs) and other antidepressants.
Statistical analysis
We compared analgesics and anti-depression medications use by category between survey participants with OA and without. For OA participants, we further calculated the median duration of use for each medication and the frequency of drug combinations. Descriptive statistics are reported as means ± standard deviations (SD) or numbers with percentages as appropriate. Student’s t-test was used for the comparison of continuous variables and the Chi-square test was used for the comparison of categorical variables.
We conducted logistic regression to evaluated adjusted odds ratios (aOR) for binary outcomes, adjusted for age, race, gender, BMI, education and income level, PHQ9 score, work pattern, exercise pattern and comorbidities. Restricted cubic splines were used to model the probability of opioids use according to BMI and PHQ9 score. We examined non-linear associations between BMI and PHQ9 score and the risk of opioids use non-parametrically with restricted cubic spline analyses. 17 In the cubic spline analysis, we used the BMI and PHQ9 score as the reference and four knots. All statistical analyses were conducted using SPSS software version 18 (IBM Corp., Armonk, NY, USA). We considered p value <.05 as statistical significance.
Results
Demographic characteristics of the American adults with or without osteoarthritis.

OA: osteoarthritis; BMI: body mass index.
The annual prevalence of each prescription analgesic medication was evaluated to show the trend of each prescription analgesic medication use. (Figure 1 and Figure S1) It was shown that the opioids use did not decrease as time goes by. We found the use of gabapentinoid increased rapidly from recent decade (From 5.0% to 12.1%), especially for male OA patients (From 3.8% to 15.2%, Figure S1). Trend of each prescription medication used by OA participants from 2007 to 2018. OA: osteoarthritis; COX-2: cyclooxygenase 2; NSAIDs: nonsteroidal anti-inflammatory drugs; SSRI: selective serotonin reuptake inhibitor.
