
Abstract
Lateral ankle instability is one of the most common problems seen in the orthopaedic setting. Proper diagnosis is essential in order to provide the ideal treatment for these patients. All patients are subjected to nonoperative management in the form of functional rehabilitation. For those, however, who did not respond well to therapy, surgical treatment is then recommended. There are several surgical techniques available which have been meticulously studied and discussed in previous articles. The focus of this paper is on the author’s perspective on choosing the surgical technique based on the quality of the anterior talofibular ligament and calcaneofibular ligament remnants. All patients are subjected to a diagnostic arthroscopy, where the remnant is assessed. The procedure then of doing an all-arthroscopic, open Modified Brostrom or anatomic reconstruction is then chosen based on this initial assessment
Keywords
Introduction
Lateral ankle sprain is one of the most common musculoskeletal injuries, which particularly have a high incidence among physically active individuals. In the US, among the general population, it was estimated to be four to seven acute ankle sprains/1000 person-years. 1 Collegiate athletes have an incidence of 0.7–1.3/1000 while Olympic level sprains showed a rate of 3.2–3.5/1000. Moreover, the incidence in active military duty was noted to be at 58.3/1000. Despite the advancement of medical technology and vast development of nonoperative treatments, approximately 10–30% still result in chronic ankle instability. 2 There are multiple surgical techniques developed over the years. The purpose of this paper was to provide a focused overview of the surgical options that may cater to specific group of patients in relation to their level of activity.
The most common mechanism of injury in ankle sprains is a combination of inversion and plantar flexion. 3 The lateral stabilizing ligaments include the anterior talofibular, calcaneofibular and posterior talofibular ligaments. The anterior talofibular ligament is the most commonly injured. During an inversion injury, the superior part of the ATFL is the first structure to tear. If the force continues to be exerted, the inferior fascicle of the ATFL along with the CFL may be involved. Concomitant injury to this ligament and the calcaneofibular ligament can result in mechanical ankle instability.4,5 The posterior talofibular ligament is the strongest of the lateral complex and is rarely injured in an inversion sprain.
Clinical examination
Ankle trauma is evaluated with a meticulous history and proper physical examination. Taking note of the mechanism injury, position of the foot and any event that causes recurrence of the injury are essential to the history. Varus deformity may be noted for patients with chronic lateral ankle instability.6,7 Pain and swelling are the most common presenting symptoms with a lateral ankle sprain. The entire length of the leg should be palpated to detect any fracture or an associated syndesmotic injury. Tenderness along the peroneal groove may suspect a tendinous pathology or pain at base of the fifth metatarsal may indicate a fracture or an avulsion of the peroneal brevis tendon. Deep pain and effusion along the talocrural joint line should raise suspicion of an osteochondral talar dome lesion. The anterior drawer test can be used to assess the integrity of the anterior talofibular ligament, and the inversion stress test can be used to assess the integrity of the calcaneofibular ligament.
8
Special tests are useful to suspect the presence of a syndesmotic injury. A squeeze test, performed by compressing the fibula and tibia at the midshaft area, is considered positive if pain is elicited distally over the tibia and fibular syndesmosis. An external rotation test is also recommended to identify a syndesmosis injury. This test is performed with the patient’s knee resting over the edge of the table. The physician stabilizes the leg proximal to the ankle joint while grasping the plantar aspect of the foot and rotating the foot externally relative to the tibia. If pain occurs with this manoeuvre, the test is noted to be positive.
9
There are still a number of tests to determine syndesmotic instability, such as single leg hop test, syndesmotic ligament tenderness, dorsiflexion-external rotation tests. No single test is sufficiently accurate and authors have recommended combination of different examinations.
32
Figure 1. Inspection of the ankle. Arrow shows effusion of the ankle joint.
Imaging
Radiograph of the ankle is the first line of diagnostic examination to be taken. Standard AP, lateral and mortise views are essential to rule out any fracture or bony abnormalities. Stress radiographs may be useful, but are often not routinely used due to the discomfort to the patients.
For ankle sprains that remain symptomatic for more than 6 weeks, computed tomographic (CT) scan or magnetic resonance imaging (MRI) should be considered to rule out talar dome lesions. CT or MRI studies should also be considered for ankle injuries that involve crepitus, catching or locking, because these symptoms may be associated with a loose body or displaced osteochondral fragment. MRI studies may be helpful in identifying syndesmosis injuries and peroneal tendon involvement. In patients with lateral ankle instability, one may be able to visualize the quality of the ATFL and CFL and assess their integrity. The accuracy, however of MRI is limited to diagnosing chronic ATFL injuries.
