
Abstract
Background
Checkrein deformity, is a rare claw toe dynamic deformity of the hallux or great toe. This study investigated the use of diagnostic ultrasound in positioning the accurate injury location causing checkrein deformity and its clinical significance for etiological diagnosis and selection of surgical methods.
Methods
This retrospective study included patients with confirmed checkrein deformities (according to typical symptoms) at the Department of Traumatic Orthopedics of Tianjin Hospital (Tianjin, China) from March 2017 to July 2021.
Results
A total of 11 patients (8 males and 3 females) with a mean age of 36.7 ± 16.8 (range 19–61) were included in this study. The injuries included six cases of tibia and fibula fracture, one case of single tibia fracture, and one case of single fibula fracture. Four patients were treated with steel plate internal fixation, three patients with intramedullary nailing, and one patient with external fixation. Three patients reported no history of any high-energy trauma or surgery. The ultrasound results showed that seven patients suffered from flexor hallucis longus (FHL) lesions, two patients suffered from flexor digitorum longus (FDL) lesions, and two patients suffered from FHL and FDL lesions. The patients underwent different surgeries tailored to their specific lesions. Toe flexion deformity was completely corrected after operation in all patients. The function of the toes was recovered to varying extent.
Conclusion
The results of this study demonstrates that the checkrein deformities can be confirmed by ultrasound. It could be used to determine the adhesions before the operation, acting as guidance while establishing the surgical planning.

Introduction
Checkrein deformity, also described as the “fixed length phenomenon”, is a rare claw toe dynamic deformity of the hallux or great toe, due to the contracture of flexor hallucis longus (FHL) tendon in the posterior foot, proximal to the flexor retinaculum of the ankle.1,2 The condition was first described in 1974 by Clawson who observed it following a tibial fracture. 3 The deformity often occurs secondary to non-operative or surgical correction of fractures of the distal tibia and fibular. 4 In addition, it has also been reported following talar fracture, 5 calcaneus fractures, 6 subtalar dislocation, 7 removal of the fibula for bone graft 8 and soft tissue trauma with compartment syndrome. 1
The clinical presentation is a flexion contracture of the hallux interphalangeal (IP) joint with mild extension contracture of the metatarsophalangeal (MTP) joint, that worsens with passive dorsi-flexion of the ankle. 9 Many patients complain that their big toe is deformed, causing pain and making it difficult for them to walk. 10
Nowadays, there are no uniform methods of treatment. Some surgeons prefer to find out the reason for adhesion and perform tendolysis when taking out internal fixations,11,12 while others advocate direct tendolysis surgery.13,9 Although the tendon lengthening alone is helpful to improve deformities, toe flexion function may still be partially lost. If the deformities are caused by adhesion, the basic function of toes can be restored through in situ release. 14 No study on positioning injury location has been reported. The adhesion location mainly relies on the personal analysis from the orthopedic surgeons or the magnetic resonance imaging (MRI) and Computed Tomography (CT) examinations. On the one hand, different adhesions will present with the same clinical symptoms, which is difficult for doctors to judge. On the other hand, MRI or CT signals can be confusing in patients with severe injuries. Combined with the inability to perform dynamic observation, identifying the exact location of the adhesion in such cases is difficult. Thus, the accurate positioning of the injury sites and etiological diagnosis have guiding significance for selecting surgical methods.
Diagnostic ultrasound imaging (DUSI) has been used in medicine since the early 1950s. 15 In the following decades, DUSI became well-established in clinical obstetrics, gynaecology and cardiology. 16 In 1972, the first clinically significant application of DUSI was used in musculoskeletal medicine; where it was used to differentiate Baker’s cysts from thrombophlebitis. 17 This paper led to the logical extension of DUSI in musculoskeletal medicine seen today. The primary use of MSK-US continues to be used for traditional diagnostic imaging purposes, allowing real-time, dynamic evaluation of neuromusculoskeletal structures, including but not limited to joints, tendons, ligaments, muscles and nerves. 18
Therefore, this study aimed to investigate the use of diagnostic ultrasound in positioning the accurate injury location causing checkrein deformity and its clinical significance for etiological diagnosis and selection of surgical methods.
