
Abstract
The distal tibiofibular syndesmosis (DTFS) is more frequently injured than previously thought. Early diagnosis and appropriate treatment is essential to avoid long term complications like chronic instability, early osteoarthritis and residual pain. Management of these injuries require a complete understanding of the anatomy of DTFS, and the role played by the ligaments stabilizing the DTFS and ankle. High index of suspicion, appreciating the areas of focal tenderness and utilizing the provocative maneuvers help in early diagnosis. In pure ligamentous injuries radiographs with stress of weight bearing help to detect subtle instability. If these images are inconclusive, then further imaging with MRI, CT scan, stress examination under anesthesia, and arthroscopic examination facilitate diagnosis. An injury to syndesmosis frequently accompanies rotational fractures and all ankle fractures need to be stressed intra-operatively under fluoroscopy after fixation of the osseous components to detect syndesmotic instability. Non-operative treatment is appropriate for stable injuries. Unstable injuries should be treated operatively. Anatomic reduction of the syndesmosis is critical, and currently both trans-syndesmotic screws and suture button fixation are commonly used for syndesmotic stabilization. Chronic syndesmotic instability (CSI) requires debridement of syndesmosis, restoration of ankle mortise with or without syndesmotic stabilization. Arthrodesis of ankle is used a last resort in the presence of significant ankle arthritis. This article reviews anatomy and biomechanics of the syndesmosis, the mechanism of pure ligamentous injury and injury associated with ankle fractures, clinical, radiological and arthroscopic diagnosis and surgical treatment.
Introduction
The distal tibiofibular syndesmosis (DTFS) is stabilized by the ligaments that confer dynamic stability to the ankle. 1 This stability is essential for the integrity of the ankle mortise during weight bearing and walking. Once there is diastasis of DTFS the integrity of the ankle is compromised. 2 Injuries to the DTFS are more frequent than previously thought. Injuries of the syndesmotic ligaments may occur either in isolation or with an associated ankle fracture. Previously these injuries were expected to represent 1%–18% of ligamentous injuries of the ankle3,4 however recent studies have shown its incidence is in the range of 17%–74% of all sports injuries of the ankle.5,6 In this review article, we intend to review the current knowledge about clinico-radiological diagnosis and management of this complex injury.
Anatomy
The DTFS is a fibrous joint between the distal tibial concave incisura and the convex distal fibular surface. The anatomy of the syndesmosis is variable in terms of depth and version of the tibial incisura, which predisposes to inaccurate reduction as well as inaccurate assessment of reduction while treating these injuries.7,8 The precise relationship between the distal tibia and fibula is maintained by syndesmotic ligaments. (Figure 1) Based on a systematic review of cadaveric studies the syndesmotic ligaments include the Anterior inferior tibiofibular ligament (AITFL), Posterior inferior tibiofibular ligament (PITFL), Inferior transverse tibiofibular ligament (ITTFL), Interosseous tibiofibular ligament (IOL).
9
Anatomy of distal tibiofibular syndesmosis (IOL- Intraosseous ligament/membrane, AITFL- Anteroinferior tibiofibular ligament, PITFL-Posteroinferior tibiofibular ligament).
AITFL originates from the anterolateral tubercle of the tibia (Chaput tubercle) and attaches to the anterior tubercle of the fibula (Wagstaffe tubercle). This ligament has three bands, superior, middle, and inferior band that is separated by 2-mm wide gaps and runs obliquely in the lateral and distal direction. 10 In addition, some patients have an accessory inferior part of AITFL or Bassett’s ligament. 11 PITFL runs horizontally from the posterior malleolus to attach along the posterior tubercle of the fibula on the lateral malleolus. It has an upper superficial part and a lower deep part. The inferior part referred to as ITTFL is stronger and runs more horizontally. 10 The interosseous membrane is located between the tibia and fibula and spans nearly the entire lower leg. The interosseous ligament (IOL) is found in the distal 1 cm of the lower leg and is contiguous with the interosseous membrane. It originates approximately 5 cm proximal to the tibial plafond and runs disto-laterally to the fibular attachment which is 7 cm proximal to the tip of the lateral malleolus.11,12 The syndesmosis joint bears loads in the coronal, axial and rotational planes. 13 IOL functions as a shock absorber during the heel strike phase of gait (first rocker) and prevents separation of the medial malleolus and lateral malleolus beyond normal limits during full contact with the floor (second rocker). 14 In the axial plane the three ligaments (AITFL, PITFL, and Interosseous talofibular ligament) are responsible for maintaining a correct reduction of the incisura fibularis while adapting to rotational moments. 13 AITFL gets stressed during dorsiflexion and external rotation stresses and is responsible for 24% of syndesmotic resistance to this mechanism of injury, and superficial PITFL is an important stabilizing structure when an internal rotational force is applied from the fibula. 15 PITFL prevents posterior fibular translation, and ITTFL limits posterior talar displacement. 16 In a systematic review of cadaveric studies, it is found that IOL is the strongest syndesmotic ligament, and the AITFL has a dominant role in stabilizing the DTFS to external rotation force and therefore external rotation stress test is the most sensitive test to recognize an AITFL tear. 17 In a biomechanical study, it was found that the AITFL provided 35%, the transverse tibiofibular ligament or deep portion of the PITFL 33%, the IOL 22%, and the PITFL 9% of the overall stability. 18 In a cadaveric study evaluating ligamentous structures of the syndesmosis it was found that a diastasis of 2.3 mm occurred with sectioning of the AITFL alone, 5.5 mm with additional sectioning of the IOL, and 7.3 mm after additional sectioning of the PITFL. 19 In an arthroscopic evaluation done in a cadaveric study, syndesmotic instability was insignificant after transection of a single ligament (AITFL or PITFL) or after IOL was additionally transected. Sectioning of all syndesmotic ligaments led to significant diastasis at the posterior margin of the incisura, and diastasis became apparent at the anterior margin only when the deltoid ligament (DL) was additionally disrupted. 20
Although DL is not a true component of syndesmosis it provides stability to syndesmosis by limiting external rotation. Concomitant injury to DL has been reported in approximately 50% of patients with syndesmotic injury. 21 A cadaveric study demonstrated that deltoid sectioning did not destabilize the syndesmosis until AITFL and IOL were both released. 15 The DL has the function of preventing talar abduction, pronation and external rotation. Syndesmotic lesions with associated damage of the DL produce a still greater instability of the talus. 22
Clinical presentation
Almost 13% of ankle fractures 23 and between 18% and 20% of ankle sprains diagnoses 24 are associated with syndesmotic injuries (SI). Non-fracture-related ligamentous injuries can occur due to ankle twisting injuries, trip and fall accidents, fall from height, and running on uneven surfaces, but most of the pure ligamentous SI are sports-related. SI are more common in sports that have high-speed collisions, artificial surfaces, uneven terrain, and high-torque cutting and jumping forces that can result in dorsiflexion and external rotation of the foot relative to the ankle and tibia (eg. football, soccer, basketball, rugby, skiing, hockey).24–26 SI commonly occur during contact sports, which involve lateral movements and may be related to external foot constraint.27–29
Acute injuries to the syndesmosis can occur as a result of different mechanisms which include external rotation, hyperdorsiflexion, eversion, inversion, plantar flexion, pronation and internal rotation. 30 External rotation and hyper dorsiflexion is the most common mechanism responsible for syndesmotic injury.24,31 Mait et al., did a cadaveric study in which an external rotation force was applied to specimens in dorsiflexion, neutral, and plantar flexion. They found that syndesmotic injury occurred in 100% of the dorsiflexion group, 50% in the neutral group, and 0% in the plantarflexion group. In addition, the deltoid ligaments superficial and deep were injured to varying degrees in all specimens with noted syndesmotic injury. 32 External rotation forces the talus to rotate laterally thus pushing the fibula externally away from the tibia. This abnormal motion tears AITFL, PITFL, ITTFL, or a combination of these. 33 These twisting forces can also tear the IOL or interosseous membrane or even fracture the proximal fibula. 34 During hyper dorsiflexion, a wider portion of the talus pushes or wedges the malleoli apart, and the excessive force can sprain or even rupture AITFL and PITFL.35,36