Prescription medication use among the osteoarthritis participants.
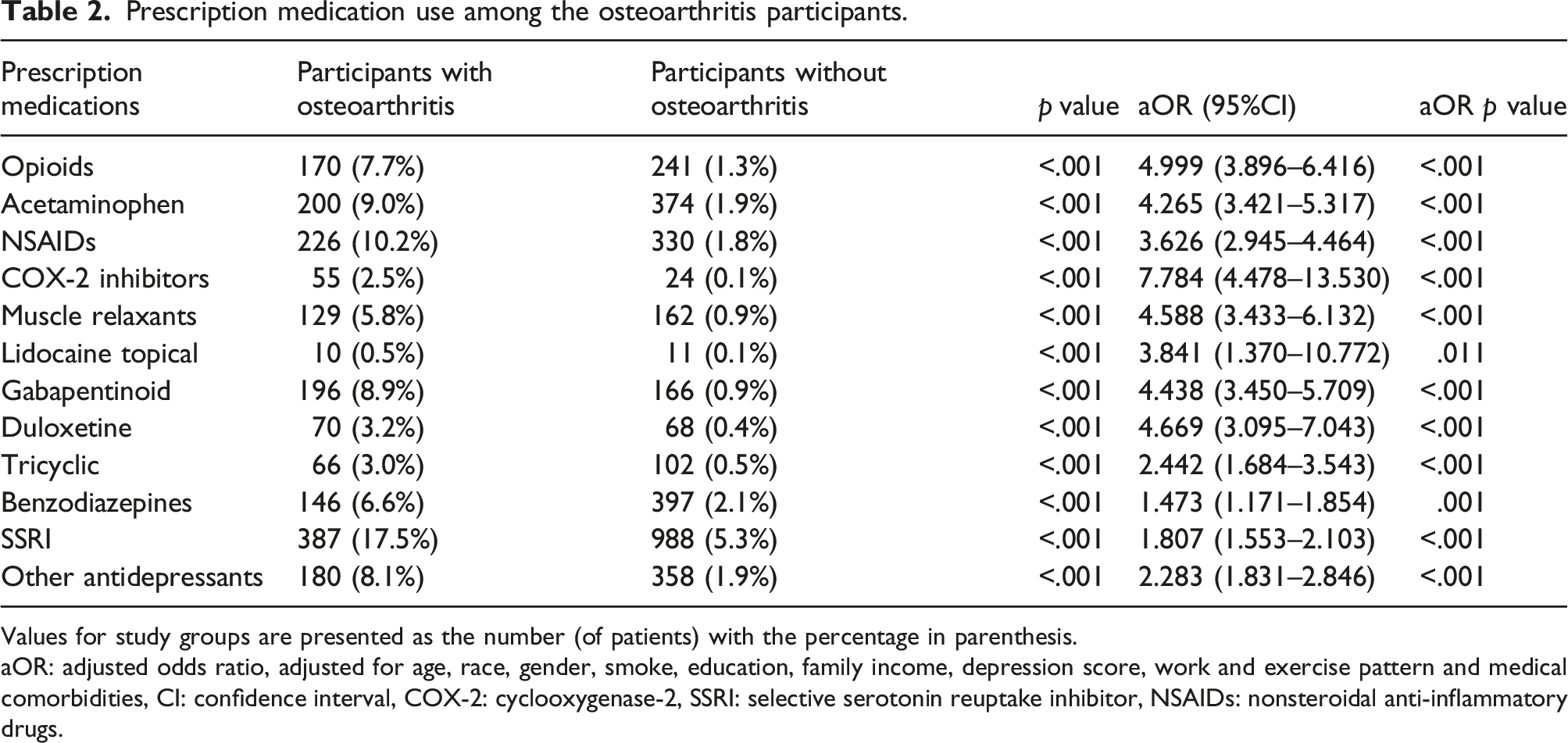
Values for study groups are presented as the number (of patients) with the percentage in parenthesis.
aOR: adjusted odds ratio, adjusted for age, race, gender, smoke, education, family income, depression score, work and exercise pattern and medical comorbidities, CI: confidence interval, COX-2: cyclooxygenase-2, SSRI: selective serotonin reuptake inhibitor, NSAIDs: nonsteroidal anti-inflammatory drugs.
Table S2 showed the median duration of each prescription analgesic medication use. The duration of opioids use was significantly longer in patients with OA (median duration 730 days) than patients without OA (median duration 182 days). For patients with OA, we also found the median duration of acetaminophen, NSAIDs and COX-2 inhibitors use was 1095, 730 and 1825 days, respectively.
We further analyze the frequency of various drug combinations used by OA population. (Figure 2) SSRIs, opioids, acetaminophen, NSAIDs, muscle relaxants and gabapentinoid were the common analgesics combined with other analgesics. The common analgesic combination used by OA population was opioids with acetaminophen and gabapentinoid with SSRIs (2.9% and 2.7%, respectively). Other common analgesic combinations could also be figured out, such as SSRIs with opioids (2.2%), acetaminophen (2.4%), NSAIDs (2.2%) or muscle relaxants (2.0%). Besides, acetaminophen was also commonly combined with gabapentinoid (1.9%) or muscle relaxants (1.8%) to reduce pain. Combinations of different medications used by OA participants. The most frequently co-administered medications are given in red and the least frequently co-administered medications are given in green. OA: osteoarthritis; COX-2: cyclooxygenase 2; NSAIDs: nonsteroidal anti-inflammatory drugs; SSRI selective serotonin reuptake inhibitor.
Adjusted odds ratio of demographic factors associated with medication use.

GED/AA: general educational development and associate’s degree (equivalent to high school diploma), REF: reference.
*p< .05; **p< .01.
