
Abstract
Background
In complete brachial plexus injury, phrenic nerve (PN) is frequently used in neurotization for elbow flexion restoration. The advancement in video-assisted thoracoscopic surgery (VATS) allows full-length PN dissection intrathoracically for direct coaptation to recipient without nerve graft.
Purpose
We report our experience in improving the surgical technique and its outcome.
Methods
Seven patients underwent PN dissection via VATS and full-length transfer to musculocutaneous nerve (MCN) or motor branch of biceps (MBB) from June 2015 to June 2018. Comparisons were made with similar group of patients who underwent conventional PN transfer.
Results
Mean age of patients was 21.9 years. All were males involved in motorcycle accidents who sustained complete brachial plexus injury. We found the elbow flexion recovery were earlier in full-length PN transfer. However, there was no statistically significant difference in elbow flexion strength at 3 years post-surgery.
Conclusion
We propose full-length PN transfer for restoration of elbow flexion in patients with delayed presentation.
Background
The surgical treatment for complete brachial plexus injuries is complex and challenging. The neurotization procedure is preferred in early presentation and the main objective is restoration of elbow flexion.1–4 Extraplexal donor nerves are always used to transfer to the musculocutaneous nerve (MCN) as intraplexal nerves are not suitable. 3 The technique of phrenic nerve (PN) transfer was introduced in 1989 by Gu et al. and they reported good motor recovery. 5 Generally, the motor recovery of elbow flexion, Medical Research Council Grade ≥3 (MRC ≥3) occurs at an average of 9.5 months post-surgery in PN transfers to MCN.5,6
Phrenic nerve exploration is quite direct as it lies on the anterior surface of the scalene anterior, easily found during supraclavicular dissection. 2 It has a large number of motor axons making it a suitable donor; in fact superior to other donors.5,7,8 The biceps motor recovery (MRC ≥3) is comparable with that in other potential donors e.g,. intercostal nerves (ICN) and spinal accessory nerve (SAN) transferred to MCN. 3 There is concern about pulmonary function as the ipsilateral diaphragm is paralysed in PN transection but many authors claim that it is a safe procedure with rare early respiratory symptoms 9 and no long term complications.5,10 Zheng et al. and Zheng et al. reported no respiratory symptoms and normal pulmonary function in their long term outcome study of PN and two to three ICN staged neurotization procedure.4,11 Some authors reported minimal impairment of lung function which returned to normal within 9 months 10 to 2 years3,5 without respiratory symptoms.
The disadvantage of using the PN as donor is the available length for transfer. Anatomically, we are aware that the thoracic portion of PN is quite long. If we could dissect it totally from its insertion at the diaphragm, we could coapt it to the MCN or motor branch of biceps (MBB) directly without graft. Conventionally, the nerve is transected at the supraclavicular region, and there is frequently an 8 cm discrepancy to reach the origin of the MCN, thus requiring interpositional nerve graft. 3 Nerve grafts undergo ischaemic changes prior to nerve regeneration, 12 thus, axonal regeneration would take a longer time. 10 If full-length PN direct coaptation to MCN is done, the starting point of regeneration would be transferred distally by 8 cm. 7 Thus, the reinnervation of biceps is predicted to be faster and motor function is expected to be earlier. In addition, the axonal loss would only occur at one coaptation site.7,12
Lijie et al. and Xu et al. described a possible technique to obtain the whole length of PN for neurotization via video-assisted thoracoscopic surgery (VATS).7,10 An extra length of 12–16 cm intrathoracic portion was obtained and this allowed coaptation to MCN without tension.7,10 According to Xu et al. the only clinical paper found in the literature, the biceps strength as restored to MRC 3 within 198.8 days compared to 378.2 days in conventional nerve transfer; approximately 6 months earlier. 10 This finding is significant and would be beneficial in patients with late presentation or neglected brachial plexus injuries.
Video-assisted thoracoscopic surgery has been reported as a safe procedure without many complications.7,10 It is minimally invasive, so early and better recovery of wounds is expected. 10 However, it is technically demanding, 3 requiring dedicated cardiothoracic surgery team involvement. Ipsilateral complete lung collapse is required during VATS and double-lumen endotracheal tube intubation is needed; requiring a dedicated anaesthetic team care. In our centre, we have good support from both teams.