Approximately 10% of ankle fractures are associated with SI and this percentage doubles in fractures requiring internal fixation. 37 Syndesmotic stability is most commonly compromised in pronation external rotation injuries (PER) followed by supination external rotation (SER) injuries according to Lauge-Hansen classification.38–40 Non-fracture-related syndesmotic ankle injuries are to be distinguished from other varieties of ankle ligamentous injuries based on the history, mode and mechanism of injury and physical examination. Some SI are obvious, but many are subtle and require due diligence to diagnose the injury accurately. In a recent study, the diagnosis of acute syndesmotic injury was missed in 49 ± 22% of the cases during the initial clinical examination. 41
As in most injuries, careful history-taking and physical examination are very important to arrive at a correct diagnosis and therefore an effective treatment. Patients with acute syndesmotic injury without ankle fractures, present with pain, swelling and ecchymosis over the syndesmosis area, and in severe injuries inability to bear partial or full weight is present. In subtle injuries, the swelling may be minimal. 42 Palpation is helpful as a syndesmosis injury is typically tender at the anterolateral joint line and proximal compared with a typical sprain which is over the distal fibula. A comprehensive ankle examination should be done to avoid missing concomitant injury to other ankle structures. 43
Tenderness to palpation at the level of the joint and the distance the pain extends proximally has been termed the “tenderness length”. The presence of “high ankle pain and tenderness,” more proximally, is suggestive of a more significant injury. 44 In fact, it has been shown that there is a significant correlation between how far this tenderness radiates proximally in the leg and the severity of the injury and consequently, the time to return to sports.44,45 Chronic syndesmotic rupture or malreduction must be suspected when persistent pain and tenderness are present in the syndesmotic area after an ankle injury. Chronic syndesmotic injury presentation may be due to missed syndesmotic ligament injury, loss of syndesmotic fixation before adequate healing, malreduction at the time of treatment, or malunion of ankle fractures. 46 When syndesmotic injury, whether acute or chronic is suspected the patient is subjected to special provocative tests which help to confirm the diagnosis.
Numerous special tests (Figure 2) have been described to detect syndesmotic injury. In Frick
47
’s test, passive external rotation of the foot in a neutral position against the fixed lower leg produces pain over the syndesmosis. Compression of the tibia to the fibula above the mid-point of the calf provokes pain at the DTFS level in the squeeze test.
48
Crossed-leg test is performed by asking the patient to rest the mid tibia of the injured leg on the opposite knee and produce a gentle downward force on the medial side of the knee of the injured side.
49
The fibular translation test is performed by stabilizing the tibiotalar joint with one hand and translating the fibula anteriorly and posteriorly with the other hand. Pain and increased translation relative to the uninjured side indicate a positive test.
27
The Cotton test is performed by translating the talus medial to lateral within the ankle mortise to elicit pain or appreciate the increased translation.
27
In a functional ‘‘stabilization test’’ an athletic tape is applied tightly above the ankle joint and the patient is asked to stand, walk, and perform a toe raise and jump. The test is positive when patients can stand, walk, and perform a toe raise and jump with lesser pain after taping.
11
Single leg hop test is done by performing a single leg hop by the toes and the test is positive when the patient is unable to hop.
44
In Lunge and twist test patient is asked to semi-squat while bearing weight and rotate the upper body, which produces pain in the syndesmotic area.
31
In the dorsiflexion compression test, the patient is asked to do extreme dorsiflexion of the affected ankle while bearing weight on both legs. If this manoeuver is painful the patient returns to a normal standing position, and the same manoeuver is again performed while compressing malleoli with both hands. A decrease in pain is suggestive of syndesmotic injury.
50
However, a systematic review of 8 different tests reported a low diagnostic accuracy of these tests and the authors concluded that no single test is sufficiently accurate for diagnosis and recommended a combination of tests.
31
The same authors performed another cross-sectional diagnostic accuracy study and found the squeeze test to have the highest specificity of 88%, whereas the syndesmosis ligament tenderness and external rotation stress test had the highest sensitivities of 92% and 71%, respectively.
51
Clinical photographs showing the physical examination manoeuvres: (a), Crossed-leg Test; (b), Tenderness Length; (c), Fibular translation test; (d), Tibiofibular squeeze test; (e), External rotation stress test; (f), Stabilization Tape test; (g), Single leg hop test; and (h), Dorsiflexion compression test.
In case the history and clinical examination suggest a syndesmotic injury, the patient needs to be subjected to further evaluation for confirmation of the diagnosis and to assess the severity of the injury.
Investigations
The radiographic imaging starts with three views of the ankle: anteroposterior (AP); mortise; and lateral. If there is a clinical suspicion of a Maisonneuve fracture, full-length radiographs of the lower leg are indicated. These radiographs are used to assess the relationship between the tibia and fibula and notice malleolar fractures and bony avulsions of the anterior or posterior fibula which are present in up to 50% of SI.
52
Increased tibiofibular space, the distance between the medial border of the fibula and the lateral border of the posterior tibia at the incisura approximately 1 cm proximal to the joint line, decreased tibiofibular overlap, the overlap of the lateral malleolus and anterior tibial tubercle, and increased medial clear space has been identified as syndesmotic indicators.53–55 (Figure 3) When using these parameters, comparison with the contralateral side is recommended, and tibiofibular clear space measured on the mortise view is the most accurate parameter when using a comparison contralateral radiograph.56,57 It has been shown that tibiofibular clear space and tibiofibular overlap fail to detect sagittal malreduction.
58
Because syndesmotic landmarks on AP and mortise views are not fully reliable, lateral fluoroscopic views have been recommended to evaluate syndesmotic injuries. In a study, on perfect lateral radiograph, the position of the fibula in relation to the tibia has been used to identify syndesmotic disruption, and anterior displacement was more reliably identified than posterior displacement (positive predictive value (PPV) 90% and 77%, respectively, for the ipsilateral images; 90% and 71%, respectively, for the contralateral images).
59
In another study lateral radiograph was used to record two measures, anterior fibular line ratio and posterior fibular distance, which were found to be useful adjuncts in the assessment of syndesmotic reduction.
60
Antero-posterior tibiofibular ratio, which assesses where the anterior fibular cortex intersects the tibial physical scar, has also been recommended to assess syndesmotic malreduction.
61
In a study to assess the diagnostic utility of different x-ray radiological methods for diagnosing syndesmotic reduction, it was found that tibiofibular clear space and tibiofibular overlap measurements were not sensitive enough to detect the syndesmosis malreduction and the A/P Tibiofibular ratio on the lateral view exhibits better diagnostic utility for syndesmosis malreduction.
62
Diagram illustrating the Tibio-fibular clear space (cd), Tibio-fibular overlap (bc), and Medial clear space (ef). ((a), Lateral fibular border; (b), Lateral tibial border; (c), Medial fibular border; (d), Lateral border of posterior tibial malleolus (incisura fibularis); (e), Medial talar border; (f), Lateral medial malleolus border).
