
Abstract
Purpose
Complete meniscus root tear is associated with meniscus extrusion; this causes a loss of meniscus function and accelerated osteoarthritis of the knee. Existing small-scale retrospective case–control studies suggested that the outcomes were different between medial and lateral meniscus root repair. This meta-analysis aims to study whether such discrepancies exist via a systematic review of the available evidence in the literature.
Methods
Studies evaluating the outcomes of surgical repair of posterior meniscus root tears, with reassessment MRI or second-look arthroscopy, were identified through a systematic search of PubMed, Embase, and Cochrane Library. The degree of meniscus extrusion, healing status of the repaired meniscus root, and functional outcome scores after repair were the outcomes of interest.
Results
Among the 732 studies identified, 20 studies were included in this systematic review. 624 knees and 122 knees underwent MMPRT and LMPRT repair, respectively. The amount of meniscus extrusion following MMPRT repair was 3.8 ± 1.7 mm, which was significantly larger than the 0.9 ± 1.2 mm observed after LMPRT repair (p < 0.001). Significantly better healing outcomes were observed on reassessment MRI after LMPRT repair (p < 0.001). The postoperative Lysholm score and IKDC score was also significantly better after LMPRT than MMPRT repair (p < 0.001).
Conclusions
LMPRT repairs resulted in significantly less meniscus extrusion, substantially better healing outcomes on MRI, and superior Lysholm/IKDC scores, when compared to MMPRT repair. This is the first meta-analysis we are aware of that systematically reviews the differences in the clinical, radiographic, and arthroscopic results of MMPRT and LMPRT repair.
Introduction
The meniscus is an essential structure that facilitates the efficient load bearing capabilities of the knee. 1 It increases the contact surface area between the articular surfaces of the femur and tibia, thereby reducing the contact pressure. In the absence of the meniscus, a 50% reduction in the tibiofemoral contact area and a 200% increase in peak contact pressure was observed. 2
The meniscus is attached to the tibia through the anterior and posterior insertional ligaments at its anterior horn and posterior root. 3 Upon weightbearing, the axial forces along the tibiofemoral joint compress the meniscus. In the presence of intact roots, hoop stresses are generated within the circumferentially oriented collagen fibers of the meniscal body. 4
Meniscus root injuries are defined as radial tears that occur within 9 mm of the meniscus root attachment, or bony avulsions of the insertional ligament. 5 Complete tears of the root hinder the ability of the meniscus to generate hoop stress, and thus causes meniscal extrusion. 6 It was shown that the biomechanical impact of complete root tear was equivalent to total meniscectomy. 7 Meniscus extrusion reduces the effective contact area between the articular surfaces, thereby increasing the resultant stress placed on the articular cartilage. It was identified as an independent predictor of tibiofemoral cartilage loss, with studies showing a greater rate of medial tibiofemoral cartilage volume loss in patients with meniscus extrusion (extrusion versus no extrusion: −1.4%/year; p < 0.05). 8
Although the medial and lateral meniscus share many similarities in structure and function, there are anatomical differences between the two. To name a few, the medial meniscus is attached at its peripheral rim to the joint capsule along its entire length, whereas the attachment of the lateral meniscus is discontinued at the region of popliteus tendon; the medial meniscus is attached to the body of the deep medial collateral ligament, but a similar relationship does not exist between the lateral meniscus and the lateral collateral ligament; the meniscofemoral ligaments (Ligament of Humphrey and Ligament of Wrisberg) serve as additional bony attachments for the posterior horn of the lateral meniscus, but similar structures are absent in the medial side. 3
Differences in the presentation of medial and lateral meniscus root tears can be observed.9,10,11,12 Patients presenting with medial meniscus root tear are often middle-aged and elderly subjects; the cause of the tear is believed to be degenerative in origin. 9 On the other hand, the etiology of lateral meniscus root tear is often traumatic in origin. It is more commonly found in young active individuals. Many of them also suffered from concomitant anterior cruciate ligament injury. 10 A discrepancy can also be seen between the reported preoperative meniscal extrusion between medial root tears (3.77 mm) 11 and lateral meniscus root tears (0.73 mm). 12 However, it remains unknown whether the anatomical differences between the medial and lateral meniscus lead to the differences seen above.
It was also noted that the postoperative radiological findings of medial meniscus root repair differed from that of lateral meniscus root repair.11,13 Chang et al. reported a residual meniscus extrusion of 3.69 mm following medial meniscus root tear repair, 11 whilst Zhuo et al. 13 reported 0.63 mm of meniscus extrusion after lateral meniscus root tear repair. Although previous meta-analyses have studied either medial or lateral meniscal root repair,11,14,15,16,17,18,19,20,21,22,23,24,25 there are currently no meta-analyses, we are aware of, that compare the demographics, presentations, clinical outcomes, and radiological results, between medial meniscus posterior horn root repair and lateral meniscus posterior horn root repair.
The purpose of this systematic review is to study whether there are differences in the presentation of posterior horn root tear between the medial and lateral meniscus; and whether the results of meniscus root repair differ between the two sides. It is hypothesized that there is no difference between the medial and lateral meniscus regarding the presentation of root tear, and the results after surgical root repair. The primary outcome is the degree of residual meniscus extrusion on post-operative reassessment MRI. The secondary outcomes include the presentation of meniscus root tear (i.e., demographics and cause of tear), healing status of meniscus root repair, short-term clinical results, and long-term radiological results.
