
Abstract
Purpose
Biomechanical study of fixation methods post hallux valgus minimally invasive osteotomy using finite element technology hasn’t been reported. This study aimed to compare maximum displacement and stress distribution of osteotomy ends after minimally invasive osteotomy fixed by bandage, Kirschner wire, Herbert screw.
Methods
Foot CT images of a patient with mild-moderate hallux valgus were collected. Three-dimensional finite element model of hallux valgus was established through CT image. This study simulated bandage, Kirschner wire and Herbert screw fixation, and analyzed maximum displacement and stress distribution of osteotomy ends in plantar flexion position of foot after fixation.
Results
Maximum equivalent stress of osteotomy end fixed with bandage, Kirschner wire, Herbert screw was 7.8615, 14.253, 8.3156 MPa, respectively. Total displacement of osteotomy end fixed by bandage, Kirschner wire, Herbert screw was 0.26,896, 0.022,779, 0.029,195 mm, respectively. Maximum stress of Kirschner wire and Herbert screw near osteotomy end was 154.7 and 46.404 MPa, respectively. Fixation strength and stability of Kirschner wire and Herber screw were better than bandage. Kirschner wire had stress concentration phenomenon, with potential fracture risk. Stress of Herbert screw was evenly distributed around osteotomy end, and there was a certain stress concentration, playing an important role in maintaining fracture end stability.
Conclusions
Herbert screw showed good fixation strength and stability, and stress distribution was uniform, which can well maintain stability of minimally invasive osteotomy ends. Findings of this study would provide a theoretical basis for selection of fixation methods after clinical minimally invasive osteotomy for hallux valgus.
Introduction
Hallux valgus is one of the common deformities of foot deformity, which mostly occurs in women, and the incidence rate is about 10%.1,2 The main clinical manifestations of hallux valgus are that the first metatarsophalangeal joint of hallux valgus deviates outward, the hallux valgus angle is larger than the physiological hallux valgus carrying angle of normal human body, and some patients have slightly outward rotation deformity of hallux valgus at the same time. 3 There are many factors leading to hallux valgus, mainly including heredity, flat feet, long-term wearing of high heels and so on. 4 Mild hallux valgus can be treated conservatively, 5 but patients with moderate to severe hallux valgus or whose symptoms have not been reduced after conservative treatment will be treated surgically. 6
With the development of medical technology, minimally invasive surgery for hallux valgus is widely used, 7 however, the choice of minimally invasive surgical fixation is still controversial. At present, the “wrapped curtain” fixation (using “8” bandage and split toe pad to fix the osteotomy end after minimally invasive valgus surgery), represented by Wen’s operation, 8 is widely used, and there are many postoperative clinical reports. However, there is no relevant report on the biomechanical comparison between “wrapped curtain” fixation and internal fixation represented by Kirschner wires and Herbert screws.
Based on the finite element method, this study aimed to analyze and compare the biomechanical characteristics of three different fixation methods (bandage, Kirschner wire and Herbert screw) after minimally invasive osteotomy for hallux valgus.
Patients and methods
Study design and patients
This study (design) was a static biomechanical experiment. This study involved one patient with hallux valgus who was treated in our hospital on 10 February 2022. This hallux valgus patient is a 28-year-old female with a height of 167 cm and a body weight of 60 kg. The hallux valgus angle (HVA) of the patient’s left foot was 25°, and the first and second metatarsal angles (IMA) were 12°. The proximal articulator set angle (PASA) was 5°, and the distal articulator set angle (DASA) was 6°. After physical examination and inquiry, we learned about other foot deformities and foot surgery history of this patient. During the examination, the radiation was strictly protected to prevent injury to patient.
Imaging data collection
The left foot of the patient was scanned with 64 slice spiral CT (Model: SOMATOM definition edge, Siemens, Erlangen, Germany), and the CT images were obtained. The sectional imaging data was output and saved in the DICOM format.
Establishment of a three-dimensional finite element models of adult hallux valgus
Establishment of a three-dimensional finite model of adult hallux valgus
The DICOM format data obtained from CT were imported into the Mimics 21.0 software (Materialise, Leuven, Belgium). The bones and other soft tissues were recognized according to the gray values with CT scanning, and the corresponding three-dimensional model was preliminarily established. The calcaneus, talus and other bones were exported to the STL format model data files respectively, and then the data files were imported into the Geomagic software 2017 (Geomagic Inc., Shanghai, China) for surface treatment to optimize the model characteristics and establish cortical bone and cancellous bone. Then, the data files were imported into the SolidWorks 2017 (Dassault Systemes S.A., Concord, MA, USA) for normal assembly. Finally, the ANSYS meshing was imported to establish an effective analysis file, and the preliminary model of hallux valgus was obtained (Figure 1(a)). In this study, the 2.5 mm of mesh size was selected for meshing the solid model for finite element analysis. Establishment of adult hallux valgus minimally invasive osteotomy model. a. Preliminary model of hallux valgus in adult. b. The established details of the adult hallux valgus minimally invasive osteotomy model.