Methods
Study design and patients
This retrospective study included patients with confirmed checkrein deformities at the Department of Traumatic Orthopedics of Tianjin Hospital (Tianjin, China) from March 2017 to July 2021.
The inclusion criteria were (1) patient with confirmed checkrein deformities according to typical symptoms manifesting as tethering lesion of the FHL following hallux deformities (when the ankle was dorsiflexed, the toes are forced into extreme flexion; for ankle plantar flexion, the toes can be completely straightened), and (2) complete data. The exclusion criteria were (1) claw toes caused by foot lesions (fixed toe flexion deformities unrelated to the ankle joint movement), or (2) patients with systemic diseases including rheumatoid arthritis, renal failure, gout and diabetes, (3) patients had clinical acute lower-leg compartment syndrome and soft tissue infection.
This study was approved by the Ethics Committee of Tianjin Hospital. The requirement for patients’ informed consent was waived due to the retrospective nature of the study.
Ultrasound equipment and examination
Ultrasound examinations were performed using GE LOGIQ E9 ultrasound device (GE Healthcare, Milwaukee, WI, USA) with 9 MHz or15 MHz linear transducer (type 9L or ML6-15) by a radiologist with more than 5 years of experience in musculoskeletal ultrasound examination, who was blinded to the clinical and MRI reports.
The examination probe with appropriate frequency was selected according to the location and depth (the 9L probe was used for the lesion with deep position and the ML6-15 probe was used for the lesion with superficial position). The FHL and the adjacent flexor digitorum longus (FDL) muscles should be examined from origin to insertion. The morphological feature, echo intensity and muscle fiber clarity were systematically evaluated. Every region should be examined in longitudinal and transverse planes. Dynamic examination under active and passive stress can be used to assess function and motion range of the muscles. Bilateral contrast scanning was helpful to quickly identify muscle abnormalities.
Data collection and definition
The patients’ demographic characteristics and clinical data including age, sex, a summary of injuries, interval between injury and checkrein deformity diagnosis, results of ultrasound testing, lesion sites, surgical methods, and injury classification were collected. The lesion sites included the FHL and FDL tendon.
