
Abstract
Background
Evolving evidence and improved instrumentation have led to increasing importance of minimally invasive surgery (MIS) surgery in the treatment of hallux valgus deformity. This study aims to investigate the current trends of the practice of MIS hallux valgus surgery in the Asia Pacific region.
Method
A survey was sent via email to 30 fellowship-trained foot and ankle surgeons in 11 Asia Pacific countries, all registered with their respective national orthopaedic societies. The survey consisted of 8 questions and was designed to assess surgeon experience with MIS hallux valgus surgery, including common contraindications, satisfaction levels, learning curves and post-operative rehabilitation after MIS hallux valgus surgery.
Results
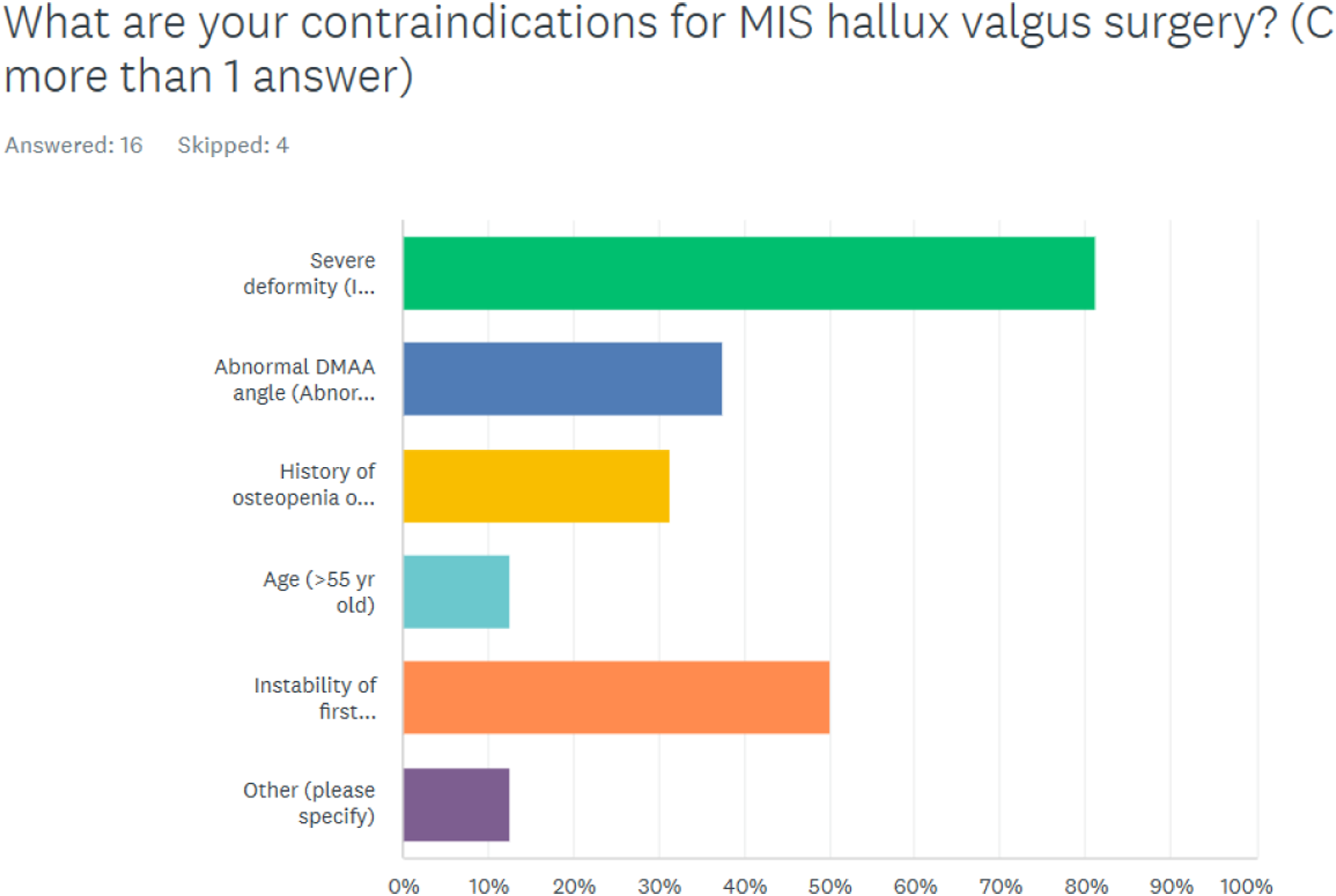
The vast majority of surgeons (63%) performed MIS hallux valgus surgery. However, only 18% of surgeons performed MIS surgery in more than half of their hallux valgus cases. A severe deformity was the most common contraindication (81%), followed by the instability of the first tarsometatarsal joint (50%), and abnormal DMAA (Distal Metatarsal Articular Angle) (38%). There was no statistically significant difference between the satisfaction score of MIS versus open surgery (p-value 0.1). The median number of cases the surgeons needed to perform before they considered themselves comfortable performing the surgery was 10 cases (range 1–100). Most surgeons allowed full weight bearing at 4–6 weeks after surgery.