Establishment of adult hallux valgus minimally invasive osteotomy (SEIR osteotomy) model
Osteotomy was generated at about 2 cm inside the proximal end of the metatarsal head. The osteotomy line on the sagittal plane formed an angle of 10° with the vertical line of the metatarsal axis, and the osteotomy line on the horizontal plane formed an angle of 15° with the vertical line of the metatarsal axis. Two intersecting osteotomy lines on the sagittal plane and horizontal plane were established as a plane, and this plane was used as the segmentation plane to segment the metatarsal bone. The distal end of the osteotomy was translated from inside to outside, and the thickness of one bone cortex was about 3 mm 9 in the direction of the osteotomy surface, so as to obtain an adult hallux valgus minimally invasive osteotomy model (Figure 1(b)).
Establishment of Kirschner wire fixation model of adult hallux valgus minimally invasive osteotomy
The 1.5 mm Kirschner wire was selected in this study. In order to facilitate the experimental research, the Kirschner wire was simplified as two parallel fixation with 1.5 mm cylinder perpendicular to the osteotomy surface (Figure 2(a)). Adult hallux valgus minimally invasive osteotomy Kirschner wire (a) and Herbert screw (b) fixation model.
Establishment of Herbert screw fixation model of adult hallux valgus minimally invasive osteotomy
In this study, a 3 mm diameter Herbert screw was selected. In order to facilitate the study, the Herbert screw was simplified as a cylinder and fixed perpendicular to the osteotomy plane (Figure 2(b)).
Element division and material parameter assignment
Material properties of bone and screws.

Determination of the contact boundary conditions and loads
The friction coefficient of the contact among the upper surface of the support structure, the plantar surface and the osteotomy was set to 0.6, and the contact friction coefficient of other joints was set to 0. 15 The friction coefficient of the contact between Kirschner wire and bone was set to 0.2. 16 The contact between screw and bone was defined as “tie” constraint. 17 According to the equivalent exchange principle of load and ground reaction force, the concentrated force was applied to the pressure center through the support structure. The upper surface of talus was fully restrained, and the ankle joint was in the neutral position when standing in balance. The proximal end of the first metatarsal osteotomy was set as the fixed end, and the distal end of the osteotomy was the free end.
After minimally invasive osteotomy of the first metatarsal neck in a 60 kg hallux valgus patient, the displacement and stress of osteotomy end were recorded when the extreme metatarsal flexion was fixed with bandage toe splitting pad, Kirschner wire and Herbert screw, respectively. When standing on both feet, one foot of the model bears half of the weight, about 300 N.
18
Referring to previous literature, the muscle force affecting the first metatarsal column was assumed to be parallel to the longitudinal axis of the first metatarsal and 50% of the reference value, about 319.5 N (Figure 3(a)).
19
The forces of the bandage and the split toe pad were decomposed into forces perpendicular to the phalanx and parallel to the longitudinal axis of the first metatarsal bone. The force of the bandage model was divided into 4.89 N perpendicular to the phalanx and 24.35 N parallel to the first metatarsal bone. In this study, it was expressed in the form of load in the finite element model (Figure 3(b)).
20
The simulation of the first plantar muscle force model (a) and simulation of the bandage split toe pad force model (b).
Main observation indicators
Three coordinate axes (namely X axis, Y axis and Z axis) perpendicular to each other were established by take a point in space as the origin of the coordinate system. The X axis was horizontal, the Y axis was vertical, and the Z axis was horizontal with the foot plane. The Z axis was perpendicular to the horizontal plane and located above the toe. Under the above constraints and loading conditions, the von Mises stress of osteotomy end, Kirschner wire and Herbert screw, and the displacement and total displacement of X, Y and Z axes were calculated.