The purpose of this study is to compare the recovery of elbow flexion and long term outcome of full-length PN transfer versus conventional PN transfer to MCN or MBB. We believe that the VATS technique can be improved and would like to share our experience which could be useful in future treatment of brachial plexus surgery.
Surgical technique: VATS aided PN dissection
The procedure
Patients lied supine and double-lumen tube intubation with general anaesthesia was performed. Then, patients were positioned lateral during cleaning and draping, subsequently, placed supine again. A sandbag was placed under ipsilateral scapula to keep the neck in extension and lateral deviation (rotation). Two teams of Upper Limb/Microsurgeons dissected the neck and arm simultaneously. The supraclavicular dissection was done to explore and identify the PN (found on anterior surface of scalene anterior), suprascapular nerve; SSN (found under the omohyoid muscle, first branch from erb’s point) and SAN (found anterior to anterior border of trapezius). The mid arm dissection was done to identify MCN, specifically the MBB (found directly under biceps brachii). Both donors; the PN and SAN were stimulated with a nerve stimulator. Upon positive response, the cardiothoracic team was called.
Ipsilateral lungs were collapsed by the anaesthetist. Patients were placed lateral and a sterile support was placed at patients’ sacrum. Video-assisted thoracoscopic surgery was performed with a 5 mm 30-degree high definition camera (Karl Storz) used for visualization of the thoracic cavity and its structures. A single portal was created at the fifth intercostal space along the anterior axillary line and the pleural surfaces, lung and diaphragm were inspected for any abnormality. The PN was identified along its whole length from the thoracic inlet down to the diaphragm. The mediastinal pleura just superior to the lung hilum was then incised to expose the PN. Gentle blunt dissection around the nerve with a right-angled forceps allowed a vascular loop to be passed for gentle retraction during dissection. The nerve was then dissected off the mediastinum from the root of the neck down to the diaphragm with a Harmonic scalpel® (Ethicon Endosurgery).
Once dissection was completed, the nerve was stimulated at the neck to confirm that it was still functioning. This was a crucial step; to confirm that no damage had occurred during dissection. Then, the nerve was detached flush at the diaphragm with the Harmonic scalpel®. The nerve was then dissected at the thoracic inlet and gently delivered proximally out from the thoracic cavity with the aid of the thoracoscope.
Passing the PN at thoracic inlet
At the thoracic inlet, the nerve must be freed under the clavicle. Early on in our experience, we tried using a plastic cannula creating a slot on the side and used it as a blunt dissector. However, during the third VATS, this was not possible. It took longer with more blood loss to retrieve the nerve proximally. Later, we noticed a small nerve branch from PN tethered under the clavicle (unsure insertion).
These branches were consciously looked for and cut in all subsequent patients, to aid smooth passage of the PN, proximally.
Length of the intrathoracic PN
We realized that there was discrepancy between the right (Figure 1(a)) and left (Figure 1(b)) PN lengths. The right PNs were shorter probably because the nerve courses straight down to the diaphragm along the medial chest mediastinum whereas the left PN traverses the cardiac border. Phrenic nerve (a) Right; reaches proximal arm only and (b) Left; reaches mid arm.
Thus, we coapted the right PN directly to the MCN, making it a longer distance that the axons were required to grow, with some axons being deviated to the brachialis and also to the lateral cutaneous nerve of the forearm. We were able to coapt the left PNs directly to the MBB. The difference between the lengths of the right and left PN was previously reported. 13
Chest tubes were inserted via the same thoracoscopic portal. Patient was turned supine again. Two Upper Limb/Microsurgeons joined the surgery again to prepare the nerves for coaptation; SAN to SSN and full-length PN to MCN/MBB simultaneously end-to-end coaptation under magnification with Nylon 8-0 with tissue glue. The PN was tunnelled subcutaneously to reach the recipient. About 1 cm of the tip was resected as we were concerned about the thermal injury during intrathoracic resection from the diaphragm. The wound was washed and skin was closed in layers.
In the ward, the chest tube was removed after 2 days. Wound dressings were changed and arm sling applied for support. All patients underwent the same physiotherapy for passive range of motion and brain mapping protocol.
Methods
This is a prospective observational study; comparison was made between full-length PN transfer (dissected via VATS) and conventional PN transfer (via sural nerve graft) to MCN or MBB to restore elbow flexion in complete brachial plexus injury patients.