The injuries were classified into three types according to the characteristics of the injury cases in a previous study 19 and this study. Type I was caused by the adhesion of tendon or muscle-tendon transition to the surrounding tissues or bony callus, leading to the imbalance that proximal muscles were not involved in any activities while only tendons below this point were involved in flexion activities, resulting in insufficient tendon length between the point and hallux. This type of deformity was mainly caused by adhesion only with muscle injuries in adhesive sites. The proximal muscles are roughly normal. Type II was caused by contracture of the muscle belly. The tendons were normal. The shortened muscle belly could not be stretched out with movements, resulting in an insufficient length of muscle tendons. Type III was caused by a mixed combination of types I and II. The ultrasound results were used to confirm the injuries to the FHL and FDL.
Results
Characteristics of the patients and surgeries.
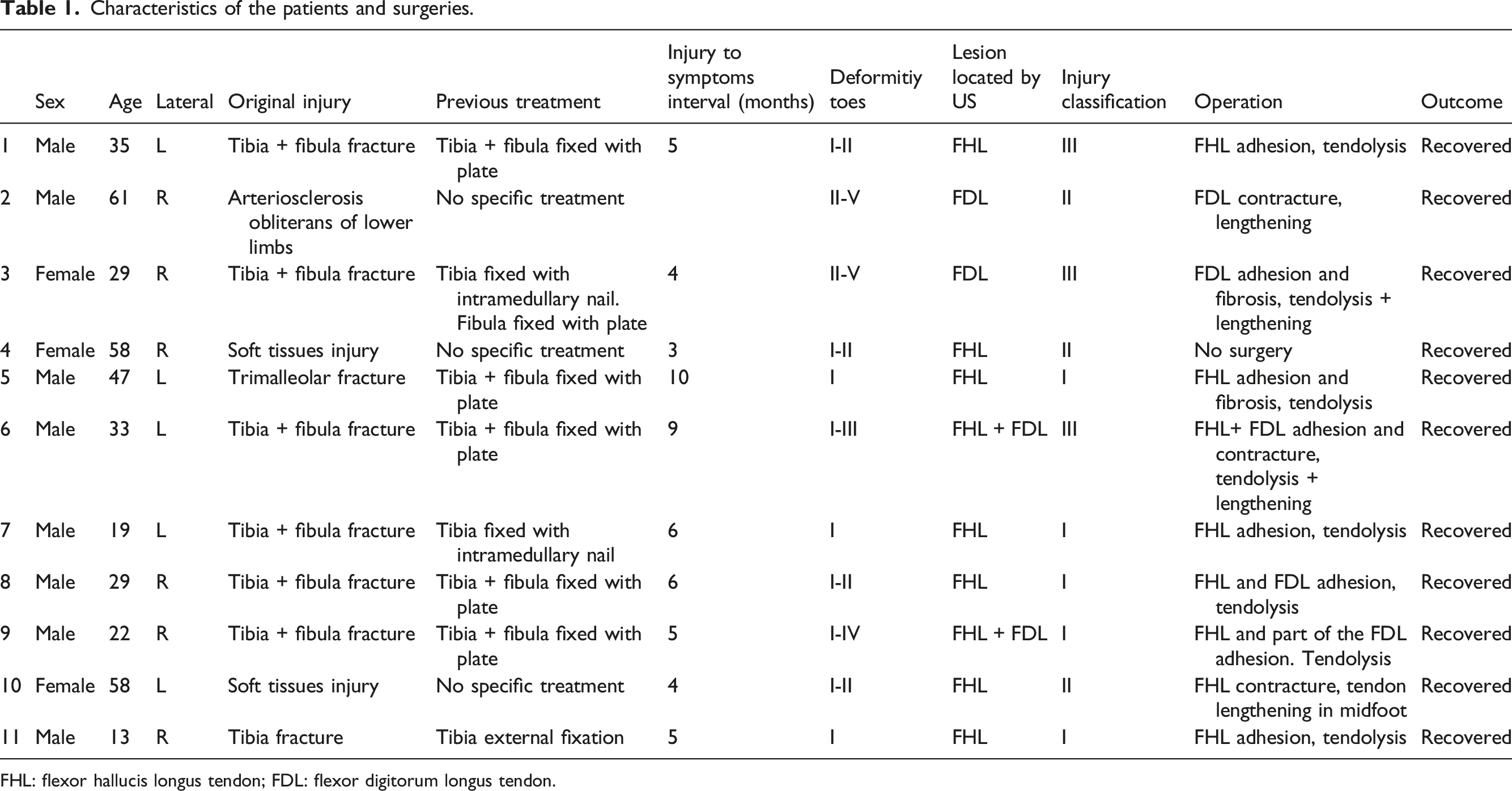
FHL: flexor hallucis longus tendon; FDL: flexor digitorum longus tendon.
The normal muscle shape was regular and the epimysium was smooth and continuous. The muscle fibers were hyporeflective and the connective areolar tissue that invests groups of muscle fibers within a muscle was hyperreflective. The perimysium was clearly seen as linear bands within the muscle belly on longitudinal images and as dots and bands on transverse section. The tendons were high reflectivity fibrillar structures appearing as multiple high reflectivity stripes on longitudinal images. The injured muscle becomes thin or uneven. Muscle belly appeared heterogeneous hypoechoic and muscle fiber’s structure were vague. Dynamic ultrasound showed muscle stiffness and reduced amplitude of motion. The hypoechoic tendon injury mainly involved the transitional part of the muscle and tendon. There was no significant injury to the distal tendon in this study. The fractured tibial or fibula showed irregular high echogenic processes instead of the smoothly bony surface, even near the internal fixation. FHL arises from the inferior two-thirds of the posterior surface of the fibula and interosseous membrane, and it inserts into the plantar surface of the great toe distal phalanx. 20 As FHL went close to the medial malleolus, restrictive adhesion of the FHL tendon by bone callus could be seen in some cases and the adhesion was almost located at the distal end of the tibia.