Results
Kirschner wire and Herbert screw displayed higher fixation strength
The results showed that the maximum equivalent stress at the osteotomy end of bandage (Figure 4), Kirschner wire (Figure 5) and Herbert screw (Figure 6) was 7.8615, 14.253 and 8.3156, respectively, among which the Von Mises stress of Kirschner wire was the largest (Table 2). Therefore, the Kirschner wire and Herbert screw displayed higher maximum equivalent stress and fixation strength than the bandage. Graphs of the Stress nephogram (a) and displacement diagram (b) at the end of osteotomy with bandage fixation. Graphs of the Stress nephogram (a) and displacement diagram (b) at the end of osteotomy with Kirschner wire. Graphs of the Stress nephogram (a) and displacement diagram (b) at the end of osteotomy with Herbert screw. Von Mises stress and displacement of osteotomy end, Kirschner wire and Herbert screw.



Kirschner wire and Herbert screw showed good fixation stability
The displacement of osteotomy end showed that the total displacement fixed by Kirschner wire (Figure 5, 0.022779 mm) and Herbert screw (Figure 6, 0.029195 mm) was obviously smaller than that fixed by bandage (Figure 4, 0.26896 mm) (Table 2). Therefore, from the perspective of the stability of minimally invasive osteotomy end, the fixation stability of Kirschner wire and Herbert screw was significantly better than that of bandage fixation. Meanwhile, there were no displacement differences between Kirschner wire and Herbert screw (Table 2). Therefore, both of the Kirschner wire and Herbert screw can show good fixation stability.
Herbert screw demonstrated good osteotomy end stability
By observing the stress nephogram of Kirschner wire (Figure 7(a)) and Herbert screw (Figure 7(b)), it can be seen that the stress distribution of Kirschner wire was uneven, and the stress near the distal end of the osteotomy end was the highest (154.7 MPa), with obvious stress concentration and potential fracture risk. The stress of Herbert screw was evenly distributed around the osteotomy end, and the maximum stress (46.404 MPa) was reached at the osteotomy end. The uniform stress concentration of Herbert screw played a good role in maintaining stability of the osteotomy end. Von Mises stress nephogram of Kirschner wire (a) and Herbert screw (b).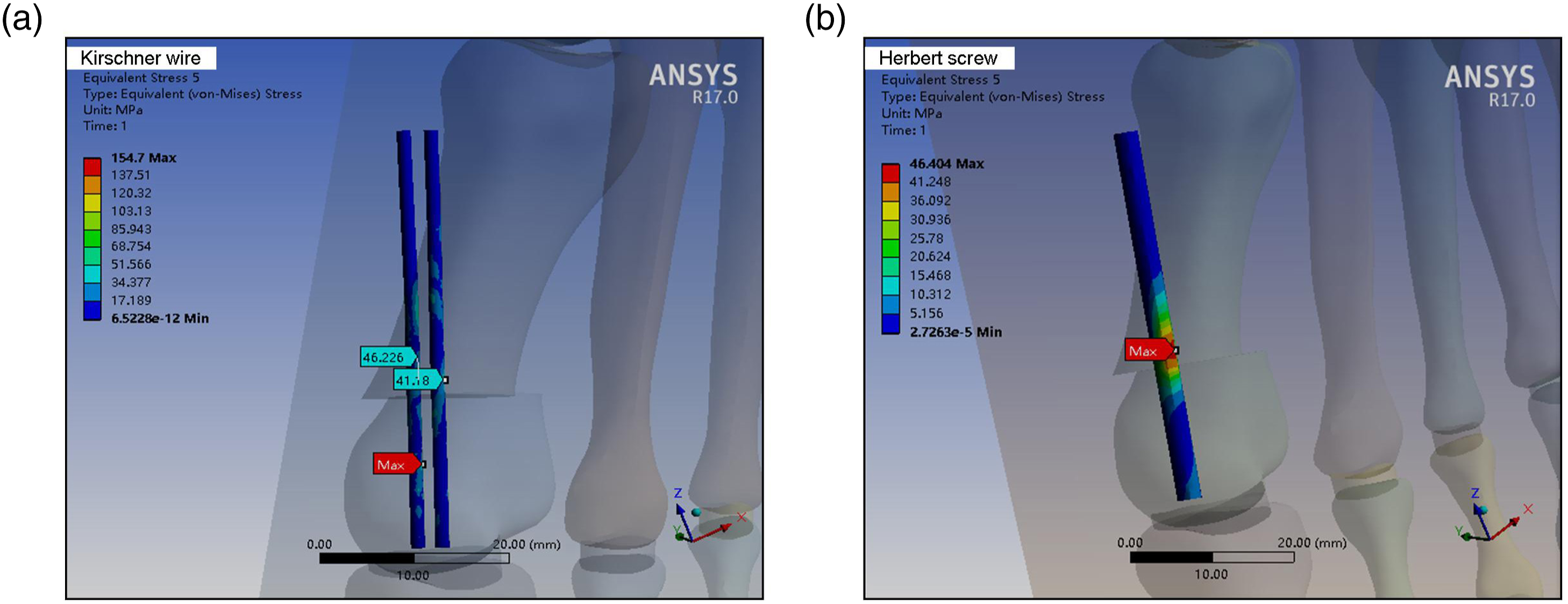
Discussion
With the development of minimally invasive technology, minimally invasive treatment of hallux valgus is being widely carried out. However, there is still a lot of controversy about the choice of its fixation method, especially the bandage split toe pad fixation method is questioned by many scholars. 8 After long-term follow-up, the satisfaction rate of bandage toe pad fixation method has reached a high level. 21 However, there are relatively few reports on the comparative analysis of bandage split toe pad fixation, Kirschner wire and screw fixation, especially in the biomechanical analysis. The development of finite element technology provides a very good means for the study of clinical biomechanics. 22 Therefore, three-dimensional finite element technique was used to compare and analyze the biomechanical characteristics of the osteotomy end of hallux valgus after minimally invasive osteotomy.