Bimalleolar and trimalleolar fractures are inherently unstable fractures and need evaluation for syndesmotic instability intra-operatively. 63 Weber type B fractures associated with SER injuries may be stable or unstable.63,64 SER injuries with significantly increased medial clear space, talar tilt or translation on non-weight bearing x-rays are considered unstable and require operative intervention. 65 Medial clear space measurements of >4 mm or 5 mm on mortise view have been considered to be suggestive of instability,66,67 but Schuberth et al. 68 concluded that this absolute value should not be used to predict instability. When instability is suspected manual external stress and gravity stress radiographs have been recommended to detect occult instability, but both tests have limitations. 65 The reproducibility of the manual stress test has been questioned due to inconsistency of the foot position and the amount of force used to stress. 69 While doing a Gravity stress test radiation exposure to the physician is avoided and the force of gravity used to stress the ankle is constant. 70 Weight-bearing radiographs have been suggested to detect instability, and if the patient can’t bear weight immediately after the injury then obtaining weight-bearing anteroposterior radiographs of the ankle, approximately 5–7 days after the injury has been advised to assess fracture stability and this strategy is more accurate.67,71–73
Although plain radiography and stress fluoroscopy has been extensively used, parameters used to predict syndesmosis using these techniques remain inconsistent.74,75 CT scan has been found more sensitive than plain radiography for detecting malalignment.76–78 CT scans possess several advantages over conventional X-rays—first, no osseous overlaps are present, making the assessment more precise; second, the tibiofibular joint can be visualized directly, which positively influences the accuracy; third, the shape of the incisura fibularis and mal-rotation of the distal fibula can be assessed.
79
Bhimani et al.
80
used weight-bearing computed tomography to obtain 3D volumetric measurements of the syndesmosis and by comparing the injured with the uninjured side they found this method to be a most effective way to diagnose syndesmotic instability. CT Scan does not take into account the amount of cartilage within the distal tibiofibular joint. When the widening does not correlate with clinical findings a contralateral comparative CT or an ipsilateral MRI scan is recommended.
81
MRI has been considered the investigation of choice for suspected syndesmotic ligament injury.
22
It demonstrated a sensitivity of 100% and a specificity of 93% for AITFL injuries and a sensitivity and specificity of 100% for PITFL tears.
82
While direct assessment of the tibiofibular syndesmosis is possible by MRI, assessment of syndesmotic injury by X-ray or CT scans must rely on recognition of secondary signs.
79
The “Lambda Sign” (Figure 4) which is the presence of a contiguous signal from the mortise into the syndesmosis resembling the Greek letter lambda on the coronal PD FS sequences has been found an independent indicator of latent syndesmosis instability.
83
A new sign on MRI (the “ring of fire”) (Figure 5), i.e. the presence of tibial sub-circumferential periosteal oedema 4–6 cm above the ankle joint is highly suggestive of a syndesmosis injury.
84
In a retrospective MRI study, a high prevalence of associated injuries was found, comprising osteochondral lesions (28%), bone contusions (24%), and osteoarthritis (10%).
85
Ultrasound is another modality recommended for diagnosing syndesmotic instability as it can be easily performed in outpatient and bedside settings, is minimally invasive and allows the possibility of dynamic evaluation without radiation exposure.
86
Although dynamic ultrasonographic examination showed a 100% sensitivity and specificity,
87
unfortunately it has the drawback that it cannot detect associated injuries and is investigator-dependent.
22
On the magnetic resonance coronal image, the lambda sign is marked by the red arrow. Magnetic resonance axial image showing the ring of fire sign (marked by red arrow).

Examination under anaesthesia (EUA) should be done in patients when a high index of suspicion exists for syndesmosis injury in the absence of plain radiograph or MRI findings. In addition, EUA should be done before operative fixation to validate the fixation. EUA is done to include dorsiflexion, dorsiflexion external rotation stress, fibular translation test, medial/lateral talar tilt, and an anterior drawer, noting the radiographic parameters described above.
88
Arthroscopy is another tool used for the diagnosis of ankle syndesmotic injuries by directly visualizing the AITFL fibres or diastasis at the tibiofibular syndesmosis89,90 Once the syndesmosis is ruptured the gap between distal tibia and fibula widens, and 3-mm ball can be inserted into this space if AITFL and IOL are disrupted.
91
This test is considered positive when the surgeon can pass a 3-mm or larger instrument tip through this space or the instrument can pass from anterior to posterior direction (Drive-Through sign positive).
92
(Figure 6) Arthroscopy helps measure dynamic diastasis and distinguish instability in multiple planes.20,93 Bhimani et al.
94
performed a cadaveric study and reported that arthroscopic measurement of sagittal plane fibular translation is more accurate than coronal plane diastasis for evaluating syndesmotic instability. Arthroscopic view is demonstrated widening of syndesmosis (long white arrow) and rupture of AITFL (*) (4(a)), drive-through is positive by inserting 3-mm shaver (S) into syndesmotic joint (4(b)), the syndesmotic joint is reduced after syndesmotic fixation (4(c), small white arrow), and AITFL is intact after open repair (4(d), *) (Ti = Tibia, Ta = Talus, F = fibula, * = AITFL, and S = Shaver).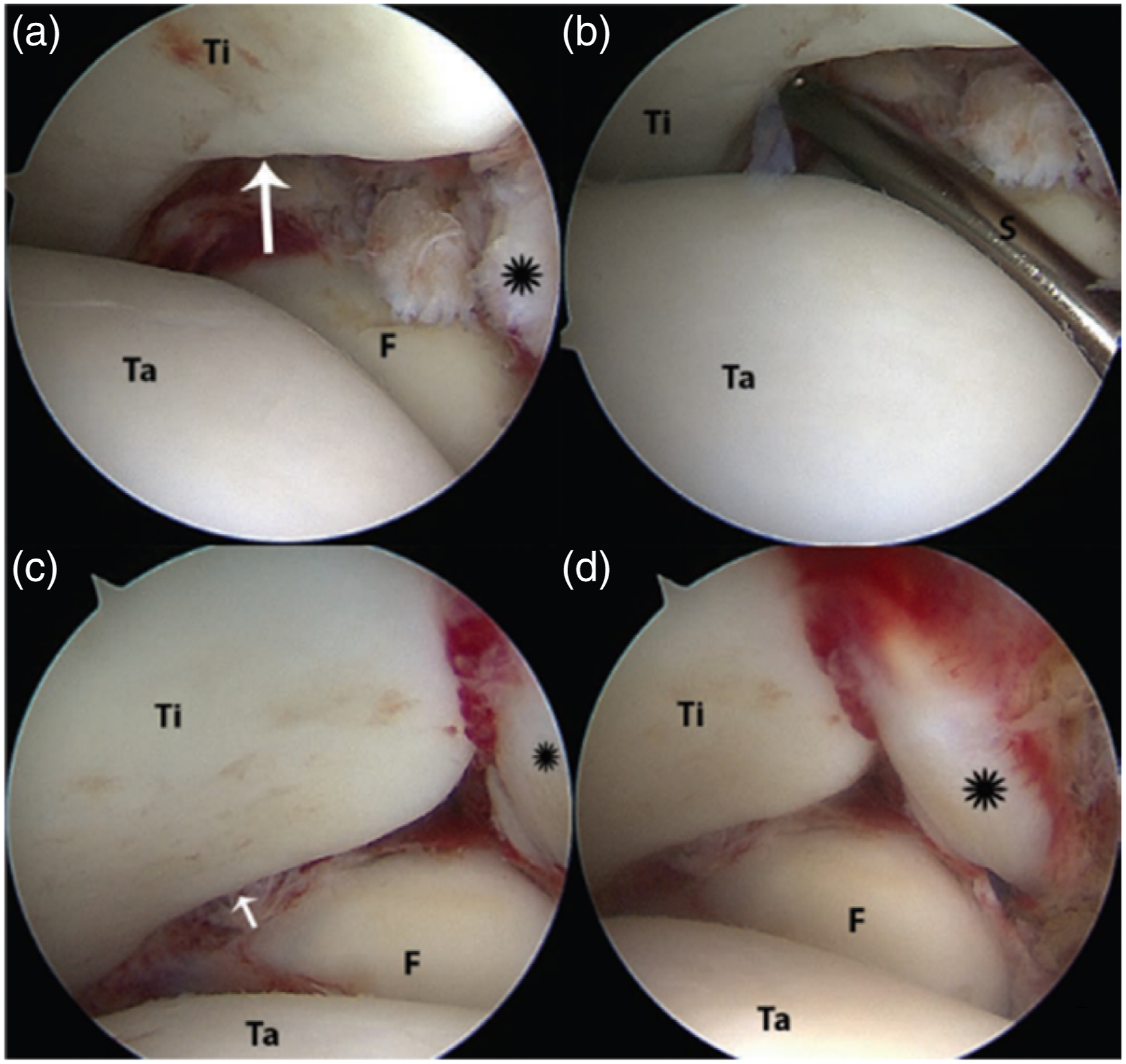
Classification