All patients were diagnosed by ultrasound, the results showed that seven patients suffered from FHL lesions, two patients suffered from FDL lesions, and two patients suffered from FHL and FDL lesions. And the injures were classified as follows: type I: 5 cases, type II: 3 cases, type III: 3 cases. Different surgical methods were adopted according to the specific lesions. Tenolysis was performed in 6 cases, tendon lengthening in 2 cases, and tenolysis plus lengthening in 2 cases (Table 1). After tenolysis, the toes should be moved immediately after the anesthesia disappears to prevent tendon adhesion again. After tendon lengthening, external fixation with a cast or brace was required for 3 weeks. After 3 weeks, the toes gradually began to move, and after 4 weeks, the toes gradually began to bear weight. The rehabilitation after tendon tenolysis and lengthening was the same as tendon lengthening. The toes flexion deformity was completely corrected after surgery in all patients. The function of the toes was recovered to varying extent. Patients were able to walk and normally squat without any serious impact on their quality of life. No obvious relapse was reported in the follow-up visits after the operation (5.8 ± 1.3 months). Compared with the surgical findings, the ultrasonic diagnosis was accurate, and the positioning diagnosis was completely correct in all cases.
Typical case
Case 6
Male, 33 years old, tibia and fibula fracture caused by a car accident. Sixteen months after surgery, he came to the hospital to treat a toe flexion deformity since it affected his daily walking. Ultrasound results indicated the muscle tendon transition of FHL was thickened, hypoechoic echo pattern, and adhesion to bony callus with a strongly echo-reflective structure protruded on the surface of the distal tibia (Figure 1). Adhesion was the main cause of the deformity. Besides that, there was diffuse hypoechoic in the proximal muscle belly, the muscle fiber’s structure was vague. The injury was classified as Type III (mixed causes). The deformities were corrected by release of adhesions and Z-plasty lengthening of the FHL and FDL tendons at the fracture site. After the operation, the toe flexion was corrected. The patient could walk normally. (a) Ultrasound image of the patient, showing the adhesion of the flexor hallucis longus tendon transfer with injured muscle belly to bony callus. (b) A flexion deformity of the left toe could be observed, while the right toes were normal. (c)The toe could completely stretch during plantar flexion of the ankle joint when he was sitting in the bed. (d)The appearance of the patient’s lower leg. Several scars could be seen on the skin.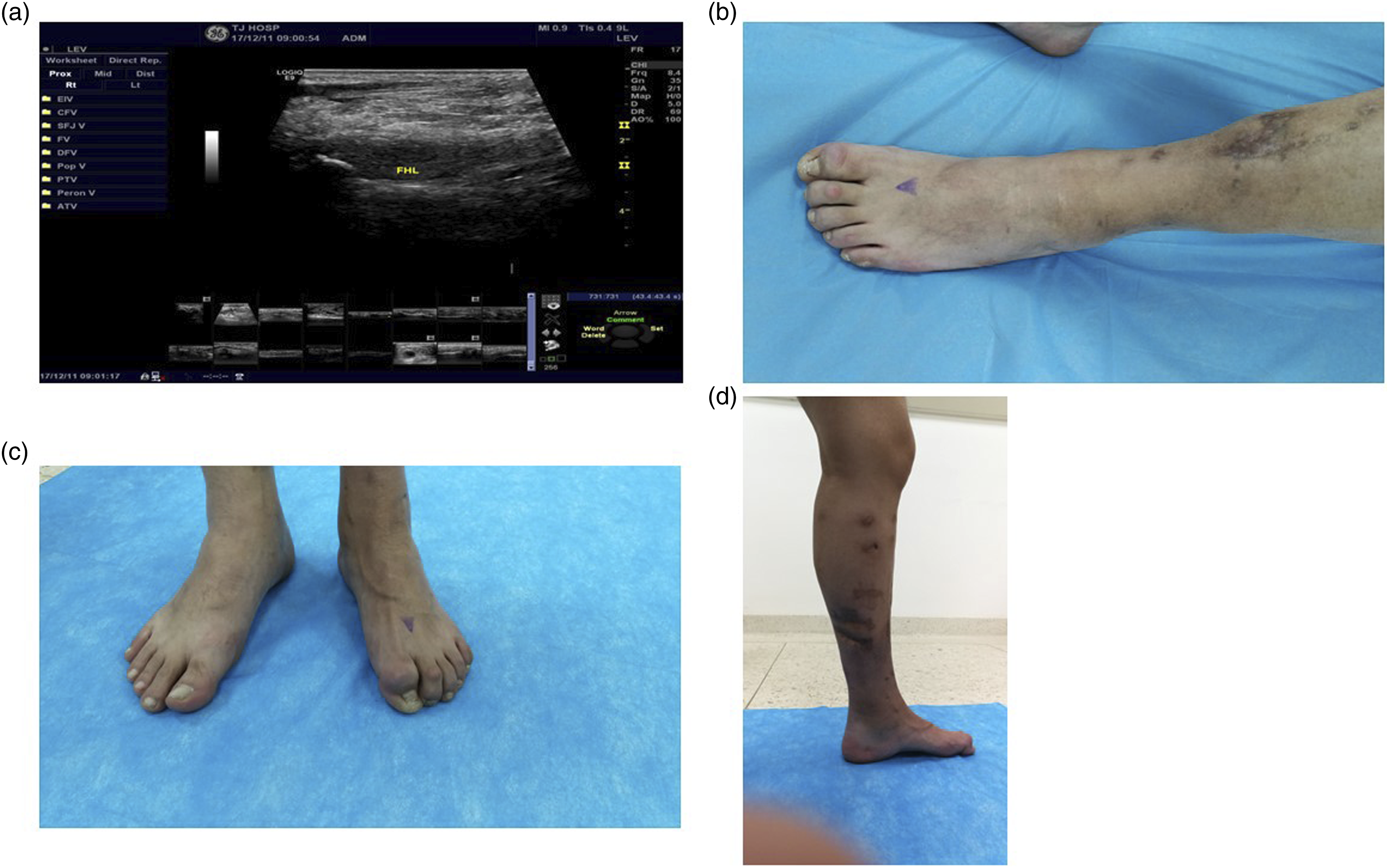
Case 10
Female, 58 years old. Falling from her bicycle caused swelling and bruising in her left lower leg, but there was no fracture on X-ray image. She gradually recovered. Four months later, flexion deformities of the hallux and second toe were observed. The cause may be subclinical compartment syndrome. Ultrasound showed that there was no abnormality in the FHL tendon. No signs of adhesion were found in passive motion. The partial muscle belly of the FHL was streak-like with a hypoechoic echo pattern (Figure 2). It was stiff and fixed in dynamic motion without any capacity of being stretched. All indicated that the deformities were caused by the relative shortening of tendons resulting from cicatricial contracture of the