The results suggested that patients with higher BMI, higher depression score, lower income level and more medical comorbidities were more likely to use opioids for pain relief. (Table 3) However, vigorous reaction exercise could inhibit the use of opioids (aOR: 0.343, 95% CI 0.160–0.734). Similarly, lower income participants were more likely to use acetaminophen, muscle relaxants and gabapentinoid. In addition, smoking was a risk factor for acetaminophen (aOR: 1.593, 95% CI 1.191–2.131) and gabapentinoid (aOR: 1.629, 95% CI 1.218–2.179) use. We also found that participants with vigorous work pattern were less likely to use muscle relaxants (aOR: 0.419, 95% CI 0.214–0.819) and gabapentinoid (aOR: 0.525, 95% CI 0.306–0.899) for pain relief.
The relationships between opioids use and BMI and PHQ9 score were analyzed by used restricted cubic splines models. The OR for opioids uses increased as the BMI and PHQ9 score increased. This suggests that the prevalence of opioids use increased as BMI (>27.5) and PHQ9 score (>3) increased. (Figure 3(a) and (b)). Adjusted cubic spline models showing association between BMI (a) and PHQ9 score (b) and the risk of opioids use. Models are adjusted for age, race, gender, smoke, education, family income, depression score, work and exercise pattern and medical comorbidities. The solid line and long dash line represent the estimated odds ratio and its 95% confidence interval. Knots are at the 25th, 50th, 75th and 95th percentiles for metabolic equivalents. PHQ9 patient health questionnaire nine score.
Discussion
The aim of our study was to analyze the trend and pattern of prescription analgesics use in American OA patients. In addition, we tried to show the demographic characteristics of opioid use among OA population which were benefit for managing the use of opioids. Recently, due to gabapentinoid was good at inhibiting the sensitization of pain, more and more concerns were paid into the use of gabapentinoid for the treatment of OA. 10 A previous study has pointed that gabapentinoid use gradually increased for patients with OA between 1995 and 2015 in England. 18 Similarly, our finding showed that the use of gabapentinoid increased rapidly from recent decade in America, especially for male patients. Previous studies showed that gabapentinoid prescriptions were striking increase all over the world.19–24 However, these studies were not specific to patients with OA while our results were representative for OA patients. A recently study pointed that OA patients were at higher risk of combination of gabapentinoid and opioids prescription. 25 This finding is partly consistent with our result. However, previous research reported that more than 85% of gabapentinoid-related deaths involved opioids. 26 This result demonstrated the risk of concomitant prescribing. So, stricter restrictions on the combination of gabapentinoid and opioids is needed.
Recent studies have pointed acetaminophen has poor analgesic effect in OA and largely unknown gastrointestinal and cardiovascular toxicity. 27 Therefore, we can find that acetaminophen use gradually decreased last decades. However, NSAIDs was also the most commonly used analgesic. Though NSAIDs are effective for OA pain control, but their side effects limit their use. So, further work is required to figure out how to decrease the gastrointestinal and cardiovascular risks related to NSAIDs.
Excessive use of opioid analgesics to treat musculoskeletal pain conditions was still a common and serious problem in America. 28 Although many professors and authorities have already appealed to reduce the use of opioids, the level of opioid use in the America remains high.29,30 Our results also supported this viewpoint, the use of opioids did not decrease in the past decade. Though the long-term pain-relieving effect of opioids for OA was not significant,31,32 our results showed the median duration of opioids in OA patients was very long.
Our study is consistent with that of Stokes et al. who reported that obesity is a risk factor for prescription opioids use among OA patients. 33 But in our present study, we further used the restricted cubic splines model to show the relationship between prescription opioids use and BMI. Interestingly, when BMI was 27.5, the risk of prescription opioids use was the lowest. While BMI higher than 27.5, the risk of prescription opioids use was gradually increased as patients getting heavier. Furthermore, we also pointed that the risk of prescription opioids was associated with depression degree (counted by PHQ9 scale). When depression degree aggravated, the risk of prescription opioids use was rising rapidly. This finding broadly supports the work of previous studies which pointed psychological states was significantly associated with the extent of opioid abuse.34,35 However, high quality evidence researches and recommendations based on psychological status assessment of OA treatment is lacking. 36 Therefore, it is possible that underestimated psychological factors might be a reason why OA patients show an extended use of opioids.