Many classifications have been suggested for ligamentous syndesmotic injuries but all of them have their shortcomings. 95 One classification is based on the interval between the injury and clinical presentation and divides the injury into acute (<3 weeks), subacute (3 weeks–3 months), and chronic (>3 months). 96 In another system traumatic syndesmotic diastasis was divided into latent and frank groups, and the frank group was divided into four types. Type I is frank diastasis with lateral subluxation of the fibula without fracture; Type II has plastic deformation of the fibula with lateral subluxation; Type III involves posterior subluxation or dislocation of the fibula, and in type IV injuries, the talus is dislocated superiorly resulting in divergence of the tibia and fibula. 97 The clinical relevance of this classification has been questioned by some due to the rarity of the III and IV types. 98 The West Point Ankle Grading System is another system proposed for the classification of pure ligamentous syndesmosis injuries into 3 grades with each grade correlating with progressive disruption of the syndesmotic ligaments and instability. Grade I suggests a partial tear of AITFL with no instability, Grade II suggests a complete tear of AITFL and a partial tear of IOL with some evidence of instability, and grade III represents a complete tear of syndesmotic ligaments with definite instability. 28 Recently ESSKA-AFAS (The European Society of Sports Traumatology, Knee Surgery and Arthroscopy-Ankle and Foot Associates) panel introduced a classification which divides the injuries into Acute (<6 weeks), Subacute (between 6 weeks and 6 months, and Chronic (more than 6 months). Acute injuries are further divided into stable and unstable types, and unstable types can be divided into frank and latent varieties. Subacute injuries are either repairable or non-repairable. Chronic lesions are divided according to the absence or presence of arthritic ankle changes. 22
Treatment
Injuries of the ankle syndesmosis can cause significant disability and time loss, and a much longer recovery period than a common lateral ankle sprain.43,99 Early recognition and appropriate treatment are the keys to restoring stability, mobility and strength, to regain the pre-injury function of the ankle. 16 D’Hooghe et al. 43 evaluated the time to return to play after surgical stabilization of isolated unstable syndesmosis injuries in professional football players. The mean time required to begin on-field rehabilitation was 37 ± 12 days, while the mean time to return to team training was 72 ± 28 days Athletes with injury to both the AITFL and deltoid ligament take longer to return to play than those with an AITFL injury alone, and IOL injury on MRI and PITFL injury on MRI were both independently associated with a delay in return to play. 100 Syndesmotic sprains without instability are treated nonoperatively as they usually heal by non-operative treatment, and non-operative management has been shown to result in good functional outcomes.101,102
Non-operative treatment
Currently, there is no consensus on the non-operative regimen, with treatments ranging from taping to fracture boots to non–weight bearing cast immobilization. 103 Reported lengths of immobilization vary from 1 to 6 weeks.22,104 A three-phase treatment has been suggested. 105 In Phase I the ankle is protected with immobilization and pain and oedema are managed. Phase II starts when pain and oedema are well controlled and the patient can walk with a minimal antalgic gait. Phase II includes strengthening and proprioceptive exercises till the patient becomes asymptomatic. Phase III is started when the patient can jog or hop without pain and includes rigorous strengthening exercises and sports-specific movements.
Operative treatment
Any acute syndesmotic injury with obvious or latent instability needs operative treatment.16,22,88 The goal of the surgery is to achieve accurate reduction which is maintained till the ligaments heal properly.
Syndesmotic reduction is the first and most important component of operative management, as syndesmotic malreduction has been linked to worst outcomes.16,22,54,88,106,107 Recently the effect of the quality of syndesmotic reduction on short-term functional outcomes following ankle fractures was analysed. The post-operative malreduction was proved by a CT scan. There was a strong association between the quality of the reduction and short-term functional outcomes, and patients with anatomically reduced syndesmosis had better VAS and AOFAS scores. 108 In pure ligamentous SI, the need for operative stabilization of syndesmosis is almost always established pre-operatively. However in the presence of ankle fractures the presence of syndesmotic instability needs to be judged before fixing isolated fibular fractures and after fixing fibular, bimalleolar or trimalleolar fractures. Intraoperative fluoroscopy stress tests are commonly used to detect undiagnosed pre-operative syndesmotic instability. 109
A lateral fibular stress test (Cotton test) is performed by applying a lateral distraction force using a surgical clamp to the distal tibia about 1–2 cm proximal to the tibial plafond. The Cotton test is a stress test performed by pulling the fibula laterally to identify the widening of the tibiofibular clear space. This stress test will be positive if the tibiofibular clear space is wider than 1–2 mm as compared to the non-stress condition and it should be more than 5 mm when evaluated by fluoroscopy.109,110 The External rotation stress test is another manoeuvre used to diagnose the syndesmotic instability intra-operatively, but this test can overestimate the syndesmotic instability because an isolated deltoid injury can also lead to increased medial clear space which is evaluated while applying external rotation stress. 111 Tap test is another proven technique to evaluate coronal syndesmotic instability intra-operatively and this technique involves advancing a cortical tap through a drilled hole in the fibula which produces a unidirectional distraction force to the tibia.112,113 A recent cadaveric study compared the Cotton test and Tap test for the assessment of coronal instability. The Cotton test and Tap test had, respectively, 73.3% and 70% sensitivity, 100% and 90% specificity, and 86.7% and 80% diagnostic accuracy. 113 The Torque test is another described method to assess syndesmotic instability, and it involves stressing the fibula in a posterolateral direction and assessing instability under direct visualization of the syndesmosis. 114 For assessing sagittal plane instability lateral relationships of the tibia and fibula are found to be more sensitive. 115 Therefore antero-posterior rocking of the fibula with a clamp can be used to appreciate sagittal plane instability. Once the presence of syndesmotic instability is proven by closed or open means, the challenge is to reduce syndesmosis anatomically.