Methodology
Study selection
Types of studies
A systematic review comparing the results of medial and lateral meniscus root posterior repair was performed. We included randomized controlled trials and cohort studies comparing medial and lateral meniscus posterior root repair, and case series concerning the surgical repair of either medial or lateral meniscal posterior root tear.
Types of participants
Participants were included in the study if they were treated with surgical repair of either a medial meniscus posterior root tear or lateral meniscus posterior root tear.
Types of interventions
We included studies that involved either meniscus-to-meniscus (mid-substance repair) or meniscus-to-bone repair (transtibial pullout or suture anchor). Studies with a mixture of different surgical repair methods were included if we were able to extract data on the participants that underwent any of the repair methods listed above.
Types of outcome measures
The degree of residual meniscus extrusion after surgical repair, and the change in meniscus extrusion on MRI were primary outcomes of interest for our study. Secondary outcomes of interest included the patient’s preoperative demographics and radiological status, meniscal healing status on reassessment MRI and/or reassessment arthroscopy, clinical outcomes at a minimum of 1-year follow-up, and reoperation rates.
Inclusion and exclusion criteria
Studies that met the following inclusion criteria were subject to full-text review: (1) Surgical repair of the posterior meniscus root tear; (2) postoperative evaluation of surgical outcomes by MRI or Arthroscopy. The exclusion criteria were as follows: (1) technical notes; (2) animal studies; (3) biomechanical studies; (4) abstract only articles; (5) review articles; (6) meta-analyses; (7) non-English language. No ethical approval was necessary for the present study as all data were based on previously published studies and anonymized.
Literature search
Electronic bibliographic databases
We searched the following databases up to 8 March 2022: PubMed database (from 1996), Embase (from 1947), and the Cochrane Library (from 1994). The following keywords were used: (“meniscus” OR “meniscal”) and (“repair”) and (“root”) and (“tear”).
Reference checking
We checked the reference lists of existing systematic reviews and meta-analyses for further relevant literature.
Data collection and analysis
Selection of studies
Two review authors independently screened the abstracts, keywords, and publication type of all articles obtained from our described literature searches. After the initial screening process, the full-text articles of studies that were possibly eligible for inclusion were obtained and assessed using the inclusion and exclusion criteria. Any uncertainties or disagreements were resolved by discussion.
Data extraction
The same two reviewers extracted data from each included study using a predefined data extraction form. The following data were collected from each of the included studies: residual meniscus extrusion on reassessment MRI (mm), change in meniscus extrusion (post-operation minus pre-operation, mm), age, sex, body mass index (BMI), causes of the tear, presence of history of injury, mean duration of surgery from injury, mean duration of follow-up, degree of preoperative osteoarthritis (in terms of Kellgren-Lawrence classification), lower limb alignment, surgical repair technique (mid-substance repair, transtibial pull out suture, suture anchor), use of biological method (e.g. microfracture, fibrin clot) to augment the healing of meniscal repair, meniscal healing status on reassessment MRI, meniscal healing status on reassessment arthroscopy, definition of meniscal healing on MRI and second-look arthroscopy, post-operative Tegner activity score and functional score (e.g. International Knee Documentation Committee (IKDC) score, Lysholm knee score), and any repeated operations (other than repeated meniscus surgery and second-look arthroscopy; e.g., high-tibial osteotomy, total knee arthroplasty). Any uncertainties or discrepancies in judgement were resolved by discussion amongst the reviewers.
Statistical analysis
All the data was initially extracted into an electronic spreadsheet (Microsoft Excel). For subgroup meta-analyses, continuous variables were extracted as means and standard deviations. If these variables were missing in the articles, the authors did not include these studies into the meta-analysis. Nominal outcomes were pooled as prevalence, and the total numbers from each study were calculated using the Chi-square test. A p value of less than 0.05 was interpreted as statistically significant. All Meta-analyses and Chi-square test calculations were calculated using IBM SPSS Statistics Software Version 27.0.1.0.
Assessment of bias
The two reviewers independently assessed all included studies using the ROBINS-I (Risk Of Bias In Non-randomized Studies of Interventions) checklist, which is an instrument designed to evaluate the risk of bias (RoB) in non-randomised studies that compare the health effects of two or more interventions. 26 On this checklist, authors must determine the RoB in seven different study domains, ranking the degree of risk according to the pre-determined ROBINS-I criteria. The study domains assessed include bias due to (1) confounding, (2) participant selection, (3) intervention classification, (4) deviations from the intended intervention, (5) missing data, (6) outcome measurements, and (7) selection of the reported result. Each of these domains are labelled as “low”, “moderate”, “serious”, or “critical” risk based on the checklist published by ROBINS-I. The RoB in all seven domains must then be accounted for to reach an overall RoB judgment for each paper.