10
It is valuable in detecting other associated pathologies such as osteochondral injuries Figure 2. Ultrasound is a more sensitive tool in diagnosing both ATFL and CFL injuries.
11
MRI images showing absence of the ATFL.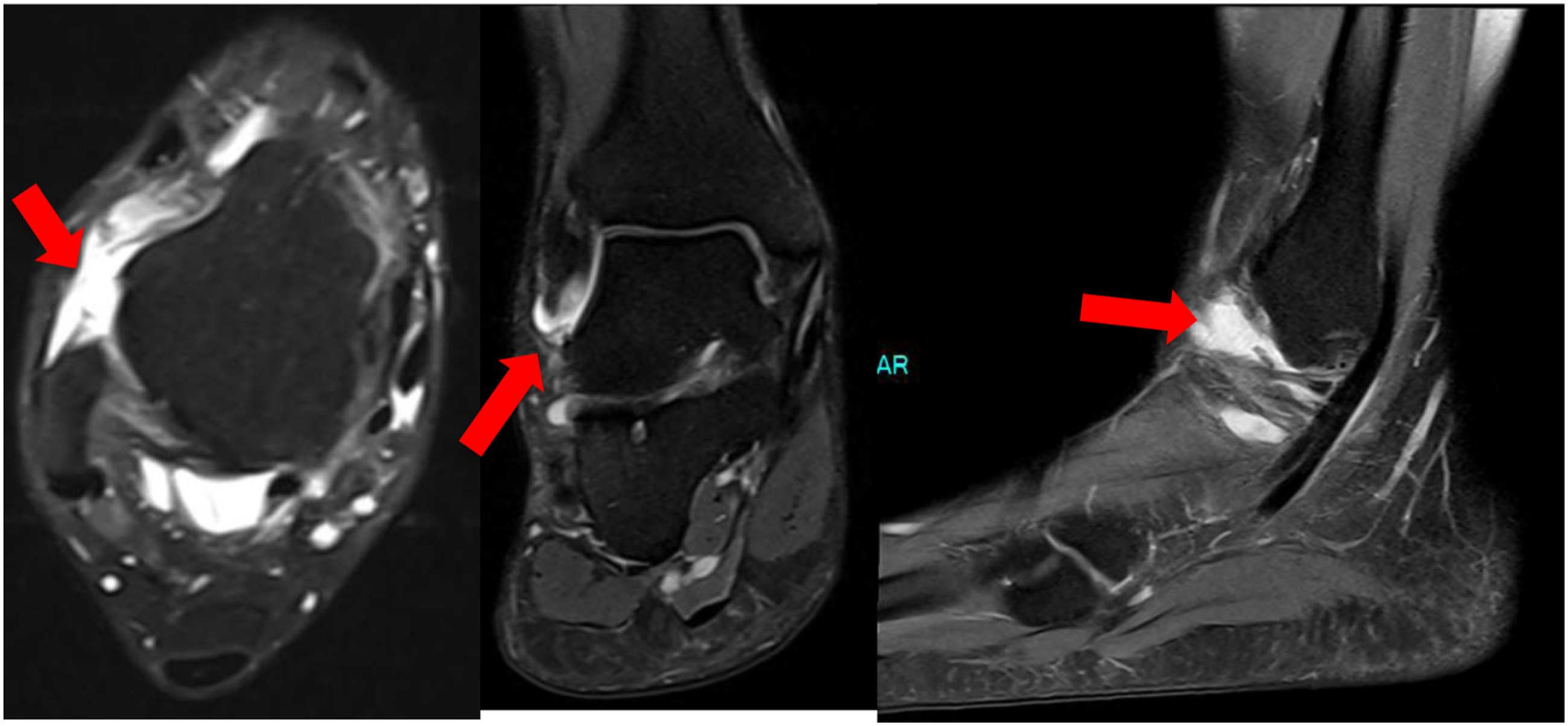
Nonoperative management
Initial treatment of acute lateral ankle sprains follows the same RICE protocols. 12 Lamb et al. 31 in 2009 conducted a multicenter randomized controlled trial, evaluating the different immobilization devices. They have concluded that a below-knee cast for 10 days resulted in more rapid resolution of symptoms and best functional outcome at 3 months follow-up. Some authors, however, do not encourage cast immobilization. Braces or ankle supports are instead recommended to facilitate early rehabilitation. Patients may be allowed full-weight bearing immediately after an injury. The importance of proper rehabilitation after an ankle sprain cannot be overemphasized, especially when the debilitating consequences of decreased range of motion, persistent pain and swelling, and chronic joint instability are considered.