Strategies to reduce syndesmotic injury include closed reduction, open reduction and arthroscopic assisted reduction.16,22,88 A common mode of malreduction is an anterior translation of the distal fibula with respect to the tibia, and syndesmotic reduction in the sagittal plane can be improved by supporting the leg under the calf with the foot hanging freely. 116 The most common closed method used to reduce the syndesmosis has involved the placement of a pointed reduction clamp around the distal tibia and fibula to maintain the reduction of the syndesmosis with fixation. Studies have demonstrated that inappropriately placed clamps may predispose to iatrogenic malreduction depending on the orientation of the clamp, and excessive force used for reduction can lead to significant syndesmosis over compression.117–119 When using a reduction clamp, the orientation of the clamp along the trans-syndesmotic axis is suggested, which can be achieved by placing one time on the fibular ridge and medial tine in the anterior third of the tibia. 120 Thumb technique is another suggested technique for syndesmotic reduction. In this technique fibula is manipulated with the thumb and when there is no palpable step at the anterior distal tibiofibular incisura the syndesmosis is considered to be reduced. 121 Recently modified Glide Path technique has been described for syndesmotic reduction and it consists of manual reduction of the fibula and placement of a Kirschner wire through the fibula and tibia along the trans-malleolar axis. The syndesmosis can then be reduced along the glide path created by the Kirschner wire to prevent posterior or anterior malreduction. 122 This technique is a modification of the previously defined glide path technique which relied on open reduction than manual reduction. 123 Direct visualization of the tibiofibular joint has been advocated for accurate reduction and this technique reduced the malreduction rate from approximately 50%–15%.106,124 Open reduction involves visualization of the fibula within the incisura and checking articular congruity of the distal tibia, distal fibula, and talus through an anterolateral approach. Mercedes sign, a three-branch star formed by the tibiotalar, talofibular and syndesmosis joints has been suggested to assess reduction during an open technique. 125 In one study open reduction of the fibula through a lateral or posterolateral fibular incision strategy was suggested and incisura was assessed through the given incisions to palpate the reduction between the tibia, fibula, and talus. Assessment of reduction was done with or without directly visualizing the syndesmosis and both techniques were found to be equally effective. 126 The “tibiofibular line” (TFL) is a CT-based technique found to be sensitive to malreduction and in one recent study, it was shown that CT based TFL can be effectively translated into a reliable open technique. 127 The accuracy of the achieved reduction should be verified by comparing it with perfect mortise and lateral view of the opposite uninjured side, which is used as a template in the operating room. 128 Arthroscopy is another method used to identify instability as well as verify reduction.20,93,94 Operative treatment of syndesmotic Injuries with assisted arthroscopic reduction has been reported. 129
Once a satisfactory reduction is achieved the syndesmosis needs stabilization. Various fixation methods have been reported, including metallic screws, suture button devices, bioabsorbable screws and direct ligament repair.16,22,88
Trans - syndesmotic screw fixation
Syndesmotic screws (Figure 7) have been used for decades for the stabilization of syndesmotic injuries with good radiological and functional outcomes.130–133 The advantages of the screws include low cost and better torsional resistance to sagittal translation of the fibula compared with flexible suture button devices.15,134 However, there are different opinions about the material, number, type and size of screws to be used. The other controversies include the number of cortices to be purchased, how proximal to the tibial plafond the screws should be placed, and whether routine screw removal is required. Both metallic and bioabsorbable screws have been used to stabilize syndesmosis. Bioabsorbable screws have been recommended because of no or minimal radiological interference, and no requirement to remove the screw.135,136 Foreign body reaction remains a concern with bioabsorbable screws, but with modern formulations, this issue is more or less solved.
137
The higher cost of the bioabsorbable screw remains a problem. Syndesmotic injury with both posterior malleolus and anterior malleolus involvement. Both anterior and posterior malleolus stabilized with screws and syndesmosis stabilized with two 3.5 mm tricortical screws and fibular plate.
Both 3.5 mm and 4.5 mm screws have been used for syndesmotic fixation, and both sizes have equivalent biomechanical characteristics, but the optimal screw size remains a controversy.138,139 The diameter of the screw should never be less than 3.5 mm because it is likely to break. 125 4.5 mm screws are less likely to break, and allow easier removal, but can potentiate a stress riser. 88,139 Although a 4.5 mm screw with quadrilateral fixation has a higher resistance to shear stress than a 3.5 mm screw, 140 both of them are biomechanically equivalent for stabilization of syndesmotic injury. 139 The screw is to be inserted in neutralization mode and not in lagging mode.141,142 Trans-syndesmotic screw fixation can lead to over-tightening of the syndesmosis which can lead to decreased dorsiflexion post-operatively.143,144 In a finite-element model, it was found that over-tightening of the distal fibular syndesmosis resulted in medial fibular displacement and widening of lateral gutter clear space, and the effect increased as screws were placed closer to the plafond. 145 Biomechanical studies have shown that a small change in the lateral gutter space can significantly change the tibiotalar contact forces. 146 The proper screw position is traditionally described as 2–5 cm proximal and parallel to the tibial plafond, angled 20–30° anteromedially along the trans-malleolar axis.88,132,147–149 The placement of a screw greater than 41 mm above the tibial plafond can negatively influence the outcomes. 149 Trans-syndesmotic screw fixation within 2 cm of the tibial plafond may better restore syndesmotic stability but can lead to synostosis.132,142,148 The inherent problem of placing the screw 20–30° to the horizontal plane is that it does not consider the rotation of the limb. In a CT-based cross-sectional study it has been found that with the ankle in a neutral position and the second toe positioned anteriorly, the ideal angle of syndesmotic screw placement was 18.8°. 150 The other concern during screw insertion is iatrogenic cartilage damage to the tibiofibular syndesmosis. In a cadaveric study which identified the cartilage of the syndesmosis, it was found that syndesmotic fixation placed 13 mm proximal to the tibial plafond would safely avoid the articular cartilage. 151
The number of cortices to be purchased with the screw is another controversy. In a cadaveric study three and four cortex fixation demonstrated no significant difference in mechanical stability. 139 In a long-term comparative study there was no significant difference in radiographic and functional outcome between 3- and 4-cortex fixation at 8.4 years follow-up. 152 In a tricortical fixation single cortical hold on the lateral tibial side allow micromotion during the early range of motion or weight bearing leading to resorption of the surrounding bone allowing screw loosening rather than screw breakage, thus making routine removal of the screw unnecessary. 153 However, diastasis during syndesmotic healing may be a concern which can be prevented by adding another tricortical syndesmotic screw. 153 Both single and double-screw fixation methods have been recommended in the literature. In one study of bimalleolar fractures with syndesmotic injury, syndesmotic fixation with one 3.5 mm tricortical cancellous screw fixation was compared with two 3.5 mm tricortical cancellous screws fixation and no difference was found between the two types of fixations. 154 Two screws are preferred in a large non-compliant patient, in the presence of high fibular fractures like Maisonneuve fractures, or ankle fractures in diabetic patients.155,156
Syndesmotic screws are known to have high rates of screw breakage and loosening. 117 It is due to this reason routine removal of syndesmotic screws has been suggested.149,156 However, routine removal of syndesmotic fixation is not supported by the literature, and many investigators have reported no clinical, radiographic, or functional difficulties in the presence of retained broken syndesmotic screws.117,157,158 Syndesmotic screws removal is indicated for painful hardware or limited ankle dorsiflexion after 4–6 months post-operatively. 149 In fact, if malreduction is noted postoperatively, screw removal has been shown to allow for in situ reductions and restoration of syndesmosis motion.58,124 The disadvantages of screw removal include increased cost of treatment, more recovery time, late diastasis if the syndesmotic ligament does not heal, and wound infection.153,159 Gennis et al. 133 compared radiographic syndesmotic widening and talar shift over time in patients with removed versus retained screws. They found evidence of increased radiographic widening of the syndesmosis in patients who had screws removed compared to those with retained screws, even if the retained screws were loose or broken. Although screw breakage is often asymptomatic, the breakage location can be unpredictable and result in painful bony erosion when breakage is within the fibula or tibia. 160 Extraction of the broken screws can be technically difficult and lead to complications. 161 A novel screw with a controlled break point between the tibia and fibula has been developed with design features that allow for easy extraction of both fragments. 162 Development of stress fracture can be a problem with the use of syndesmotic screws particularly in osteoporosis, and adding a plate helps to distribute loads on the plate instead of screw heads. 163 To avoid trans-syndesmotic screws in lateral malleolus fracture a novel syndesmotic plate has been developed which has fixation strength comparable to screws. 164
The distal tibio-fibular syndesmosis acts as a dynamic stabilizer of the ankle joint by allowing some movement of the fibula in the coronal plane, axial plane and rotational plane. 13 Trans-syndesmotic is a rigid construct and prevents this physiological motion, although the use of tricortical screws may allow some micromotion, it can’t match the normal physiological play between the tibia and fibula. 153 This led to the development of flexible fixation devices which maintain syndesmotic reduction and allow some rotational, proximal-distal, and anterior-posterior movement of the fibula relative to the tibia. 165
Flexible fixation
Recent years have seen the advent of less rigid constructs such as suture button (Figure 8) which is strong enough to withstand physiologic loading that occurs with weight bearing and normal ankle motion.