We also found patients with lower income level was more likely to use opioids, while education level was not a risk factor. For low-income patients, they usually believe that they are not prescribed enough pain medications, including opioids. 37 Another possible explanation for this is that doctors’ prescribing practices in low-income neighborhoods and low-income patients not questioning the appropriateness of prolonged opioid treatment. 38 However, this outcome was partly contrary to previous studies pointed that lower education level was a risk factor for opioids use.39,40 A possible explanation for this might be that previous studies were focus on low back pain and neck pain patients with lower average age. So, education level may play a nonsignificant role in older populations.
One unanticipated finding was that reaction exercise can significantly reduce the use of opioids and acetaminophen. This also accords with our earlier observations, which showed that exercise therapy could play a significant role in tapering or deprescription of opioids. 41 Another recent study indicated early physical therapy can reduce the frequency and level of opioid use for all musculoskeletal pain. 42 Above findings suggested that reducing prescription opioid use will require striker management for key populations and expanding access to nonpharmacologic therapies and nonopioid medications. The Osteoarthritis Research Society International (OARSI) recently released a guideline for managing OA, which do not recommend paracetamol and strongly recommend against opioids. 43 Therefore, future research should focus on nonpharmacologic therapies such as exercise therapy, physical therapy and cognitive behavioral therapy.
However, there are some limitations in our study. Firstly, our data was self-reported which may contribute measurement error and recall bias. Especially, opioid users are more likely to conceal their medication history which may lead the underestimate of opioids use. Secondly, specific dosage and frequency of each analgesic were unknown which inhibit the further exploration of the relationship between specific dosage and some demographic characteristics. Thirdly, it is not clear whether the analgesics were used for other unlicensed, painful conditions. Though we have excluded many conditions which may affect the use of analgesics, such as gout, cancer, fracture, rheumatoid arthritis, psoriatic arthritis, other arthritis, iritis/uveitis, ulcerative colitis, and Crohn’s disease to decrease this bias as far as possible. Fourthly, our research was conducted in America and thus findings may not be generalizable to other countries. The America has a long history of analgesics use and thereby accumulated a lot experience in management of analgesics. Nowadays, the demand for prescription analgesics is increased rapidly, and excessive use of analgesics is becoming a serious global problem. 44 Therefore, learning from the American experience is also important for other countries. 45 Finally, usage of non-oral drugs such as opioid path is not provided in the database, therefore we could not involve the non-oral drugs into our present study.
Conclusion
For OA patients, NSAIDs, acetaminophen and gabapentinoid were the mostly highly used analgesics, while SSRIs were the mostly used antidepressants drug. We also found that the opioids use was very common in OA patients and did not decrease from 2007 to 2018. In addition, the use of gabapentinoid increased rapidly from recent decade, especially for male patients. The duration of opioids, acetaminophen, NSAIDs and COX-2 inhibitors use was significantly long in patients with OA. Therefore, future research and clinicians should pay more attention on nonpharmacologic therapies. We also found that patients with higher BMI, higher depression score, lower income level and more medical comorbidities were more likely to use opioids for OA pain relief. The risk for opioids uses increased as the BMI and PHQ9 score (depression) increased. For these risk population, more striker management for pain should be recommended. Our results revealed the potential problems in pharmacotherapy choices for OA patients and may help improve and standardize the pain management.
Ethical statement
Ethical approval
All data were obtained from NHANES directly in deidentified form, and thus this study did not require additional Institutional Review Board approval.
Supplemental Material
Supplemental Material - Prescription analgesic medication use among osteoarthritis patients
Supplemental Material for Prescription analgesic medication use among osteoarthritis patients by Zhenzhen Huang, Xinxin Chen, Xihong Gan and Jiajia Chen in Journal of Orthopaedic Surgery.
Footnotes
Authors’ contributions
All authors make substantial contributions to conception, design, acquisition of data, and analysis and interpretation of data.
Declaration of conflicting of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.