After initial acute treatment, a rehabilitation protocol is essential in providing early return to activity and preventing chronic instability. Functional stress stimulates the incorporation of stronger replacement collagen. Functional rehabilitation begins on the day of injury and continues until pain-free gait and activity are attained. The four components of rehabilitation are range-of-motion rehabilitation, progressive muscle strengthening exercises, proprioceptive training and activity-specific training. Ankle joint stability is a prerequisite to the institution of functional rehabilitation.
Functional rehabilitation is initiated once range of motion is attained, and swelling and pain are controlled, the patient is ready to progress to the strengthening phase of rehabilitation. Peroneal muscles strengthening are essential in preventing ankle instability and recurrent injury. In patients with chronic ankle instability, the peroneal muscle reaction time is significantly longer to patients with no instability. 13 Strengthening begins with isometric exercises performed against an immovable object in four directions of ankle movement. The patient then progresses to dynamic resistive exercises using ankle weights and resistance bands. Resistance exercises should be performed with an emphasis on eccentric contraction. Toe raises, heel walks and toe walks may also be attempted to regain strength and coordination. Proprioceptive training is initiated as the patient achieves full weight bearing without pain, for the recovery of balance and postural control. The most common result after proprioceptive training is a lower propensity of patients to adopt ankle positions that predisposes them to injury.13–15 Use of devices with a series of progressive drills can effectively return patients to a high functional level. The simplest device for proprioceptive training is the wobble board. Having the patient perform wobble board manoeuvres at different heights and with closed eyes can advance training. When walking a specified distance is no longer limited by pain, the patient may progress to a regimen of 50% walking and 50% jogging. When this can be done without pain, jogging eventually progresses to forward, backward and pattern running. An athlete who will be returning to sports may require additional therapy from a sports therapist. Use of an orthotic device or tape, with subsequent weaning, may be recommended during the early period of activity-specific training. Even in the setting of chronic lateral ankle instability, 50% of patients still improve from a structured rehabilitation protocol. All efforts should be made prior to subjecting patients to a surgical option.16–19
Surgical management
Surgical approaches to lateral ankle instability have been categorized into nonanatomic and anatomic approaches. Non-anatomic reconstruction procedures use different configurations of local tendon grafts to accomplish the restrictive function of the ATFL without repair of the ligament remnants. Several techniques have been described, including tenodesis procedures from the Achilles tendon or peroneal tendon mimicking the function of the lateral ankle ligaments such as the Watson-Jones procedure, the modified Evans procedure and Chrisman-Snook procedure. Nonanatomic procedures most notable clinical disadvantage is the sacrifice of a normal tendon to use as a graft, which consequently may impair ankle range of motion and possibly lead to long-term degenerative changes.20,21 On the contrary, anatomic procedures are preferred to restore normal anatomy and recreate the normal joint biomechanics of the ankle.22,23 A direct lateral ligament repair depends on the quality of the ligamentous tissue. Brostrom first described the surgical technique in primary repair of ATFL and CFL. This was later modified with the Gould procedure, where reinforcement of the repair is done using the extensor retinaculum.24–26 The modified Brostrom-Gould repair is the most common procedure used for lateral ankle instability. In a meta-analysis, authors have shown nonanatomic procedures have poor clinical satisfaction. The authors hypothesized the poor outcome due to increased inversion stiffness at the subtalar level, although this statement is not well documented. Patients in this category also had more subsequent sprains. The anatomic approach showed best results with the modified Brostrom procedure. 23 Additionally, internal bracing or the use of a suture tape and/or suture anchor augmentation for lateral ligament reinforcement has also been studied. In a cadaveric study, the authors found that the Brostrom with tape augmentation group was biomechanically superior to the traditional Brostrom repair only. In a comparative study, Kulwin et al. 27 showed return to pre-injury level was faster by 4.2 weeks when the Brostrom repair is supplemented by internal brace compared to a simple Modified Brostrom technique. In recent years, arthroscopic ATFL repair has been increasing in popularity because of its minimally invasive nature and the capability to decrease patients’ recovery time and morbidity. During arthroscopy, surgeons may be able to treat intra-articular pathologies such as osteochondral lesions or impingement problems while addressing the injured ligaments. In a randomized controlled study, comparing an ‘all-inside’ arthroscopic modified Brostrom to the open technique, at 1 year after surgery there was no difference in clinical or radiologic outcomes. 28 In another study, the authors compared clinical outcomes of the open Brostrom-Gould repair to an all-inside arthroscopic Brostrom. The data showed no observable differences between the two approaches with respect to pain, American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Score and Karlsson-Peterson scores. However, the study showed that the arthroscopic group exhibited earlier time to ambulation. 29 Moreover, in the setting of revision surgery, chronic instability with poor remnants, and generalized ligamentous laxity, the use of an autograft or allograft is necessary to reconstruct the ATFL and CFL.26,30 In a comparative study evaluating clinical outcomes following Brostrom repair versus anatomic reconstruction with allograft tendons; the two groups had similar outcomes and activity levels at a minimum of 2 years follow-up, which suggests that reconstruction is a reliable option for those at risk of failure with a standard anatomic repair. 26
Author’s perspectives
There are several operative techniques in the treatment of lateral ankle instability for patients who do not respond to rehabilitation. Results, however, may vary, as there is no technique that may cater to different kinds of pathologies. The purpose of this paper is to present the author’s perspectives in the treatment of lateral ankle instability with a patient-specific approach. All patients undergo diagnostic arthroscopy. Lateral ankle instability can be associated with many intra-articular conditions such as impingement, loose bodies and osteochondral lesions of the talus. These pathologies, if left untreated, may lead to less favourable outcomes after operative stabilization of the ligament. During diagnostic arthroscopy, the ATFL quality is then assessed. Figure 3. (a). Diagnostic arthroscopy showed crustal deposits on the talar dome. (b). Osteochondral loose body. (c). Anterior talofibular ligament may be assessed using arthroscopy.