Results
Identification of studies
An electronic search of the PubMed, Embase, and Cochrane Library databases yielded 728 studies (Figure 1). The references of relevant systematic review and meta-analyses were checked for any additional relevant articles, yielding four additional studies for screening. Out of the 732 studies screened, 325 duplicates were excluded. An additional 372 studies were excluded after screening of the abstracts, which left 35 studies remaining for full-text review. Of these, 15 were excluded through our study’s selection criteria. Ultimately, 20 studies were included in this systematic review (Table 1). Prisma Flow Diagram. General characteristics of the included studies. LOE = level of evidence; TP = transtibial pull-out; SA = suture anchor; PM = partial meniscectomy; MSR = mid-substance repair

Literature search
Of the 20 included studies, only one retrospective case–control study compared the results of medial and lateral meniscus posterior root repair. 27 15 studies assessed the outcomes of medial meniscus root tear repair,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42 and four studies assessed the outcomes of lateral meniscus root tear repair.12,13,43,44 No randomized controlled trial was identified.
Two studies evaluated the outcomes of more than one repair technique; Kim et al. compared the outcomes of transtibial pull-out repair against suture anchor repair for medial meniscal posterior root tear, 33 and Okazaki et al. 43 compared transtibial pull-out repair to mid-substance repair for lateral meniscal posterior root tears. Therefore, amongst the 20 studies there were a total of 23 cohorts of meniscus root repair. Further details regarding the demographic data, level of evidence, surgical repair method, and post-operative regimen are described in Table 1.
Patient characteristics
Baseline Demographics and surgical data of study patients.

Values are expressed as mean±standard deviation
Meta-Analysis
Chi-square test ns non Significant
The causes of the tear was reported to be degenerative in three studies (all on medial meniscus posterior horn root repair) 27,39,40; and traumatic in 10 studies (including five studies on medial meniscus posterior horn root repair 29,31,32,33,35 and five studies on lateral meniscus posterior horn root repair ).12,13,27,43,44 The cause of the tear was not mentioned in the remaining eight studies.28,30,34,36,37,38,41,42 All of these eight studies were reports on medial meniscus posterior horn root repair.
Among the 10 studies stating that the cause of the tear was traumatic in origin, data on time between injury and surgery was available in five (3 studies on lateral meniscus posterior horn root tear12,43,44 and two studies on medial meniscus posterior horn root tear29,31). The mean time of surgery from injury was 497 days in lateral meniscus posterior horn root repair and 85 days in medial meniscus posterior horn root repair.
Concerning lower limb malalignment, data was found in 11 studies concerning repair of medial meniscus posterior horn root tear,29,30,31,32,36,37,38,39,40,41,42 but none on the lateral meniscus counterpart. To summarize, varus lower limb malalignment was reported to be present in only one study. 36 Varus malalignment was either an exclusion criteria29,31,32,36,39,41,42 or an indication for concomitant high tibial osteotomy30,34,40 in the remaining publications.
Surgical repair technique
Amongst the 624 knees (17 cohorts) with a medial meniscus root tear, 559 knees (89%), 36 knees (6%), and 29 knees (5%) underwent a transtibial pull-out repair, suture anchor repair, and mid-substance repair, respectively. None of the patients with a lateral meniscus root tear (122 knees) underwent a suture anchor repair; however, 58 knees underwent a transtibial pull-out repair and the remaining 64 knees received a mid-substance repair. A majority of the medial meniscus posterior root repairs were conducted at the meniscus-bone interface (either by transtibial pull-out suture or suture anchor; 95%). Conversely, 48% of lateral meniscus root repairs were performed at the meniscus-bone interface; the remaining 52% underwent mid-substance repair. Concomitant anterior cruciate ligament reconstruction was performed in only 0.3% of medial meniscus root repairs, 31 as compared to 91% in lateral meniscus root repair.12,13,27,43,44
There was no description of the use of biological method to augment meniscus healing (including fibrin clot and microfracture) in 16 studies.12,27,28,29,30,31,32,33,34,35,36,38,39,40,43,44 Among the remaining four studies, Ulku et al. 41 reported using fibrin clot and Zhu et al. 42 reported using microfracture as biological augments of medial meniscus posterior horn root repair. The last two studies reported information concerning microfracture. One study utilized microfracture as a treatment for grade 3 or four chondral lesion, but not as an augment for meniscus healing. 37 In the last study, 13 concomitant microfracture was considered as an exclusion criteria.
Meniscus extrusion on reassessment MRI
Meta-analysis of results of posterior root tear repair.