All patients who were diagnosed with complete brachial plexus injury were planned for neurotization procedure if recovery was not seen within 3 months. The diagnosis was made clinically. We performed SAN to SSN for shoulder abduction/stabilization and PN to MCN or MBB for elbow flexion; simultaneously. The function of PN was tested pre-operatively from clinical examination, chest radiographs and sniff test. 14 Patients with concomitant chest injuries, history of chest tube insertion and lung diseases were excluded from this study. Written informed consent was obtained from all patients who agreed to participate in this study. The study had been approved by local medical research ethics committee (MREC Number: 2021222-9860).
Outcome of full-length phrenic nerve (PN) transfer for restoration of elbow flexion in complete brachial plexus injury.

Outcome of conventional phrenic nerve (PN) transfer for restoration of elbow flexion in complete brachial plexus injury.

Data analysis was done with SPSS Version 26.0 software (SPSS, Inc., Chicago II). Descriptive analysis was performed for demographic data and pre-operative findings. Comparison between the two groups; categorical and continuous data were analyzed with Fisher’s exact test and independent-samples t-test respectively. A p-value of less than 0.05 was considered as statistically significant.
Results
Comparison between full-length phrenic nerve (PN) transfer and conventional phrenic nerve (PN) transfer for restoration of elbow flexion.

All patients were males in both groups.
aFisher’s exact test was used in all categorical data.
bSignificant difference between two groups (p < 0.05).
Both groups showed good improvement in power of elbow flexion at 3 years post-surgery. In full-length PN transfer group, there were three patients in MRC 3 and two patients achieved MRC 4 whereas in conventional PN transfer group, there were five patients who achieved MRC 3. Two patients from each group did not achieve good recovery of biceps. The mean strength of elbow flexion achieved at 3 years follow up were MRC 3 in both groups.
Early recovery of elbow flexion (MRC ≥1) was noticed earlier in full-length PN transfer; mean duration 10.5 (SD 6.27) months post-surgery (range, 4.9–23.3 months). In conventional PN transfer, the mean duration was 14.0 (SD 6.01) months post-surgery (range, 6.5–25.8 months). The difference was not statistically significant, however clinically this finding is significant as the nerve regeneration must occur before the irreversible motor end plate degeneration occurs.
At 6 months post-surgery, the conventional PN transfer showed poor recovery. Only one patient had biceps flexion MRC 1. The full-length PN transfer group had better recovery with one patient achieving MRC 2 and two patients achieved MRC 1. We found the recovery of elbow flexion was earlier in full-length PN transfer compared to the conventional PN transfer.
In general, the motor recovery of biceps was slow in both groups. Interestingly, two patients with the earliest recoveries of their biceps function (MRC ≥1) were seen in full-length PN transfer; 4.9 and 5.8 months and both were non-smokers. The delay in recovery in other patients could be contributed by the effect of smoking.
There was no major complication encountered during both procedures. None of the patients complained of respiratory symptoms. However, the duration of hospital stay in full-length PN transfer was longer; mean duration 4 days compared to conventional PN transfer; 2 days. This difference was statistically significant (p < 0.05). Those patients had to be monitored longer for chest tube care and drainage.
Discussion
Neurotization procedures for brachial plexus injuries are evolving; many improved and promising techniques have been described. Best outcome with early motor recovery is seen in younger patients, distal nerve injuries and early surgical intervention. 15 Early neurotizations are recommended for motor restoration as it is crucial to reinnervate the motor endplates before irreversible atrophy/degeneration occurs.15,16,17 Grinsell and Keating quantified the duration of denervation within 12–18 months. 16 Ray et al. suggested neurotization surgeries within 6 months of trauma and a maximum delay of 1 year. 15 Some authors suggested neurotizations within 4 months of trauma as ideal, with the best outcome. 12 Chuang et al. suggested 5 months post-trauma and mentioned the worst results are seen if neurotization surgery is done after 1 year. 18 In our centre, we counselled patients for neurotization if there was no significant recovery of elbow flexion within 3 months. This would accommodate for preparation of surgery and patients’ decision, thus, surgery can be done within 4 months; the ideal time suggested by Liu et al. 12
In view of the slow nerve regeneration of 1–2 mm per day, 16 direct coaptation of donor nerves to nerve branch nearest to target muscles is ideal. 1 Therefore, a direct PN (motor nerve with more than 800 myelinated motor axons) 15 transfer to MBB (without graft) should have good outcome theoretically. However, almost 16 cm of PN length is intrathoracic. 7 The full-length PN transfer to MBB was possible with the advancement of VATS. The procedure requires skill and a dedicated team. The intrathoracic PN is loosely attached to many vital structures like pericardium and superior vena cava, which are at risk of bleeding if damaged during dissection. 7 Post-operatively, patient would need chest tube and longer hospital stay. In our study, there was a significant difference in duration of hospital stay.