muscle belly. It was a type II injury. The injury location could be seen in the MRI since the patient had no history of surgery and was not treated with internal fixation and her injury was quite simple. The deformity resolved after z-plasty lengthening of the FHL tendon in the midfoot. (a) The muscle belly of the flexor hallucis longus tendon (FHL) was scarred with a hypoechoic echo pattern. It was stiff in dynamic motion without any capacity for stretching. (b) The streak-like low signal area of the FHL was consistent with the ultrasound results. (c) The patient could stretch out her toes when plantar flexion of both ankles. (d) The deformity of the left toe flexion was observed while the patient dorsiflexed her ankle joints.
Discussion
Checkrein deformities are rare and involve entrapment or fixed tethering of the flexor hallucis longus and, occasionally, flexor digitorum longus tendons. It is seen as a dynamic flexion deformity of the hallux characterized by flexion contracture of the interphalangeal joint and extension contracture of the metatarsophalangeal joint, worsened by ankle dorsiflexion. When the ankle plantar flexes, the deformity is corrected completely. Deformity is mostly secondary to FHL tendon entrapment after trauma with tibial, leg or ankle fracture, regardless of the internal fixation device used. 21 Because the FHL tendon has some interconnection to the tendons of FDL, deformities of the lesser toes are sometimes seen. An average time of onset of deformity with respect to the initial trauma is difficult to calculate from the data available in the literature, ranging from a few days after the trauma up to 60 months. 8
Diagnostic ultrasound is a common imaging modality used to assist in the diagnosis of musculoskeletal complaints when the clinical picture is uncertain. 22 MRI is often used to assess soft tissue injuries. However, when serious muscle and tendon injuries occur in the calf, there will often occur soft tissue structural disorder, limited or extensive scar tissue and muscle adipose after treatment. On the other hand, in some patients, due to artifacts of metal internal fixation and other reasons, MRI is difficult to display clearly, resulting in contracture, adhesion and fixation after injury of FHL and FDL. The major advantage of ultrasound over MRI, X-ray, or computed tomography (CT) is its ability to examine the tendons at rest and in dynamic extension and flexion, providing a better assessment of the adhesions or the contracture state of the muscle. 23 The real-time dynamic ultrasound examination can detect injuries in active motion and makes it possible to observe the dynamic movement of tendons by passive movement of patients’ toes with the assistance of the examiners. In this way, the location and cause of adhesion, together with the adhesion area, can be accurately determined. Meanwhile, the echo in muscle tendons can be used as indicators to decide whether there are any tendon injuries and the scope and severity of cicatricial contracture. Patients with any other toe deformities could be checked whether there is any injury in FDL and tendons. In addition, movements are not allowed in MRI examinations. It has limited value in the study checkrein deformity due to the impact of internal metal fixation. Ultrasound is different from MRI and is not affected by metal artifacts. Thus, it is an alternative to MRI and effectively assesses the soft tissue in the injury area.