In this study, we only modeled the cortical bone and cartilage model, but did not model ligaments, muscles, and soft tissues. Initially, the cancellous bone was considered when establishing a three-dimensional model, but the previous references10,11 mentioned that both cortical bone and cancellous bone can be considered to have linear elastic behavior under quasi-static loading. Therefore, cortical bone and cancellous bone are not classified, but all material properties of bone mineral are used. Therefore, to maintain consistency with the literature and ensure the accuracy of the article, it is agreed to remove cancellous bone. In this study, about 2 hours were used to complete one simulation, and the variation is related to the specific model and the number of computer programs running at that time. From the results of finite element model calculation, the fixation strength of Kirschner wire (14.253 MPa) and Herbert screw (8.3156 MPa) was greater than that of bandage split toe pad (7.8615 MPa). The previous studies23,24 have confirmed that within the physiological range, exerting certain pressure on the fracture end has an obvious inducing effect on the repair of fracture. Therefore, from the perspective of osteotomy end healing, the higher stress of Kirschner wire and Herbert screw can more effectively stimulate osteotomy end healing. However, the stress distribution diagram at the osteotomy end showed that the stress of Kirschner wire fixation occurred locally, and the maximum stress occurred in the dorsomedial side, which was related to the friction and bending moment between Kirschner wire and bone. The withdrawal of Kirschner wire and other phenomena during clinical follow-up may be related to the above effects. By comparing the displacement of osteotomy end, we found that the total displacement fixed by Kirschner wire (0.022,779 mm) and Herbert screw (0.029,195 mm) was significantly smaller than that fixed by bandage (0.26,896 mm). From the perspective of the stability of minimally invasive osteotomy end, the fixation stability of Kirschner wire and Herbert screw was significantly better than that of bandage fixation, and the displacement difference between Kirschner wire and Herbert screw was very small, which showed that they can achieve the same level of fixation stability. Although Kirschner wire fixation could provide good stability, it remained outside the skin for a long time, which put forward higher requirements for postoperative care. At the same time, the indwelling of Kirschner wire also increased the risk of potential infection and involved secondary removal surgery, which increased the pain and economic burden of patients. 25 Herbert screw fixation not only had bidirectional compression effect, but also could maintain good fixation stability. The end of Herbert screw could be embedded in bone without taking it out, which avoided the pain of secondary surgery. Herbert screw fixation could still achieve good fixation effect for patients with poor medical compliance, allowing patients to move in a large range, which was conducive to early functional recovery. In this study, the osteotomy end did not move much due to bandage fixation, which was consistent with previous reports. 25 The displacement of bandage fixation mainly occurred in the X-axis (0.2689 mm). It can be seen that the displacement of osteotomy end mainly occurred in the horizontal position. The displacement in this direction was allowed by the treatment concept. According to Kenwright et al.’s report 26 and other studies, when the relative displacement between fracture ends was 0.5–1 mm, the intensity of ossification at the fracture site increased and the speed of ossification accelerates. In this study, the total displacement of bandage fixation was less than 0.5 mm, which had no adverse effect on the healing of osteotomy end and could achieve the result of secondary healing. However, after the bandage was fixed, the patient needed to regularly go to the hospital for reexamination and replacement of the bandage, which would affect the healing of the osteotomy end and the medical compliance of the patient. According to the stress nephogram of Kirschner wire and Herbert screw itself, the stress distribution of Kirschner wire was uneven, and the stress near the distal end of the osteotomy end was the highest, reaching 154.7 MPa, with obvious stress concentration and potential fracture risk. However, the stress of Herbert screw was evenly distributed around the osteotomy end, and the maximum stress (46.404 MPa) was reached at the osteotomy end. Actually, when endowing the material contact relationship, this study considered that the Kirschner wire is a smooth object and does not have the effect of pressure unlike the Herbert screw. Therefore, the friction coefficient was set as the reference document of 0.2, so there is local stress concentration after the application of the load, resulting in large stress data. Therefore, this study adopted the point method to better present the real data of Kirschner wire and defined the maximum stress over 150 MPa. This uniform stress concentration played a good role in maintaining the stability of the osteotomy end.
