
Abstract
Purpose
Polymethyl-methacrylate cement (PMMA) is often used as bone defect reconstruction material after surgical removal of giant cell tumors. The purpose of this study was to investigate if the application of PMMA improves the local recurrence rates for giant cell tumors (GCT) of appendicular bone treated with intralesional curettage.
Methods
A retrospective analysis of all appendicular GTCs treated at two major Danish sarcoma centres between the 1st of January 1998 and December 31st 2013; minimum follow-up of 3.0 years (median: 8.9; 1.3–18.7 years). Kaplan-Meier survival model, log-rank and multivariate Cox regression were used to calculate and compare local recurrence rates. p-values <0.05 were considered statistically significant.
Results
102 patients (M59/F43), median age 31Y (11–84) were included in this study. The overall 3-years local recurrence-rate was 19.9% (95%CI: 11.9–27.9%); 91% had occurred within 3 years. In patients treated with intralesional curettage (n = 64), the 3-years recurrence-rate was 30.6% (95%CI: 18.8–42.4%), compared to 2.6% (95%CI: 0.0–7.8%) in patients treated with wide resection or amputation (n = 38), p < .001. The 3-years recurrence-rate for patients treated with intralesional curettage and reconstruction using PMMA was 29.0% (95%CI: 12.6–45.4%) and without PMMA: 31.8% (95%CI: 15.2–48.4%), p = .83.
Conclusion
We found that the use of PMMA for bone defect reconstruction after intralesional curettage of GTCs in the appendicular skeleton did not ensure a reduced risk of local recurrence.
Keywords
Introduction
Giant cell tumors of bone (GCTs) are rare, predominantly benign tumors known for their high risk of local recurrence. GCTs are typically located in the epiphyseal bone in primarily young active patients and most frequently around the knee.1,2
Local recurrence rates up to 65% have been reported following simple intralesional curettage without adjuvant treatment. 3 Though other surgical approaches such as wide resection, en bloc - and segmental resection have been associated with low recurrnece rates of 0–12%, intralesional curettage remains the standard treatment for GCTs, as it allows for joint preservation in this tumor entity providing a better functional outcome for the patient.4,5 With the use of more extended curettage with high speed burring and employment of local adjuvants such as bone cement, liquid nitrogen, hydrogen peroxide, zinc chloride, phenol and cauterization with argon beam, recurrence rates between 10 and 20% has been reported.6,7 Today, wide bone resection is usually only considered when the joint is deemed unsalvageable although other variables such as tumor characteristics, the patients’ overall health status and surgeons’ preference might also affect the choice of the surgical treatment strategy.5,8
After intralesional curettage, the optimal technique for reconstruction of the residual bone defect is a matter of ongoing debate. Polymethyl-methacrylate (PMMA) bone cement is a popular option, advocated by many authors, as it provides immediate strong mechanical support to the often thin subchondral bone remnant beneath the adjacent articular surface and induces a potential tumor necrosis effect on potential residual tumor due to local heat generation associated with polymerization.9–11
PMMA precludes, on the other hand, remodelling to normal bone, which is why alternative options such as cancellous bone allograft are preferred for bone defect reconstruction in some sarcoma centres.3,10,12
Accordingly, there is still not consensus among surgeons regarding what type of local adjuvant should be used as filler in the tumor cavity after curettage. Our country, with two main sarcoma centres is a good example of this controversy. Historically, PMMA has been the preferred method for bone defect reconstruction following intralesional curettage of GCTs in one centre while cancellous bone allograft was preferred in the other centre. In this study we performed a retrospective analysis of all patients referred to both sarcoma centres to determine if PMMA reduces the local recurrence rate among this cohort. The main objective was to identify the effect of PMMA as a local adjuvant among patients treated with intralesional curettage for GCT of appendicular bone. Secondary objectives were to investigate if primary major bone resection (joint replacement surgery/local bone resection/amputation), age, sex, tumor location, pathological fracture, Campanacci Grading, unintended prior surgery, or neoadjuvant Denosumab could be identified as independent risk factors for local recurrence or confound the association between PMMA and recurrence rates.
Materials and methods
Data inclusion
This is a retrospective study of all patients who underwent primary surgical treatment for giant cell tumors of bone in the appendicular skeleton at the two major Danish orthopedic oncology centres between January 1st 1998 and December 31st 2013.
Demographic data on age, gender, histological diagnosis, tumor size and anatomical location of the bone lesions, details of the surgical procedure and local recurrence were collected from the medical records and the national pathology database. 13 From 2009, data were collected prospectively and reported in a national sarcoma database. 14 Patients with axial tumors, malignant transformation and recurrent tumors were excluded from this study. High-speed burring and adjuvant hydrogen peroxide was used occasionally, but not systematically documented and therefore not included as a variable in this study.