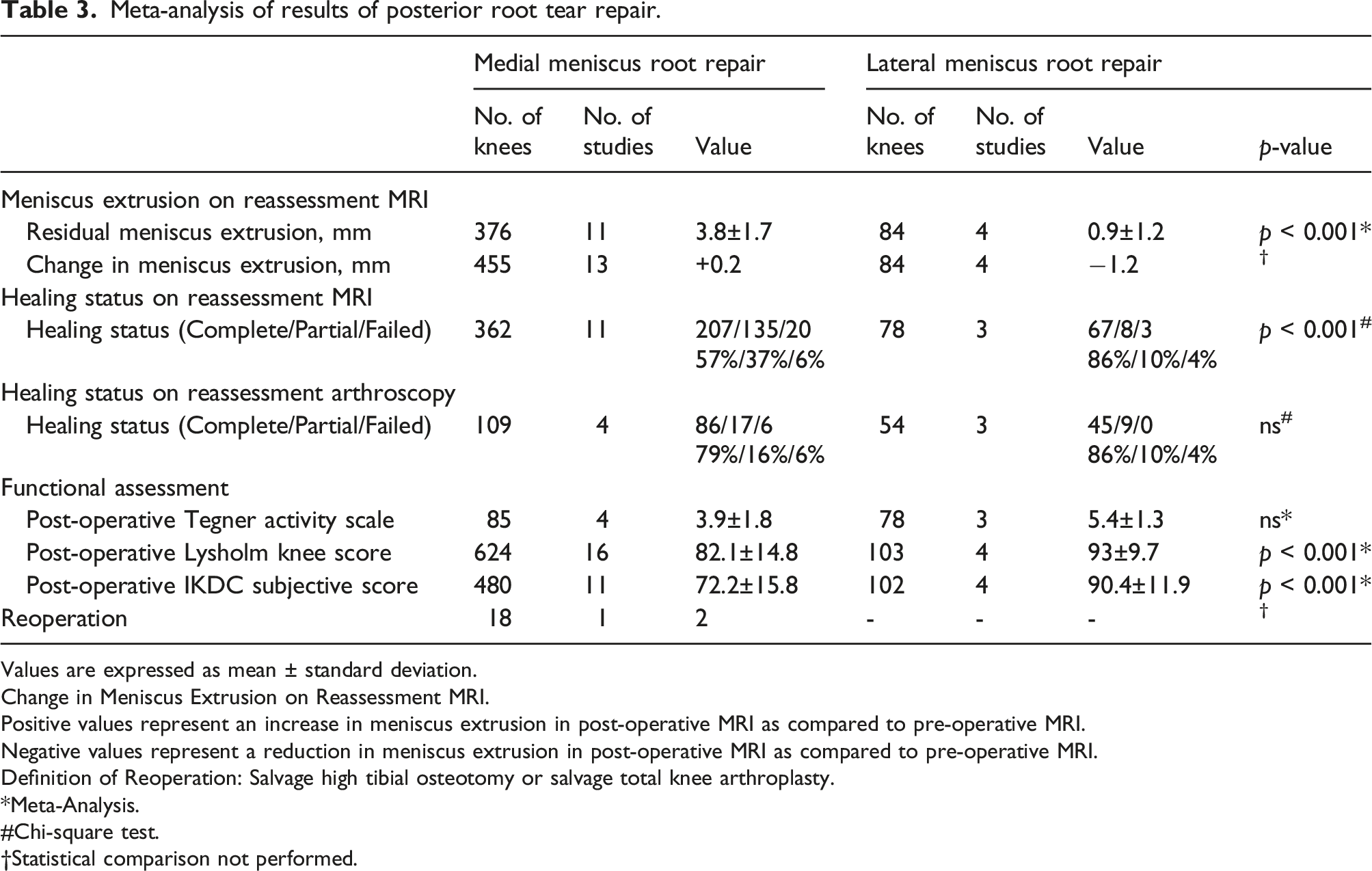
Values are expressed as mean ± standard deviation.
Change in Meniscus Extrusion on Reassessment MRI.
Positive values represent an increase in meniscus extrusion in post-operative MRI as compared to pre-operative MRI.
Negative values represent a reduction in meniscus extrusion in post-operative MRI as compared to pre-operative MRI.
Definition of Reoperation: Salvage high tibial osteotomy or salvage total knee arthroplasty.
Meta-Analysis.
Chi-square test.
Statistical comparison not performed.
Healing status on reassessment-MRI
Methods of assessment of healing of meniscus repair.
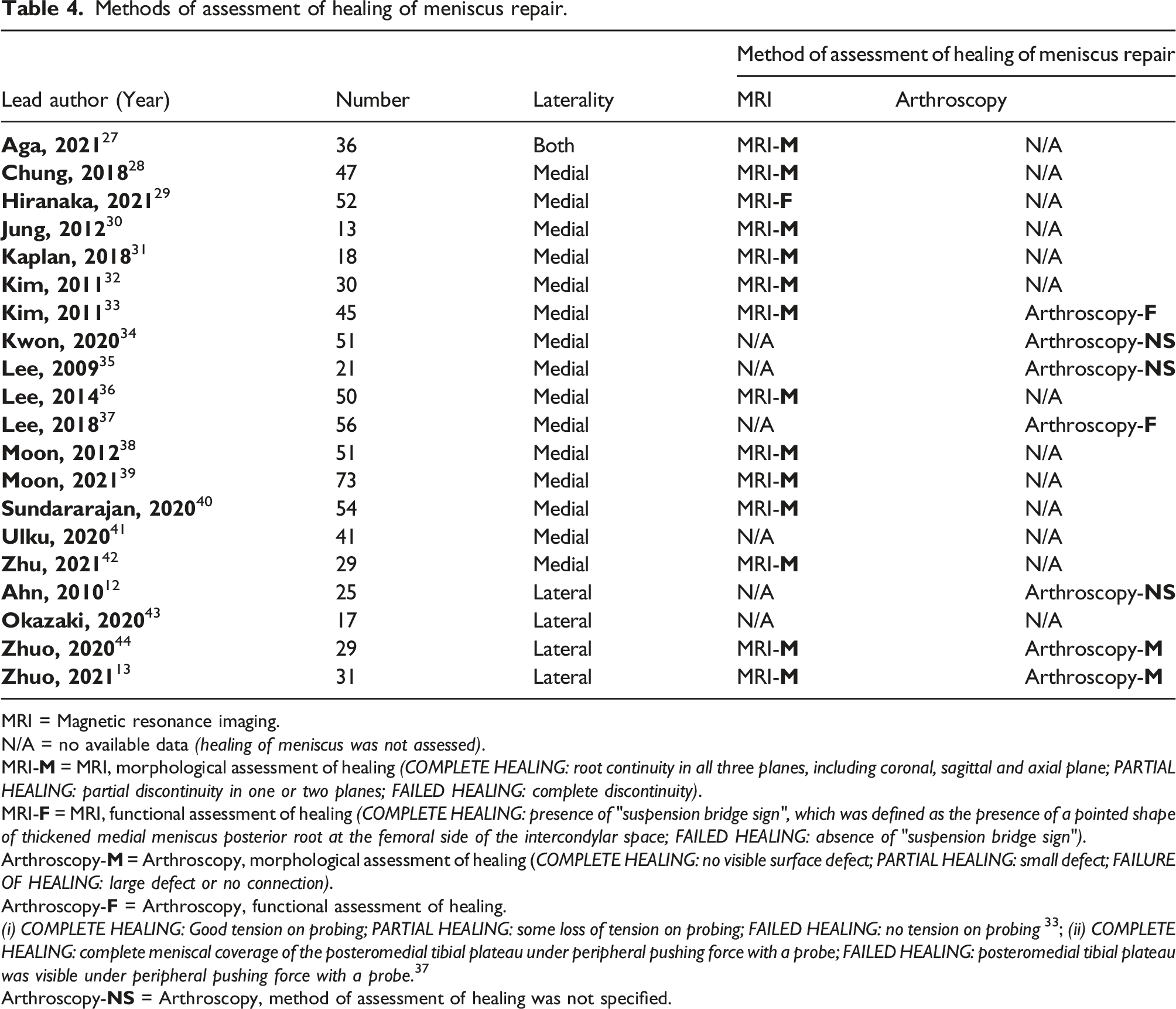
MRI = Magnetic resonance imaging.
N/A = no available data (healing of meniscus was not assessed).
MRI-
MRI-
Arthroscopy-
Arthroscopy-
(i) COMPLETE HEALING: Good tension on probing; PARTIAL HEALING: some loss of tension on probing; FAILED HEALING: no tension on probing 33 ; (ii) COMPLETE HEALING: complete meniscal coverage of the posteromedial tibial plateau under peripheral pushing force with a probe; FAILED HEALING: posteromedial tibial plateau was visible under peripheral pushing force with a probe. 37
Arthroscopy-
Amongst the medial meniscus root tear repair cohort, complete healing was observed in 207 knees (57%), partial healing in 135 knees (37%), and failed healing in 20 knees (6%). Significantly better outcomes were observed amongst the lateral repair group, with 67 (86%) demonstrating complete healing; 8 (10%), partial healing; and 3 (4%), with failed healing (p < 0.001, Chi-square test). (Table 3)
Healing status on reassessment arthroscopy
Second-look arthroscopy was used to evaluate the healing status of the meniscus repair in seven of the 20 studies.12,13,32,34,35,37,44 Overall, 163 knees (22%) had their healing status evaluated; 109 knees (4 studies) were assessed after medial meniscus root repair32,34,35,37 and 54 knees (3 studies) after lateral meniscus root repair.12,13,44