166
The physiological reduction achieved with a flexible device allows for earlier rehabilitation, and less need for implant removal.167–169 In a recent study 147 patients treated with suture buttons were followed with postoperative bilateral CT imaging to analyse rotation and translation of the suture button drilling tunnels, and it was found that the suture button system postoperatively deviated to compensate for intraoperative malreduction.
170
There are many studies which compared suture button devices with screws and suggested greater functional outcomes, quicker return to sport, and comparable postoperative reduction volume on computed tomography following repair with suture buttons.171–173 Lehtola et al. followed 43 patients of pronation external rotation ankle fractures treated either by syndesmotic screw or suture button for a minimum of 6 years to assess syndesmosis reduction and OA grade. They found syndesmotic screw and suture button maintained reduction equally well and both methods resulted in moderate OA.
174
Although flexible devices are preferred especially after athletic injuries, these devices do have some drawbacks. It has been reported that the suture button allows supra-physiological fibula range of motion particularly posteriorly in the sagittal plane and less resistance to external fibular rotation.175,176 The suture-button device alone results in poor stability during rotational forces when DL is injured.
177
Furthermore, there are concerns when a suture button is used for severe injuries with wide diastasis, with regard to late loss of reduction and the ability of the suture button to truly hold an anatomic reduction.
129
Surgical technique for suture button fixation is demonstrated. The guidewire with protector was inserted from the fibula to the medial malleolus direction and the direction is parallel to the ankle joint with 20–30° angulation to the horizontal plane (Figures 5(a) and (b)), after obtaining a good position, a 3.5 mm drill is following (Figure 5(c)) and then suture button is introduced from fibula to medial malleolus direction (Figure 5(d)), a small incision is created on the medial side to check the position of the medial button and make sure that no compression on neurovascular structures before tightening the suture on the lateral side (Figure 5(e)), and final fluoroscopic view of ankle AP and lateral views (Figure 5(f) and (g)).
To overcome the supra-physiological movements with single suture button constructs various options have been suggested which include a combination of suture buttons and syndesmotic screws, double suture buttons and AITFL augmentation. 177 In a controlled laboratory study, it was found that hybrid fixation with 1 suture button and 1 tricortical screw appropriately restored tibiofibular kinematics for early weight bearing. However, over constraint of motion during inversion was a concern. 121 One study showed a combination of screw and suture-button fixation in purely ligamentous injuries allows for initial rigid fixation until screw removal, which can be performed in the office. The suture buttons then remain for longer-term stabilization. 178 In one study hybrid fixation with a suture button and a trans-syndesmotic screw was performed for Dennis-Weber Type C fractures with syndesmotic injuries a high accuracy of reduction, a low rate of diastasis and favourable clinical outcomes were achieved. 179 Direct anatomical repair of AITFL with suture anchors, with suture tape is another technique which has been successfully used for the management of syndesmotic instability associated with external rotation-type ankle fractures.180–182 While using this technique the integrity of PITFL should be ensured otherwise compression of AITFL anteriorly will widen the tibiofibular clear space posteriorly. 42 A recent biomechanical study reported that AITFL suture repair with or without suture tape augmentation may be a good operative addition or alternative to suture button fixation for isolated syndesmotic disruptions. 183 Use of two tightropes has been recommended to provide more stability in proximal fibula or Maisonneuve fractures, as well as Weber type B fractures, comminuted fractures and in obese patients. When using two tightropes, it is recommended to place the second tightrope approximately 1 cm proximal to the first with slight axial divergence to increase rotational stability. 184 In a finite analysis, an intact model, an injury model, and eight different fixation models with only screw/screws, only suture button/suture buttons, and hybrid models with suture buttons and screws were studied for biomechanical analysis. The models were compared in terms of lateral fibular translation, posterior fibular translation and external rotation of fibula compared to tibia and stress values occurred on screws. In the hybrid-1 model, comprising one screw at 4 cm and one suture button at 2 cm from the tibial plafond lateral fibular translation and external fibular rotation values were obtained as close to the intact model. 185
Suture buttons have some other issues too. The braided sutures within the SB implant provided a conducive environment for the development of infection across the syndesmotic fixation tract, suggesting the need for prompt infectious workup in the presence of suture button migration or osteolysis. 186 In cadaveric studies of suture button fixation, it has been shown nerve entrapment can occur 10%–20% of the time and saphenous vein entrapment can occur 10%–37% of the time, and to avoid this entrapment a medial incision has been suggested.187,188 A newer knotless device has demonstrated good clinical results and reduced the possibility of entrapment and skin irritation seen in previous devices. 172 In a latest study, a knotless suture button was compared with trans-syndesmotic screw fixation, and both devices produced equally good long-term results, however, athletes returned to sports earlier with suture button devices. 189 Flexible devices have shown better short-term results in athletes presenting with pure ligamentous injuries and may be preferred over the trans-syndesmotic screws in this situation, but long-term results with both devices are the same, thus allowing the surgeon to opt for any of these techniques according to the working conditions. AITFL augmentation is recommended by some authors, but long-term studies proving the efficacy of this technique are still awaited.