Conclusions
MIS hallux valgus surgery is gaining popularity in the Asia Pacific region, with the majority of surgeons adopting this practice. The fact that severe deformity is seen as the most frequent contraindication and that MIS surgery is still not the most popular alternative demonstrates that surgeons are still circumspect when it comes to MIS surgery. Surgeons can use the findings of this study to guide their adoption of MIS practices in hallux valgus surgery and gauge well they perform in comparison to their counterparts in the Asia Pacific region.
Keywords
Introduction
Hallux valgus is a prevalent foot and ankle condition that many orthopaedic surgeons deal with. 1 In cases where nonoperative management fails, a variety of surgical techniques have been described to address the problem. 2 Recent years have seen MIS surgery (Minimally Invasive Surgery) becoming increasingly popular due to reduced recovery time, improved cosmesis and better pain management postoperatively after MIS hallux valgus surgery. 3
The practice of MIS hallux valgus surgery has evolved over a few generations. Isham et al. described the first generation, which involved a percutaneous burr being used to perform a medial closing wedge osteotomy. 4 Metal fixation was not used in this procedure. The second generation included Bösch 5 and SERI (Simple, effective, rapid, inexpensive) techniques, 6 which involved sub-capital osteotomy with percutaneous K-wire fixation.
The third generation of surgery was described by Vernois and Redfern, who popularized MICA (Minimally Invasive Chevron and Akin) osteotomy 7 involving percutaneous osteotomy and the use of percutaneous screw fixation. Several modifications were also described,8–10 including different types of osteotomy, locations of osteotomy, and the number of screws. More recently, Lewis et al. 11 published a technique on fourth generation surgery, which involved extra-articular transverse osteotomy, that enabled multidirectional deformity correction and rigid stable bicortical fixation.
MIS hallux valgus correction is traditionally popular in Europe and is increasingly gaining acceptance in the United States. 12 It remains unclear whether MIS surgery is popular in the Asia Pacific region. The purpose of this study was to investigate the current trend of the practice of MIS hallux valgus surgery amongst Asia Pacific fellowship-trained foot and ankle surgeons. We aimed to understand the popularity, common contraindications, satisfaction levels, learning curve, and post-operative rehabilitation after MIS surgery.
Methods
A survey (Supplemental Material) was sent via email to 30 fellowship-trained foot and ankle surgeons registered with their respective national orthopaedic societies in the Asia Pacific region. The survey was sent in December 2022 and a reminder email was sent in January 2023. The survey consisted of 8 questions and was designed to assess surgeon experience and satisfaction with MIS surgery. MIS hallux valgus surgery was defined as percutaneous surgery with percutaneously inserted burr instead of saws. This definition included techniques of any generation of MIS hallux valgus surgery. The definition of MIS hallux valgus surgery and the purpose of the survey were made known to the survey participants, and any questions from participants were clarified via email reply. The survey participation was entirely voluntary and the results were anonymous. Since there was no direct patient involvement in the survey, ethics approval was not necessary.