The arthroscopic definition of meniscus healing employed was different between the medial meniscus repair and lateral meniscus repair cohorts. Functional assessment was used to define successful healing in the two studies concerning medial meniscus posterior horn root repair.33,37 In Kim et al. 33 ’s study, “complete healing” was considered to be present if good tension was found on probing of the repaired site; “partial healing” if there was some loss of tension on probing; and “failed healing” if no tension was found on probing . On the other hand, Lee et al. 37 relied on the absence of displacement of the posterior-medial meniscus during probing to define healing of the repair. “Complete healing” was considered to be present if there was complete meniscal coverage over the posteromedial tibial plateau despite the meniscus was put under peripheral pushing force with a probe. If the posteromedial tibial plateau was visible under peripheral pushing force with a probe, the medial meniscus posterior horn repair was considered to be “partially healed”. The arthroscopic assessment of the healing of lateral meniscus posterior horn root repair was morphological.13,44 “Complete healing” was defined as the absence of any visible surface defect. If a small defect was found, the healing status was reported as “partial”. “Failed healing” was reported if a large defect was found or if there was no connection between the two ends of the repaired meniscus. The definition of healing during second-look arthroscopy was not mentioned in the remaining three studies.12,34,35 (Table 4)
No difference in healing was observed during second-look arthroscopy between the medial and lateral posterior root repair. Amongst the medial repair group, 86 (79%) demonstrated complete healing; 17 (16%), partial, lax, or scar tissue healing; and 6 (5%), failed healing. Concerning the lateral repair group, 45 (83%) demonstrated complete healing; 9 (17%), partial, lax, or scar tissue healing; and none with failed healing. (Table 3)
Clinical outcomes
A significant difference in the postoperative functional score (Lysholm score and IKDC subjective score) was observed between the medial and lateral meniscus root repair cohorts at a minimum follow-up of 1-year (p < 0.001). There was no difference in the postoperative Tegner activity scale between the two groups (Table 3).