Syndesmotic injuries with ankle fractures
Distal tibiofibular diastasis injury occurs in 11%–20% of ankle malleolar fractures.130,190 Syndesmotic instability is most commonly present in pronation external rotation injuries followed by supination external rotation injuries according to the Lauge-Hansen classification.38–40 Appreciation and treatment of the syndesmotic instability are extremely important as syndesmotic malreduction has been associated with poor functional outcomes and the development of osteoarthritis.106,107,110,191–194 Achieving accurate syndesmotic reduction and its maintenance is considered a critical factor in the treatment of ankle fractures with associated syndesmotic instability. 195 Rates of syndesmotic malreduction are higher in Weber C fibular fractures than in Weber B fibular fractures.118,196 Rates of syndesmotic malreduction are almost double in pronation external rotation injuries than in supination external injuries. 197
Most of the patients with malleolar fractures present with severe symptoms which do not allow the physician to perform special tests which are done to evaluate ligamentous injuries. In the presence of clinical suspicion, radiographs are recommended and generally, anteroposterior (AP), lateral and mortise views are used during radiographic examination. These radiographs are used to assess the relationship between the tibia and fibula and notice malleolar fractures and bony avulsions of the anterior or posterior fibula which are present in up to 50% of SI. 52 Bimalleolar, trimalleolar and ankle fracture-dislocations are considered unstable fracture patterns and require operative management. 198 thus allowing an opportunity to assess syndesmotic instability intraoperatively. Predicting instability in the presence of isolated fibular fracture is challenging. Weber type A fractures which occur below the level of the syndesmosis are generally stable fracture patterns. 65 Weber C isolated lateral malleolar fractures secondary to a rotational injury are generally unstable due to associated injury. 198 Isolated fibular fractures at and above the level of syndesmosis with increased medial clear space, talar translation and tilt on non-weight-bearing x-rays are considered unstable. 65 The challenge lies in diagnosing the instability in Type B Weber fractures without any signs of sufficiently increased medial clear space, talar translation or tilt. 198 External rotation stress radiographs,65,199 gravity stress radiographs, 70 or weight-bearing radiographs after a short period of weight-bearing on the fractured ankle 200 have been suggested to establish instability. However, the most accurate method for assessing instability remains without consensus. The use of additional radiographic measurements such as the lateral talar displacement ratio, derived in relation to the talar body width on ankle stress imaging can provide additional information in determining stability when MCS is within a clinical gray area. 201 In one more recent study, it was found that fractures ending between the level of the plafond and the lower physeal scar of the tibia are 2.4 times more likely to have a syndesmotic injury as compared to those which end below the plafond. 202 In many patients with ankle fractures, accurate prediction of syndesmotic instability can be done using radiological parameters and Lauge-Hansen classification. 203 However, a CT scan is more sensitive than radiographs and can pick up subtle diastasis, subtle fractures and rotational abnormalities of the fibula.53,77,204 Most surgeons agree that a CT scan is always necessary for correct pre-operative planning, because some fractures may be overlooked in radiographs.205–207 Donohoe et al., demonstrated that performing a preoperative CT scan changed 52% of fracture identifications and in 44%, the surgical approach and patient positioning. 205
It has been realized that osseous equivalents of syndesmotic injury occur and should be treated with stable internal fixation anatomically, and these osseous equivalent injuries include fractures of the posterior malleolus, fracture of the Chaput tubercle of the tibia, fracture of the Wagstaffe tubercle of the distal fibula. 208 Recently “Quadrimalleolar Concept” for ankle fractures has been introduced according to which the ankle is divided into four areas on the axial CT scan: (A) (posterior malleolus), (B) (medial malleolus), (C) (lateral malleolus), and (D) (anterior malleolus Chaput and/or Wagstaffe fragments), and depending on the malleolus involved surgical approach and fixation strategy is suggested. 209
Posterior malleolar injury represents instability of the bony attachment of the PITFL,
208
and out of all ligaments stabilizing the syndesmosis PITFL provides the greatest strength.
18
A study concluded that fixation of PM restored PITFL function because all ankle fractures with posterior malleolus injury had intact PITFL which was attached to the fractured fragment.
210
A cadaveric model showed fixation of the posterior malleolus restores 70% of the syndesmotic stiffness compared with 40% after trans-syndesmotic screw stabilization.
211
Anatomical reduction of the PM fragment also restores the articular surface and the normal anatomy of the inferior tibiofibular joint so its fixation has been advocated.
212
(Figure 9) In a recent study trans-syndesmotic screw frequency was evaluated after fixing the posterior malleolar fractures involving less than 25% of the articular surface and a significant decrease in trans-syndesmotic screw need following osteosynthesis of PM was noticed.
213
Recent studies have recognized posterior malleolus as an important contributor to syndesmotic stability and congruent ankle alignment and a significant decrease in the frequency of need for trans-syndesmotic screw after PM fixation.214,215 When it comes to fixation of the PM, direct open reduction is more stable than indirect reduction and anteroposterior screw fixation.216–219 A routine use of CT scan of all posterior malleolus fractures is recommended to determine the size, orientation, comminution, and articular impaction.
220
Numerous classifications of PM fracture are suggested in the literature to understand the configuration of the PM fractures as well guide the selection of approach and fixation strategy.217,221,222 A trimalleolar fracture treated by open reduction and internal fixation of the lateral malleolus, posterior malleolus and medial malleolus. Syndesmosis stabilized itself after fixation; hence, no syndesmotic stabilization was required.
Fractures of the Chaput tubercle of the tibia may result in failure of the AITFL. Wagstaffe tubercle represents the avulsion of the fibular attachment of the AITFL and must be recognized and addressed at the time of fixation.208,209,218 By reducing and stabilizing the Chaput fragment, the AITFL ligament is tensioned, thus allowing the correct reduction of the fibula within the tibial incisura. 223 Its correct stabilization restores the anatomical configuration of the incisura fibularis and anterolateral tibial plafond and helps to avoid anterior and valgus displacement of the talus. 209 Extra-articular small bony avulsions are fixed with suture anchors or transosseous sutures, larger fragments involving the tibiotalar joint and the tibial incisura for the fibula can be fixed with 3.5-mm cannulated screw with a washer, and depressed fracture of the anterolateral tibial plafond may need plating. 209 Wagstaffe fracture represents the avulsion of attachment of AITFL on the fibular side and may or may not be associated with fibular fracture and the treatment of this fragment is mostly based on the size of the fragment. 224
After fixing the malleolar fractures syndesmotic stability must be checked intra-operatively. 209 Several intraoperative tests like the Cotton test, External rotation test, Tap test and Torque test discussed earlier are performed to assess the instability. The biggest concern is subtle rotational malreduction of the fibula in the incisura which has been found in 50% of the patients and is not always appreciated on plain radiography or even direct visualization intraoperatively.158,225,226 A method for the detection of lateral malleolar malrotation using conventional fluoroscopy has been described, which takes into consideration the shape of the distal fibula and lateral talofibular space to judge fibular malrotation. 227 The other technique recommended to diagnose syndesmotic instability includes intra-operative CT. 227 However, this facility is not routinely available to many surgeons. A recent study showed no difference in the rate of syndesmotic malreduction with the use of intraoperative CT compared with standard intraoperative fluoroscopic views. 228 Open reduction,106,124 and arthroscopy20,93 are other strategies suggested to diagnose instability and assist reduction. If there is no obvious instability and ankle mortise is restored, it will allow healing of the ligaments of the ankle and syndesmosis in anatomical position. 229 When the syndesmotic instability is present, the syndesmosis needs to be stabilized with a flexible device or trans-syndesmotic screw with or without AITFL repair or supplementation, and the advantages and disadvantages of these techniques have been discussed previously.