We found a similar study published recently which concluded that supraclavicular PN transfer had better results compared to VATS aided PN transfer for restoration of elbow flexion in brachial plexus injuries. 19 However, this study was a comparison made between two medical centers and it was not mentioned if the surgeons’ level of expertise were comparable. There were too many variables for target nerve coaptation in supraclavicular PN transfer group and some were sutured directly without nerve graft. This could have contributed to the better outcome.
In our study, the early recovery of elbow flexion in full-length PN transfer compared to conventional PN transfer is clinically significant. This would particularly benefit the group of patients who present late to medical centres. Sadly, there is still lack of awareness of brachial plexus injuries in many countries and many patients often present to hospital after exhaustion of alternatives. We usually do not perform neurotization as we are aware of poor prognosis in delayed presentations. With this technique, late neurotization is an option as we expect early nerve regeneration before permanent motor endplate degeneration occurs.
In general, there was a delay in recovery of elbow flexion after both the PN transfer groups in our study. Interestingly, we found that our best outcomes were among the full-length PN transfer group who are non-smokers. There is no strong evidence to support the adverse effects of smoking with outcome of neurotization. A few authors reported a decrease in recovery rate and poor outcome post-neurotization.20,21 In addition, smokers tend to have higher pain scores post-operatively. 22
There were two patients in each group who did not achieve good recovery of elbow flexion. Intraoperatively, we noticed that their biceps muscles were pale and severely fibrosed. Probably, they had concomitant vascular injury during the trauma which affected the nerve regeneration and muscle healing. Thus, it affected the motor recovery of elbow flexion. However, we did not investigate further for vascular trauma prior to surgery.
Lijie et al. forbade the use of diathermy close to the nerve and even cut the insertion with the use of clips. In our case, the harmonic scalpel undoubtedly speeded up the procedure. 7 The nerve function was also tested immediately prior to transection, so we were assured of no immediate damage. However we did not look into subsequent propagating damage in the time following the procedures, as we deemed this much less likely. Furthermore, a very long graft with inadequate blood supply may be equivalent to a graft as central necrosis is commonly reported. 23
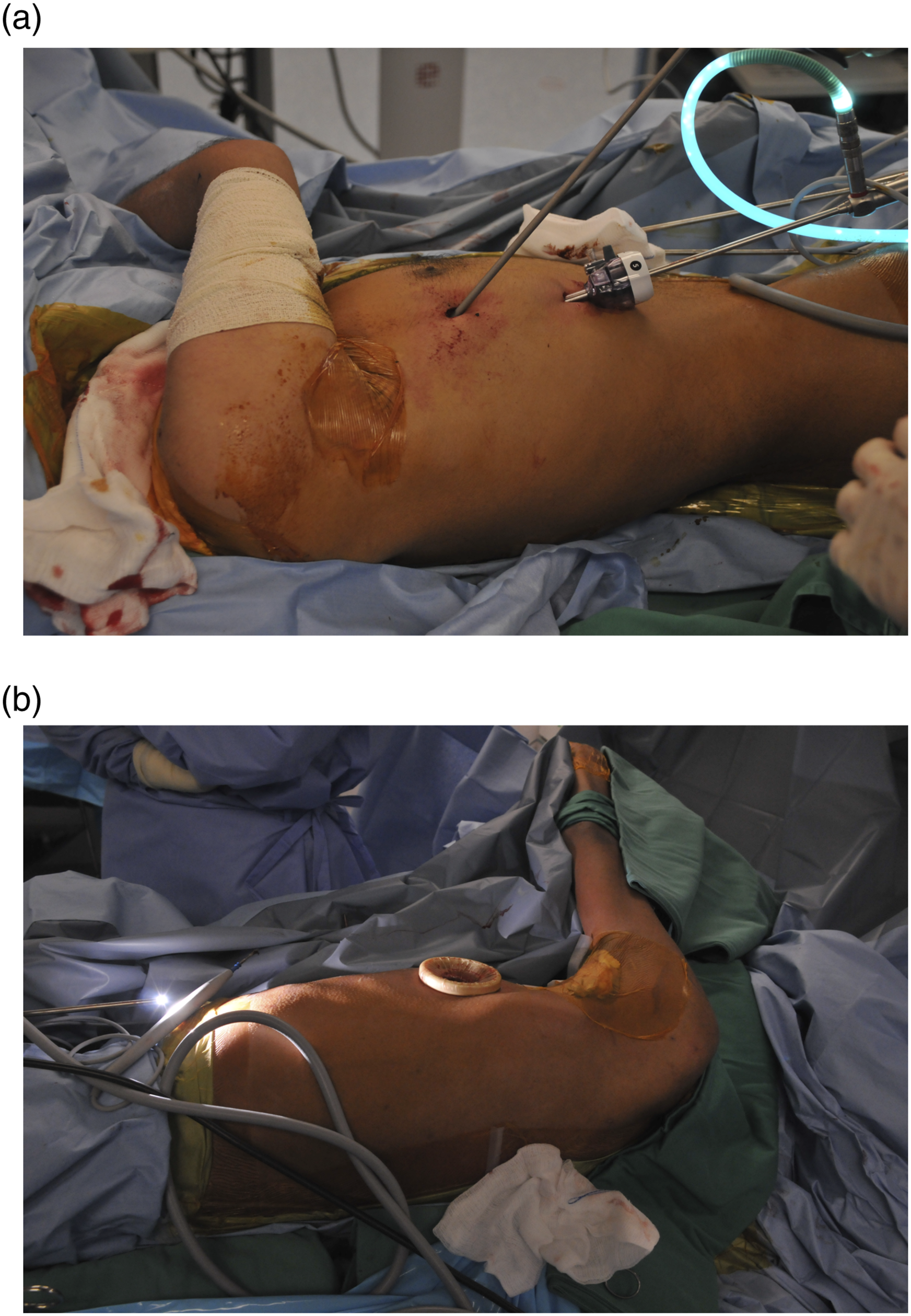