Lysholm score
All of the studies included in this meta-analysis reported the mean postoperative Lysholm score, involving a total of 727 knees (97%). A mean Lysholm score of 82.1 ± 14.8 was reported amongst the 624 knees (16 studies) that underwent medial meniscus root repair. This was significantly less than the mean score of 93 ± 9.7 reported amongst the 103 knees (4 studies) in the lateral meniscus root repair cohort.
IKDC score
A total of 15 studies including 582 knees evaluated the postoperative IKDC score.12,13,28,29,31,32,33,34,36,37,39,40,42,43,44 A mean score of 72.2 ± 15.8 was reported amongst the 480 patients in the 11 studies evaluating medial meniscus root repair. The mean postoperative IKDC score was significantly greater for the lateral meniscus root repair cohort, with a mean score of 90.4 ± 11.9 reported amongst 102 patients (4 studies).
Reoperation
Just one study provided information on progression to reoperation. 27 Amongst the 18 knees that underwent medial meniscus posterior root repair, 2 knees underwent high tibial osteotomy due to complaints related to the fixation button. No concomitant repeated meniscus surgery or second-look arthroscopy were conducted for these 2 knees.
Subgroup analysis with reference to surgical technique
Residual meniscus extrusion with reference to surgical technique
Amongst the three different surgical repair methods studied, the residual meniscus extrusion, in both medial and lateral repair groups, was reported in transtibial pull-out repair and mid-substance repair only. Suture anchor repair was only performed in patients with a medial meniscal root tear. The amount of residual meniscus extrusion after transtibial pull-out repair of a medial meniscus root tear was significantly greater than its lateral counterpart; 323 knees in nine studies had a mean residual meniscus extrusion of 3.9 ± 1.7 mm after medial root repair,27,28,29,31,32,33,38,39,41 as compared to the 1±1 mm of extrusion seen in the 58 knees (3 studies) after lateral root repair (p < 0.001).13,27,43
Healing status on reassessment MRI with reference to surgical technique
Subgroup Analysis with reference to surgical technique.

Values are expressed as mean ± standard deviation.
Meta-analysis.
Chi-square test.
Statistical comparison not performed.
Healing status on reassessment arthroscopy with reference to surgical technique
A total of five studies including 132 knees utilised reassessment arthroscopy to assess the healing status of the meniscus repair after transtibial pull-out repair of the meniscus root.13,32,34,35,37 Amongst these, 109 knees (4 studies) were from the medial meniscus root repair cohort32,34,35,37 and 23 knees (1 study) from the lateral repair cohort. 13 No significant differences were seen in the healing status of the meniscus root repair in these two groups. Statistical analysis was not done for the other two repair methods as reassessment arthroscopy was not conducted. (Table 5)
Subgroup Analysis of influence of laterality of meniscus on post-operation meniscus extrusion in a subgroup with known time of surgery from injury
Subgroup analysis: Meta-analysis of results of posterior root tear repair in studies reporting time of surgery from injury.
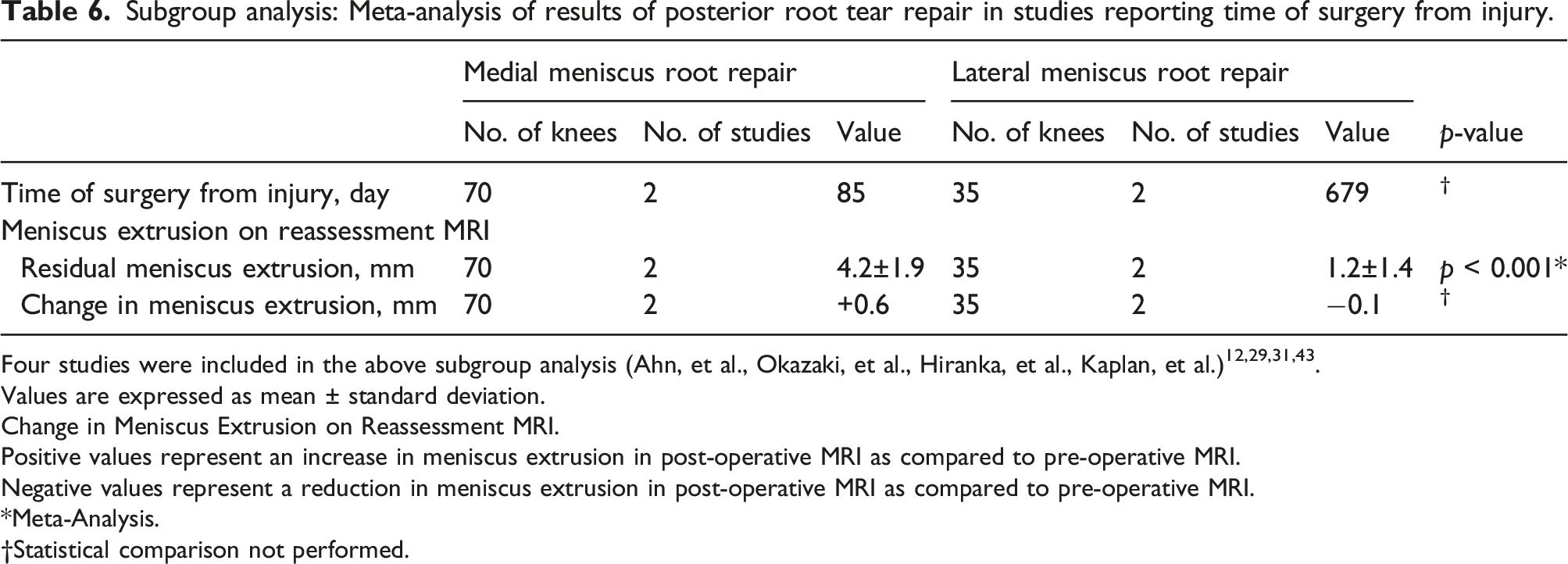
Four studies were included in the above subgroup analysis (Ahn, et al., Okazaki, et al., Hiranka, et al., Kaplan, et al.)12,29,31,43.