There was an equal representation of surgeons from different countries in the Asia Pacific region. The countries included are India, China, South Korea, Japan, Australia, Thailand, Hong Kong, Malaysia, Singapore, Philippines, and Indonesia. Surveymonkey.com was used to collate the data. Multiple choice questions and visual analogue scales were used to gather surgeon responses. Statistical analysis was done using Excel software. Nominal and ordinal data were shown in percentage and absolute count. Mean and standard deviation were used for normally distributed data, while median and range were used for non-normally distributed data. T-test was used to compare means from two different groups.
Results
A positive response was obtained from 20 out of 30 surgeons who were contacted, with a response rate of 67%. Most surgeons in our study focused their practice primarily on foot and ankle surgery. 9 out of 20 (45%) of them had 75% of their practice in foot and ankle surgery, and 5 out of 20 (25%) of them had 100% of their practice in this subspecialty (Diagram 1). The majority of the surgeons did perform MIS hallux valgus surgery, with 63% of them answering “yes” to the question of whether they performed MIS hallux valgus surgery (Diagram 2). What proportion of your practice is foot and ankle surgery?. Do you perform MIS hallux valgus surgery?.

However, only a small number of surgeons performed MIS surgery in more than 50% of their hallux valgus surgical cases. Only 18% (3 out of 17 surgeons) performed between 50 to 100% of their hallux valgus cases with the MIS techniques (Diagram 3). A severe deformity was the most common contraindication (81%), followed by the instability of the first tarsometatarsal joint (50%), abnormal DMAA (Distal Metatarsal Articular Angle) (38%), history of osteopenia (31%), and age > 50 year old (13%) (Diagram 4). In hallux valgus surgery, what is the proportion of cases you perform MIS surgery?. What are your contraindications for MIS hallux valgus surgery?.
For open hallux valgus surgery, the preferred option was Scarf osteotomy for most surgeons, with 14 out of 20 surgeons (70%) choosing Scarf osteotomy over other options (Diagram 5). The mean satisfaction score for MIS surgery was 7.6 (SD 1.4) while the mean satisfaction score for open surgery was 8.4 (SD 0.9). There was no statistically significant difference between the satisfaction score of MIS versus open surgery (p-value 0.1). The median number of MIS valgus surgery cases the surgeons needed to perform before they considered themselves comfortable performing the surgery was 10 cases (range 1–100). Most surgeons (41%) allowed full weight bearing at 4–6 weeks after surgery (Diagram 6). For open hallux valgus surgery, which is your preferred option?. When do you allow full weight bearing after MIS surgery?.

Discussion
A number of studies of MIS hallux valgus surgery had been published by surgeons in the Asia Pacific region.13–17 These studies were done in recent years which showed the increasing popularity of MIS surgery in the region. This trend is consistent with the outcome of our survey, where the majority (63%) of the respondents did perform MIS surgery. However, only 3 out of 17 respondents performed MIS surgery in most of their hallux valgus surgical cases. Most surgeons in Asia Pacific do have MIS surgery as part of their armamentarium, but this technique is still not the most widely used procedure in the region.
There is good evidence of the benefits of MIS surgery in other foot and ankle surgeries. Grassi et al. 18 in a meta-analysis of MIS Achilles tendon repair showed significantly reduced postoperative complications especially wound infection and were more likely to report a good or excellent subjective outcome in the MIS group. A meta-analysis of arthroscopic ankle fusion 19 showed improved fusion rate and lower complications in arthroscopic ankle fusion than open ankle fusion. The benefits and outcomes of MIS surgery in hallux valgus correction are still up for debate. Lewis et al. 20 in a prospective study with 2 years follow up found MIS surgery provided significant improvement in clinical outcomes with a low rate of recurrence. A randomized study by Lee et al. 21 showed that the MIS group had less pain in the first 6 weeks post-operatively and comparable outcomes in comparison to an open group at the final follow-up. Another randomized study by Kaufmann 22 revealed the outcome of MIS surgery was comparable to that of open surgery 5 years after treatment. These results were consistent with the response rate of our survey, which showed similar satisfaction scores of MIS and open surgery amongst Asia Pacific foot and ankle surgeons.