All tumors were graded according to the Campanacci classification system and size was measured as the largest diameter from the initial MRI-scan. 15 The choice of surgical procedure and material for defect filling was left at the discretion of the attending surgeon, however, as previously stated, PMMA was preferred at one centre, and never used in the other centre.
Statistics
We performed a Kaplan-Meier survival analysis to estimate the cumulative incidence function with a calculation of 95% confidence intervals (CI95%) for single-variable relations. Log-rank test and multiple Cox regression analysis were calculated using SPSS-software (version 27). Time to local recurrence was measured from the date of primary operation until the date when local recurrence was histologically verified. Variables chosen for the multiple Cox regression analysis among patients treated with intralesional curettage were: Patient age and gender, application of PMMA (yes/no), the presence of a pre-operative fracture, pre-operative treatment with Denosumab, Campanacci tumor grading, tumor location in a long bone and if unintended surgery was performed prior to referral to the sarcoma centre (Table 3).
Approvals
This study was approved by the Danish Data Protection Agency (J.no. 2013-41-2081) and the Department of Health Agency (J.no. 3-3013-725/1).
Results
Descriptive statistics: Patient and tumor characteristics
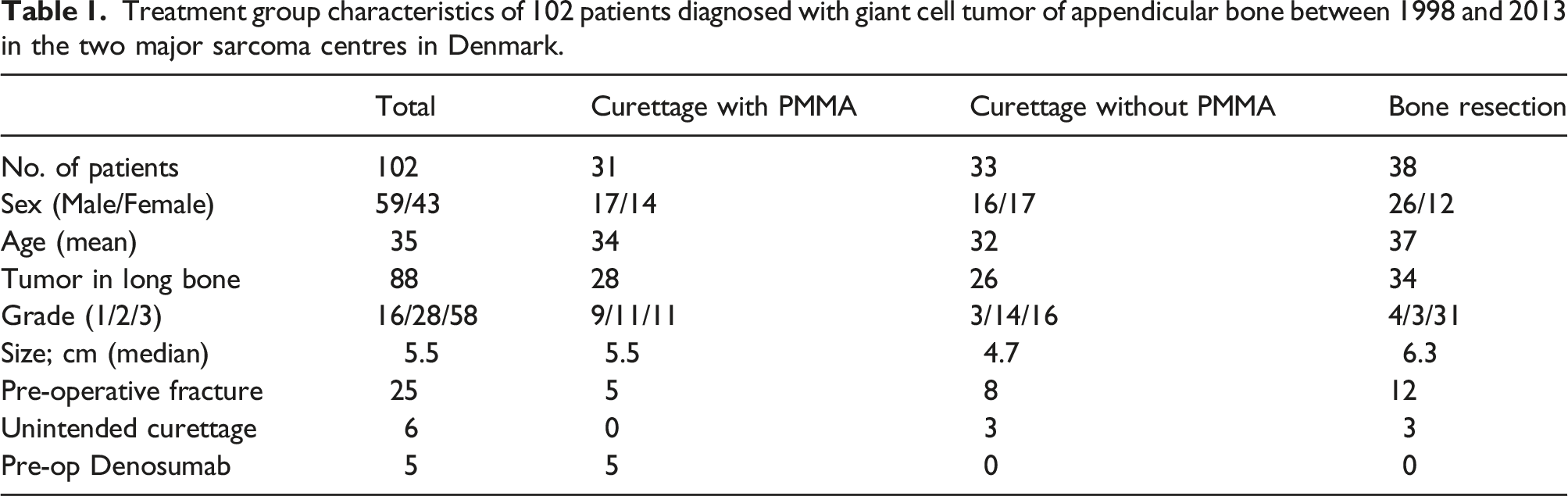
Treatment group characteristics of 102 patients diagnosed with giant cell tumor of appendicular bone between 1998 and 2013 in the two major sarcoma centres in Denmark.
Surgical intervention and recurrences of 102 patients diagnosed with giant cell tumor of appendicular bone between 1998 and 2013 in the two major sarcoma centres in Denmark.

Recurrence
In the entire cohort, 22 patients experienced local recurrence and most recurrences (n = 20/22, 91%) occurred within 3 years, resulting in 1-, 3- and 5-year probability of local recurrence of 11.9% (95%CI: 5.5–18.3%), 19.9% (95%CI: 11.9–27.9%) and 21.3% (95%CI: 13.1–29.5%), respectively (Figure 1(a)). Kaplan-Meier survival analysis of giant cell tumor recurrence in a Danish cohort of patients diagnosed between 1998 and 2013. (a) Overall recurrence rate (n = 102), (b) 3-years recurrence rate comparing patients treated with intralesional curettage with PMMA (n = 31) and without PMMA (n = 33), (c) 3-years recurrence rate comparing patients treated with intralesional curettage (n = 64) and resection (n = 38).