Actually, in clinical work, we use the Herbert screw with biphasic compression effect, which can also effectively prevent the rotation of the osteotomy end after fixation. We not only use one screw, but also use Kirschner wire or bandage for hallux valgus surgery. With regard to your question about bandage and Kirschner wire fixation, we have carried out relevant clinical cases in our clinical work (Supplementary Figure 1). Furthermore, the solid model cannot be directly used for finite element calculation, so it needs to be meshed to generate a finite element model. The finite element model is a mathematical representation of solid structure and material. In ANSYS, the solid model can be divided by elements to generate the finite element model. The above process is called the meshing of the solid model. In essence, the meshing of the solid model is to divide the solid model into many sub-regions with one cell. These sub-areas have attributes, that is, set material cell attributes. In this study, 2.5 mm of mesh size was selected for meshing solid model for finite element analysis. Actually, the mesh size here is the most suitable mesh for the current model after selecting the optimal finite element mesh according to the previous medical finite element experience and adjusting and dividing the mesh several times. The selected mesh is the size with relatively uniform stress change. When the mesh size is 2.5 mm, the model changes most uniformly under the stress, so this size is selected. In addition, the finite element model can also be directly generated by using elements and nodes.
This study does not do validity verification and grid convergence, which has certain limitations in data. The limitation lies in the accuracy of the data. Model validation and grid convergence can greatly ensure that the difference in data size is not significantly different from reality. If not done, accuracy will decrease. Based on past experience, this study can ensure that accuracy rate is above 80%. However, although there are differences in accuracy rate of data size, there is no error in inter group comparison. Because each group has a similar error, it can be judged that even if the data size error is large, the inter group comparison will not be affected, and the rule of results will not be affected. Therefore, although this study has not been validated, it has considerable accuracy.
Conclusion
Based on the CT images of hallux valgus patients, three-dimensional finite element technology was used to simulate and analyze the biomechanical characteristics of three different fixation methods after minimally invasive osteotomy for hallux valgus (Figure 8). This study found that Kirschner wire and Herbert screw were better than bandage fixation in fixation strength and stability, but there was no significant difference between Kirschner wire and Herbert screw. Meanwhile, bandage fixation had no adverse effect on the secondary healing of the osteotomy end. Bandage fixation had higher requirements for the medical compliance of patients, and there was a potential risk of fracture of Kirschner wire. However, on the premise of ensuring good fixation strength and stability, Herbert screw allowed patients to have a wider range of activities, which was more conducive to the functional recovery of patients after surgery. This study had some simplification in the model design, which might affect the accuracy of the data and would become the focus of future research. The finding of this study will provide theoretical basis and reference for the selection and optimization of fixation methods after clinical minimally invasive osteotomy for hallux valgus. The experimental design flow chart of the biomechanical characteristics comparison among three different fixation methods after minimally invasive osteotomy for hallux valgus.
Supplemental Material
Supplemental Material - Three dimensional finite element analysis of biomechanics of osteotomy ends with three different fixation methods after hallux valgus minimally invasive osteotomy
Supplemental Material for Three dimensional finite element analysis of biomechanics of osteotomy ends with three different fixation methods after hallux valgus minimally invasive osteotomy by Qiang Xie, Xiaodong Li and Pei Wang in Journal of Orthopaedic Surgery
Footnotes
Author contributions
Qiang Xie and Pei Wang conceived the work, interpreted the data, and substantively revised the work. Pei Wang designed the work and substantively revised the work. Qiang Xie and Xiaodong Li analyzed and interpreted the data. Qiang Xie drafted the work. All the authors approved the submitted version and agreed to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This patient signed the informed consent and informed the risk, before the examination. The research plan was approved by the Ethics Committee of the Affiliated Hospital of Chengde Medical College (Approval No. LL090).
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available, but are available to be provided privately on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.