The role of MIS surgery in severe deformity is still controversial. Bia et al. 23 did a review of 1534 MIS procedures and concluded the main indication was mild deformities. Another review by Singh et al. 24 found MIS surgery provides satisfactory outcomes for mild to moderate deformity, and the outcomes were not as good as open surgery. In contrast, other studies demonstrated good results even for severe deformity. 25 Lewis et al. 26 in a study of MIS surgery in severe deformity found substantial deformity correction and improved clinical outcomes at 2-years follow-up. Castellini 27 in another study of MIS surgery in moderate to severe deformities discovered significant improvements in clinical and radiographic parameters at a minimum 12-months follow-up. Our study showed most surgeons in the Asia Pacific still viewed severe deformity (81%) as a contraindication for MIS surgery. This finding is potentially explained by the more cautious and traditional view of Asia Pacific surgeons with the adoption of MIS practices for hallux valgus surgery.
Increased DMAA is classically a problem with congruent hallux valgus deformity. 28 Correction of increased DMAA in hallux valgus surgery often needs meticulous pre-operative planning and selection of the appropriate osteotomy. Several authors had studied the use of MIS surgery in correcting DMAA. Frigg et al. 29 reported better DMAA correction in MIS surgery compared to open Scarf/Akin surgery. Brogan et al. 30 in a cohort study comparing MIS to open surgery found a trend favouring MIS surgery in DMAA correction. Only 38% of the surgeons in our survey indicated abnormal DMAA as a contraindication for MIS surgery, indicating the majority of the surgeons were still confident that MIS surgery could be used in cases with abnormal DMAA.
A learning curve exists when a surgeon learns a new surgical technique and this phenomenon is present in most foot and ankle procedures. 31 MIS hallux valgus surgery is not spared. Several studies were done to assess the number of surgeries a surgeon performed before achieving competency. These studies used operative duration and radiation exposure to determine competency. It was found that surgeons needed to perform 27 to 38 cases before he or she achieved competency.32,33 Our survey showed the surgeons in Asia Pacific perceived the median number of cases needed was 10 cases. This finding may reflect the lack of awareness of the steep learning curve surgeons have to go through to achieve competency. Bedi et al. 34 discussed good tips on how to shorten the learning curve, which included cadaveric training, attention to detail, and self-reflection.
Post-operatively, Vernois and Redfern advocated immediate weight bearing in a flat shoe or heel-bearing shoe. There was similar practice by other authors who also performed third generation MIS surgery, 35 and the rationale was third generation surgery provides more stability to the osteotomy site. However, most surgeons in our survey only allowed weight bearing at 4–6 weeks after surgery. The definition of MIS surgery in our survey included any generation of MIS surgery and therefore, there may be potential worries of unstable fixation, resulting in delayed weight bearing.
There are a few limitations of our study. To begin, this study is survey-based and hence reflects only the opinions of the survey participants and not necessarily the actual trend of practice and agreement of MIS techniques in general. The response rate of the survey is 67% and the group of non-responders may represent non-believers in MIS surgery. There was also no segregation of MIS techniques into different generations. We hope to capture the overall trend of MIS surgery utilization in the region and therefore did not segregate the surgery into specific generations. Furthermore, multiple modifications of third-generation surgery and the recent description of fourth generation surgery make the segregation of MIS techniques into individual generations more confusing and as a result, we may lose important input from the respondents.
With newer evidence and techniques, MIS surgery has a growing importance in the treatment of hallux valgus deformity. It is gaining popularity in the Asia Pacific region with the majority of surgeons performing MIS surgery. The fact that severe deformity is seen as the most frequent contraindication and that MIS surgery is still not the most popular alternative demonstrates that surgeons are still circumspect and traditional when it comes to MIS surgery. Surgeons may use the findings of this study to guide their adoption of MIS practices in hallux valgus surgery and gauge how well they are performing in comparison to their peers in the Asia Pacific region.
Supplemental Material
Supplemental Material Perspectives and trends for minimally invasive surgery for hallux valgus deformity in the Asia Pacific region
Supplemental Material for Perspectives and trends for minimally invasive surgery for hallux valgus deformity in the Asia Pacific region by Chin Yik Tan and Gowreeson Thevendran in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.