Twenty patients treated by intralesional curettage suffered a local recurrence of which 10 patients had received defect reconstruction with PMMA and 10 patients received defect reconstruction without PMMA (Table 2). When comparing the 3-year probability of local recurrence for patients treated with intralesional curettage and PMMA reconstruction (29.0% (95%CI: 12.6–45.4%)) and without PMMA reconstruction (31.8% (95%CI: 15.2–48.4%)), our main objective, we found no statistical difference, log-rank, p = .831 (Figure 1(b)).
Local recurrence occurred in only two of 38 cases of patients treated with primary bone resection: A soft tissue recurrence after 4.9 years and a malignant transformation after 1.2 years. The 3-year probability of local recurrence was significantly lower for patients treated with bone resection (2.6% (95%CI: 0.0–7.8%)) compared to intralesional treatment (30.6% (95%CI: 18.8–42.4%)), log-rank; p < .001 (Figure 1(c)).
Multiple Cox regression model among patients treated with intralesional curettage (n = 64), diagnosed at the two major sarcoma centres in Denmark between 1998 and 2013.

Discussion
In this retrospective study we investigated if the use of PMMA bone cement after intralesional curettage of appendicular giant cell tumors reduces the local recurrence rate. We were unable to show a statistically significant decrease in local recurrence rates when PMMA bone cement was applied. We found that bone resection (joint replacement surgery, local bone resection or amputation) compared to intralesional curettage was associated with a statistically significant lower risk of local recurrence. None of the variables, in the multiple Cox regression analysis of the cohort that was treated with intralesional curettage showed statistically significant associations with the risk of local recurrence.
In recent systematic reviews there is still no consensus on whether PMMA should be used systematically for bone defect reconstruction to reduce the recurrence rate after curettage of GCTs.3,5,11,16 The rationale for using PMMA is that it provides immediate mechanical stability and thereby allows the surgeon to be more aggressive in tumor removal. Further, PMMA is believed to provide a tumor toxic and necrotic effect that eliminates remaining active tumor cells. 12 However, PMMA might on the other hand induce thermal damage to surrounding tissue, increase the risk of infection and promote degenerative conditions in the surrounding bone due to stress shielding.5,7,11,17
Various combinations of medical and surgical techniques have been suggested to reduce the recurrence rates such as high-speed burring, hydrogen peroxide, phenol, and liquid nitrogen among others. However, none of them has been reported systematically as independent significant predictors for decreased LRRs.2,18
In two large retrospective multicentre studies, both in favor of PMMA as a local adjuvant it is noticeable that the reported local recurrence rates after curettage without PMMA are very high ranging from 49% up to 61%.9,19 These rates are not only high compared to our study (31.8%) but markedly higher than what has previously been reported (18%) among patients treated with intralesional curettage without the use of cement adjuvants. 20 These large differences in recurrence rates following similar treatments illustrate how confounding factors can have a substantial effect on the results and conclusions of studies on recurrence in giant cell tumors.
Studies evaluating the effect of PMMA typically report recurrence rates between 14 and 20% after intralesional curettage and defect reconstruction using PMMA although the recurrence rates up to 30% have been reported.9,12,21,22 These rates are lower than found in our study making it less likely that we would find a significant effect of PMMA. One possible confounding factor influencing our results is the use of the previously mentioned high-speed burring, which we have not systematically documented and therefore not included in our study. Very promising results have been shown using only high-speed burring as adjuvant treatment after intralesional curettage with recurrence rates between 12 and 23%. 23 The possibility of achieving very low recurrence rates without the use of chemical adjuvants suggests that thorough surgical tumor-removal might be the most important factor to avoid local recurrence. 4 In support a review of 387 patients treated with high-speed burring showed that the addition of PMMA and other adjuvants did not affect recurrence rates. 20
This is a retrospective analysis with a limited data set size. This is partly due to the rarity of the disease and to the fact that Denmark has a small population size of only approximately 6 Mio. people. Further, data is limited because high speed burring was not documented systematically. Hydrogen peroxide was occasionally used intraoperatively to flush the surgical cavity at one of the two sarcoma centres, but not documented systematically. We had no missing data points in the variables included in the analysis, due to the national patient journal system and national pathology database.
Conclusion
We found that wide resection of giant cell tumors of bone in the appendicular skeleton is associated with low recurrence rates compared to intralesional treatment and that the use of PMMA did not guarantee reduced recurrence rates. Does this mean that we do not recommend the use of PMMA? No. Instead, we argue it should be left to the discretion of the surgeon to outweigh potential risks and benefits in the specific case. We advocate not to compromise thorough tumor removal in the belief that PMMA will remove residual tumor cells. We suspect that the true effect of PMMA is yet to be uncovered and prospective randomized controlled studies are warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.