Recommendations or tips for VATS: 1. Perform VATS aided PN dissection in lateral position. It was easier to manipulate the thoracoscopic instruments and took a shorter time. (Figure 2(a) and 2(b)) 2. Due to discrepancy in left and right PNs, left PNs (longer) can be coapted to MBB and right PNs (shorter) to MCN. This will aid in initial exploration and preparation of recipients. 3. The Harmonic scalpel was preferred for dissection as it increased the speed of dissection, hemostasis and significantly reduced the risk of bleeding.
24
The heat generated from an ultrasonic scalpel is no more than 100°C with minimal lateral thermal spread.
25
It has been shown that the temperature 1 cm away from the tip of the harmonic scalpel does not rise to more than 42°C.
26
The tip of the distal end of the PN is usually excised 1 cm prior to coaptation. The nerve function was tested before final resection. 4. The PN must be explored under the clavicle for its branches and resected free. The risk of bleeding is higher at the thoracic inlet region as the PN is between the subclavian vein and artery with its first branch; internal mammary artery.
7
5. The whole PN should be kept in visual field during instrumentation. We had a case of left PN dissection which got entangled and damaged at its insertion. About 5 cm of its tip had to be sacrificed but the length was sufficient to coapt at MCN. 6. Exclude all patients with chest trauma. Patients with previous chest injuries may have pleural adhesions which may prevent lung collapse
7
which is crucial prior to VATS. 7. Watch out for approximity of pericardium at left PN and superior vena cava at the right PN. (a) Patient in lateral position with two port incisions and (b) uniportal technique (preferred technique).
Limitation of this study is the small sample size and inadequate for statistical analysis. A randomized control study would have been better than this prospective study. However, considering the incidence of complete brachial plexus injuries in our country and strict inclusion criteria, we could not randomize the samples. Universal sampling was carried out. Pulmonary function was not done in any patients as they had no respiratory symptoms. Furthermore, most of the evidence in the literature mentioned that lung function returned to normal due to the presence of accessory PNs 3 and other elements of the cervical plexus. 5
Conclusion
Early recovery of elbow flexion is possible with direct full-length PN transfer to MCN or MBB; intrathoracic PN dissection done via VATS. This procedure would benefit the patients with delayed presentation. We predict good outcome in carefully selected patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.