Values are expressed as mean ± standard deviation.
Change in Meniscus Extrusion on Reassessment MRI.
Positive values represent an increase in meniscus extrusion in post-operative MRI as compared to pre-operative MRI.
Negative values represent a reduction in meniscus extrusion in post-operative MRI as compared to pre-operative MRI.
Meta-Analysis.
Statistical comparison not performed.
Effect of the use of biological methods to augment the healing of meniscus repair
The use of biological methods to augment the healing of meniscus root repair was reported in only two studies. Both were studies about medial meniscus posterior horn repair 41,42 Ulku et al. 41 reported the use of fibrin clot and Zhu et al. 42 reported using microfracture. In view of this, statistical analysis was not performed. Findings were reported as followed.
Ulku et al. found that there was an average improvement of 0.8 mm (range: 0.6 mm–1.1 mm) meniscus extrusion after the repair. 41 Power analysis with respect to meniscus extrusion was not performed in Ulku’s study. On the other hand, Zhu et al. 42 found that meniscus extrusion significantly deteriorated by a mean of 1.2 mm after the surgery . Zhu et al.’s study was adequately powered.
Effect of lower limb malalignment in the healing of medial meniscus posterior horn root repair
Among all the recruited studies, significant varus malalignment was only reported to be present in one publication. 38 In view of this, the finding of that study was described as followed.
Moon et al. compared the results of medial meniscus posterior horn root repair between patients suffering from varus malignment of more than five degrees and those of less than five degrees. 38 They found that there was no difference in post-operation meniscus extrusion between patients having varus malalignment <5° (5.0 mm) and those >5° (5.2 mm). 38 The rate of healing of medial meniscus posterior horn root repair in this study was 90.3%. However, sample size analysis was not performed to justify the study was adequately powered. 38
Quality assessment
ROBINS-I (risk of bias judgements in non-randomised studies of interventions).
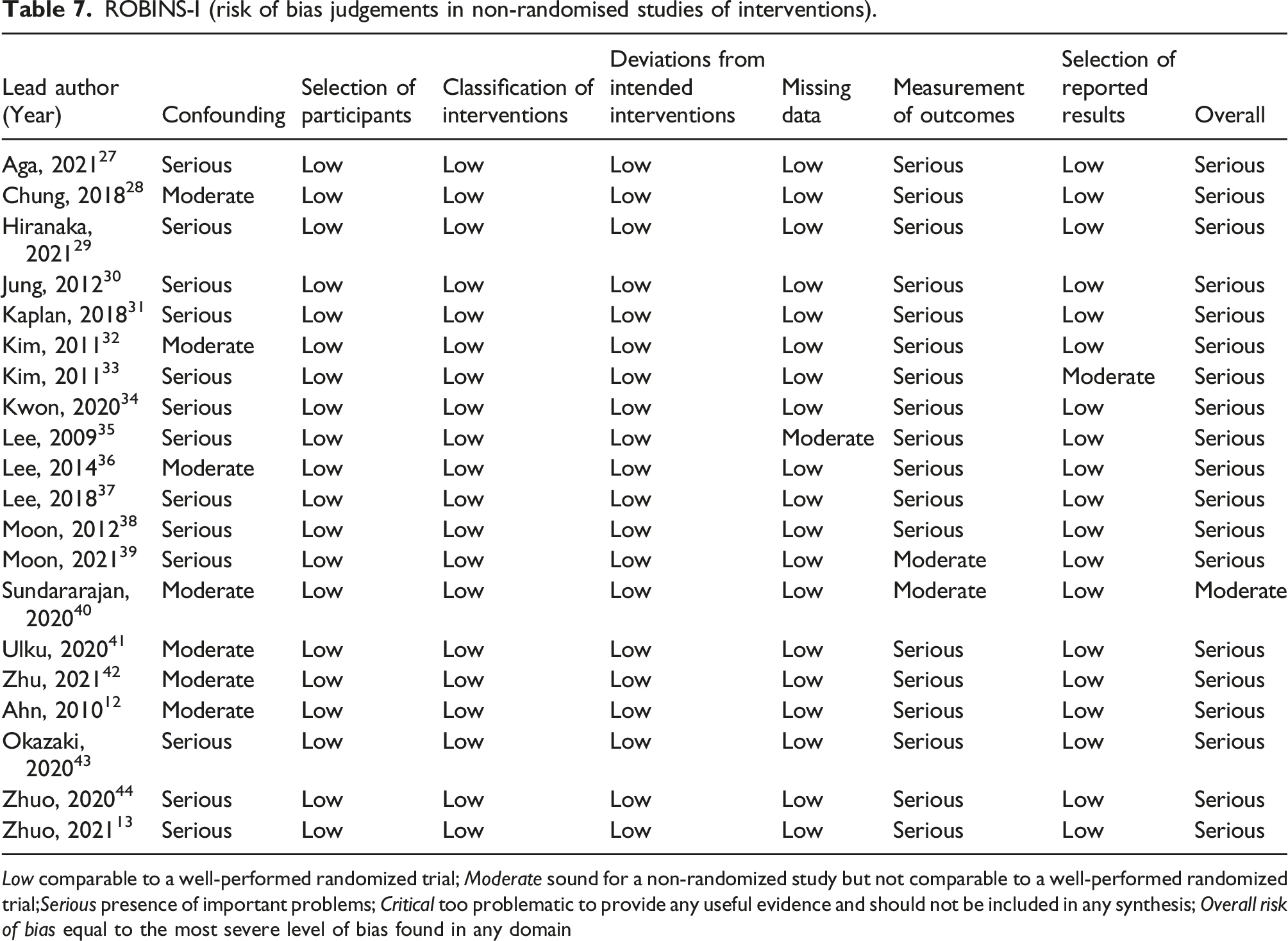
Low comparable to a well-performed randomized trial; Moderate sound for a non-randomized study but not comparable to a well-performed randomized trial;Serious presence of important problems; Critical too problematic to provide any useful evidence and should not be included in any synthesis; Overall risk of bias equal to the most severe level of bias found in any domain
Discussion
From this study, we found that the amount of residual meniscus extrusion following medial meniscus root tear repair was significantly greater than the extrusion observed after lateral meniscus root tear repair (3.8 ± 1.7 mm vs 0.9 ± 1.2 mm, p < 0.001). Additionally, the healing status of the meniscus repair as assessed on reassessment MRI, also demonstrated significantly poorer outcomes in the medial root repair group as compared to its lateral counterpart (57% complete healing vs 86% complete healing, p < 0.001). Significant differences in the postoperative Lysholm score and