Another emerging strategy for syndesmotic instability management is acute deltoid repair. Fractures of the distal fibula with concurrent injury to the deltoid ligament are rotationally unstable injuries and lead to instability across the syndesmosis and widening of medial clear space with decreased tibiotalar contact.230–232 Assessment of ankle instability after fixation of lateral malleolus and syndesmosis is recommended and medial clear space widening and talar tilt as indicators of instability persistent medial instability. 233 Deltoid injury and infolding of the deltoid complex can prevent anatomic reduction of medial clear space even after fixation of fibula and syndesmosis which warrants exploration of the medial side for deltoid complex injury and its repair.234–236 In one retrospective study of bi-malleolar equivalent fractures, patients underwent one of three methods after fixation of the distal fibula: trans-syndesmotic fixation, deltoid ligament repair, or combined trans-syndesmotic fixation and deltoid ligament repair. At midterm follow up deltoid ligament repair yielded similar functional scores and fewer reoperations compared to trans-syndesmotic fixation and authors concluded DL repair may be a favourable treatment strategy when considering trans-syndesmotic fixation. 237 In a systematic review to define the role of DL repair in ankle fractures with Weber B and Weber C fibular fractures and syndesmotic instability, the authors reviewed three surgical strategies of DL repair as a principle method of syndesmosis stabilization, trans-syndesmotic screw fixation, and a combination of DL repair and syndesmotic stabilization. The authors concluded that DL repair offers lower syndesmotic malreduction rates and reduced re-operation rates for hardware removal in comparison to trans-syndesmotic screws. 238 In a retrospective study of 78 cases of acute ankle fractures with DL disruption, the authors found that medial instability may persist even after fracture fixation and syndesmotic stabilization, and concluded that a direct repair of the deltoid ligament was adequate for restoring medial stability. 239 In a comparative study evaluating ankle fractures treated with or without DL repair, surgical repair of the DL helped in decreasing the postoperative MCS and malreduction rate, especially for the AO/OTA type-C ankle fractures. 240 It appears from the recent literature that even after syndesmotic fixation ankle instability may persist in some highly unstable ankle fractures and these fractures will need deltoid repair even after syndesmotic stabilization. Using deltoid repair as a substitute for syndesmotic fixation is controversial. Our strategy is to look for medial clear space widening and talar tilt after fixation of the lateral and posterior malleolus and explore the medial side if medial instability is present. DL is then repaired and an additional syndesmotic stabilization is done if syndesmotic instability persists after DL repair. (Figure 10) To do DL repair before or after syndesmotic fixation is controversial. Primary repair of AITFL is another technique suggested for syndesmotic instability associated with ankle fractures. In a systematic review, early functional results were found to be better after AITFL repair compared to syndesmotic fixation alone, however, there was no difference in terms of late functional and radiological outcomes. 241
Chronic syndesmotic injury (CSI)
The definition of chronicity varies, from 6 weeks to 6 months.22,97,242 Chronic syndesmotic instability and diastasis are due to failure to detect and treat or inadequate treatment of acute injuries. Diabetics with neuropathy and obese patients are more likely to develop a chronic condition.243,244 The patients present with pain which increases with weight bearing, persistent swelling in the ankle region, reduced range of ankle motion particularly dorsiflexion and feeling of instability while walking on uneven ground. In long-standing injuries, the symptoms may mimic ankle osteoarthritis. 242 The patients with suspected chronic syndesmotic injury (CSI) are subjected to special tests used for an acute injury which may not be as specific as in acute injury. In one study palpation of the anterior syndesmosis evoked dull tenderness in 18 of 20 confirmed chronic injuries, 3/20 patients had positive external rotation test, and 2/20 had positive squeeze test translating to 90%, 15%, and 10% specificity, respectively. 245
Different techniques have been described for chronic syndesmotic rupture, which includes arthrodesis of the syndesmosis, 246 screw fixation after reduction,247–249 and ligamentous reconstruction.250,251 Almost all techniques involve debridement of the syndesmosis of the scar tissue to achieve reduction. In chronic syndesmotic injury (CSI) associated with ankle fractures, the bony component of the injury and malunion need to be considered. 125
CSI can lead to chronic pain due to anterolateral ankle impingement from the impingement of scar tissue and hypertrophic synovium between the tibia and fibula. There is no instability in these patients and they respond well to arthroscopic debridement and arthrolysis.
242
In some patients, chronic pain after a syndesmotic injury is due to tibiofibular ossification and synostosis, and these patients can be treated by resection of synostosis and sealing the debrided areas with bone wax.98,252 Chronic syndesmotic injury (CSI) associated with diastasis is amenable to arthroscopic or open debridement followed by secondary fixation with syndesmotic screws or suture-button implants.253–255 The use of a combination of a screw and suture button
253
or two to three suture buttons
254
are other suggestions for syndesmotic fixation. Recently a new aperture fixation device has been developed and it is composed of a threaded tibia anchor, fixed-length suture bridge, and telescoping fibular anchor. This construct provides more strength and stiffness and less stretch and creeps compared with suspensory suture button devices.
256
This device has been used for recurrent syndesmotic diastasis following screw fixation for pronation-external rotation (Weber C) fractures,
257
Before syndesmotic fixation congruent ankle must be restored, and this restoration may require correction of the malunions in CSI associated with malunited ankle fractures and debridement of the syndesmosis.
242
In case medial clear space remains open after syndesmotic reduction, it needs to be explored to remove any interposed tissue.
125
and if there is gross medial instability with a valgus tilt of the talus DL repair may be required.
98
Pronation external rotation injury with deltoid ligament injury with posterior malleolus fracture accompanied by a wide lateral translation of talus. The posterior malleolus and lateral malleolus was fixed and deltoid ligament repair was done. Trans syndesmotic screw used to protect deltoid ligament repair and was removed after 3 months.
Because the syndesmosis is dynamic in nature, many investigators have propagated a dynamic ligament reconstruction. Various techniques have been described, but the general principle involves the creation of bone tunnels and the passage of tendon grafts to recreate various components of the syndesmotic ligamentous complex. Dekker et al. used double limb allograft to reconstruct the interosseous ligament without attempting to reconstruct each ligament. 258 Grass et al. 250 recommended a split peroneus longus tendon graft for a near anatomic reconstruction of the AITFL, IOL, and PITFL at the level of the chronically unstable syndesmosis to reconstruct the 3-point fixation of the distal fibula. Lui 259 described a minimally invasive technique involving arthroscopic guidance and peroneus longus tendon autograft. When required suture tapes have been used for the augmentation of AITFL.182,260 Tibiofibular or syndesmotic fusion is another technique recommended for CSI. 243 Tibiofibular synostosis results in a nonphysiological stiffness of the ankle mortise by eliminating the 3-dimensional fibular motion with tibiotalar motion which may subsequently cause ankle arthritis. Olson and colleagues 261 followed 10 patients of tibiofibular arthrodesis for at least 2 years and reported favourable results, although three patients required reoperation no secondary ankle fusion became necessary.
Conclusion
A syndesmotic injury may be a pure ligamentous injury or accompany ankle fractures. Pure ligamentous injuries can be easily missed unless there is a high index of suspicion. Isolated ligamentous injury with diastasis needs syndesmotic stabilization with trans-syndesmotic screws or flexible devices. Because most isolated ligamentous injuries occur in athletes, the use of flexible devices like a suture button is preferred because it allows physiological reduction, earlier rehabilitation, and less need for implant removal. SI associated with ankle fractures requires anatomical fixation of both malleoli and osseous equivalents of syndesmotic ligaments like PM, Chaput tubercle, and Wagstaffe tubercle. Once the bony fragments are reduced the syndesmotic stability is checked intraoperatively by stress tests. If the syndesmotic instability persists, accurate syndesmotic reduction and stabilization with a trans-syndesmotic screw or flexible device are required. Persistence of increased medial clear space and valgus tilt warrants medial side exploration and DL repair. CSI without diastasis requires debridement which is done mostly arthroscopically. For CSI with diastasis, reconstruction is preferred and arthrodesis is considered a last resort.
Footnotes
Acknowledgements
I would like to acknowledge the assistance of Dr Gaganpreet Singh Bedi for his invaluable contribution to provide images of radiological signs (the lambda sign and the ring of fire sign).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.