The present study suggests that the checkrein deformities can be accurately confirmed by ultrasound. It could be used to determine the adhesions before the operation, acting as guidance while laying down the surgical planning. Ultrasound diagnosis in the present study, 9 cases were confirmed by surgery and 2 cases by MRI. In the 2 cases, one did not receive any surgical treatment, the other was performed with FHL tendon lengthening in the midfoot after confirming that the deformity was caused by muscle contracture through ultrasound. Since the surgery was not performed at the injury site, the muscle contracture was not confirmed in operation. Because the toes’ function recovered well after operation, it was indirectly confirmed that the injured site was located in the lower leg. Still, the two cases were not severe and did not have an internal metal fixation. They underwent MRI before the operation, and the results were consistent with the ultrasound. In addition, another one had underwent MRI in the 9 cases. No diagnostic information was obtained due to the muscle disorder and metal artifact.
Although the causes for checkrein deformity might involve tendons tethering or muscle contracture, the fact that the two causes can happen at the same time when the injuries are severe was neglected in the literature. 19 By ultrasound, we could find that the absolute shortening caused by contracture of the muscle belly and tendon fixation caused by adhesion of tendons could co-exist. The literature about the management of checkrein deformity is mainly reports of one to three cases. 24 These reports highlight the use of a specific surgical method in a specific patient, suggesting that surgical management of checkrein deformity should be tailored to each case, as advocated by the present study.
Because of the rarity of this deformity, no single surgical technique has been defined as the standard. In the present series of 11 patients, 10 patients achieved satisfactory outcomes after surgery, without recurrence or complications. It is supported by a series of eight patients who underwent a Z-plasty of the FHL. 9 Operation of hardware removal and tendolysis can be performed simultaneously on the patients who have requirements for internal fixation. Locating the injury area before the operation is helpful to determine the area on which tendolysis should be performed. For the patients without any requirements for internal fixation, the causes of the deformities can be classified through an accurate assessment by ultrasound. For type I, whether the in situ release is possible can be assessed, and a more minimally invasive treatment can be selected compared to tendon lengthening. For types II and III, which are caused by contracture of the muscle belly, tendolysis alone is ineffective. Such cases should be considered for tendon lengthening to reduce the frequency of unnecessary probing into the injuries of proximal muscle, thus reducing iatrogenic damage to the patients. With some experience gained from the series of cases, we recommend preoperative dynamic ultrasound examination, and select specific surgical methods according to the classification of injuries.
The present study has limitations that should be considered. On one hand, due to the rarity of the condition, only a small number of patients could be included. A higher level of evidence and a larger sample size should be provided. On the other hand, ultrasound examination is highly operator-dependent, thus requires experienced doctors with rich knowledge of musculoskeletal ultrasonography to perform assessment in the static and dynamic state.
Conclusion
This study demonstrates that checkrein deformities can be confirmed by ultrasound. It can be used to determine the adhesions before the operation, acting as guidance while establishing the surgical planning.
Footnotes
Acknowledgments
The author thanked the Ethics Committee of Tianjin Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethics Committee of Tianjin Hospital (No. EIC2022217).