If the ligament exhibits good quality for repair, then an arthroscopic repair is done using anchor sutures. Besides the standard anteromedial and anterolateral portals, an additional accessory lateral portal is utilized. The author preferably uses two suture anchors placed at the footprint in a double row configuration and knotless technique. This offers quick recovery for patients and least morbidity. Figure 4. (a). Placing the initial anchor brings the native ligament back to its natural position. (b). A second anchor is then placed to form a double row repair configuration for added stability.
However, in cases where the integrity of the ligament is questionable, an open modified Brostrom is recommended. The open approach will allow surgeons to grasp a good cuff of the ATFL remnant, and possibly decrease the chances of surgical knot failure. In recent years, the author has also implemented internal bracing using suture tape augmentation. This additional technique allows the patients to return to pre-injury status earlier. Figure 5. (a). Placement of anchor sutures for the repair. (b). Modified Brostrom using anchor sutures with internal brace using suture tape augmentation. (c). Skin incision for this open technique.
In the setting of chronic instability with poor ligament remnants or generalized laxity, anatomic reconstruction using semitendinosus graft is utilized. The semitendinosus is used to reconstruct the ATFL and CFL. The graft is tunnelled through the fibula and fixed with tenodesis screws in the standard attachments in the talar body, calcaneus and fibula. Figure 6. Diagnostic arthroscopy prior to reconstruction. Arrow shows poor ATFL remnant.
In the author’s case series, 18 patients with a minimum follow-up of 2 years, all treated with either an open or arthroscopic repair, with eight of which had internal bracing, all had improved VAS FA and AOFAS scores. Normal gait was noted at an average of 12 days post surgery and return to pre-injury level was noted at an average of 10.2 weeks. The group with internal brace, however, showed to be more confident in ambulation earlier compared to those without suture tape augmentation. Only complication noted in this series was wound dehiscence in one patient, which was treated with oral antibiotics only. Standard accelerated rehabilitation is done for all patients. Weight bearing is immediately allowed and protected with an ankle stirrup brace for 2 weeks. Figure 7 Proprioceptive exercises are implemented at 2 weeks and light jogging allowed by the third week. Most are then allowed full sports activity after 4 weeks. Figure 8. (a). Placement of semitendinosus graft in the talar tunnel. (b). Tunnelling through the fibula for both the ATFL and CFL attachments. Arrow shows reconstructed ATFL and CFL using semitendinosus graft.

Conclusion
Lateral ankle instability is the result of recurrent lateral ankle sprains that compromise the static stabilizers of the ankle joint. This can be associated with other pathologies such as impingement or osteochondral lesions of the talus. Proper diagnosis is necessary to be able to address all lesions. The preferred initial treatment includes pain control, activity restriction, bracing and functional rehabilitation. All patients must undergo this form of management prior to any surgical procedure. The open Modified Brostrom procedure is one of the most commonly performed techniques with good results with some requiring augmentation with other methods. Although an arthroscopic approach provides several advantages, the steep learning curve with this technique may limit the utilization of this approach. By initially performing arthroscopy, one may assess the quality of the ATFL remnant and may proceed with either an all-arthroscopic or open approach. If the said remnant is non-salvageable, a reconstruction is then necessary. Surgical treatment then may be based on the patient-specific quality of the ATFL remnant.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.