IKDC subjective score were also observed between the medial and lateral meniscus root repair cohorts, with the lateral repair cohort producing better functional outcomes (Lysholm score: 82 ± 15 vs 93 ± 10, p < 0.001; IKDC score: 72 ± 16 vs 90 ± 12, p < 0.001). This study also confirmed the contrasting patient characteristics observed between medial and lateral meniscus root tears. Patients with medial meniscus posterior root tears were older (55 ± 9 years vs 28 ± 9 years, p < 0.001), predominantly female (82% vs 34%, p < 0.001), and more likely to occur as an isolated root tear (99.7% vs 9%, p < 0.001). Whereas patients with lateral meniscus posterior root tears were significantly younger, predominantly male, and more likely to be associated with traumatic injury requiring concomitant ACL reconstruction surgery.
In this study, an increase in the degree of meniscus extrusion was observed after medial meniscus posterior root tear repair; however, the significance of this finding could not be determined. In a systematic review of 10 studies evaluating 297 patients, Chang et al. 11 found a decrease in medial meniscal extrusion from 3.77 mm to 3.69 mm after medial meniscus posterior root tear repair; the data, however, was too heterogenous to assess for any statistical significance. Despite the sustained meniscus extrusion after repair, the healing status, evaluated via reassessment arthroscopy in 11 studies and reassessment MRI in eight studies, found complete healing in 244 of 422 knees (58%), partial healing in 150 (36%), and failed healing in 28 (7%).
Unlike its medial counterpart, a reduction in the degree of meniscus extrusion after lateral meniscus posterior root tear repair was observed. In a systematic review of three different studies, Zheng et al. 23 found that there were observed reductions, albeit insignificant, of coronal extrusion after lateral meniscus posterior root repair in all three studies. One of the studies, however, was comparative in nature and reported a significantly greater reduction in meniscus extrusion after pull-out repair versus mid-substance repair. 43 Another two case-series included in the systematic review by Zheng et al. assessed the postoperative healing status of the meniscus repair on reassessment MRI, which found complete healing in 28 of 29 knees, and failed healing in 1.6,44 The healing rate of repaired lateral meniscus posterior root tears was also assessed after reassessment arthroscopy in 81 patients across five studies.6,12,44,45,46 At a mean follow-up of 22.1 months, the healing status was rated as complete in 59 of 81 knees, partial in 17, and failed in 5.
There is only one retrospective case–control study, we are aware of, that compares the results of medial and lateral meniscus posterior root repair. 27 Aga reported that the amount of persistent extrusion after meniscus root repair was more in the medial side (4.8 ± 1.9 mm; 18 knees) when compared with the lateral side (1.4 ± 1.1 mm; 18 knees). The result of our systematic review echoed the findings of Aga. In our systematic review of 746 patients (624 medial meniscus root repair and 122 lateral meniscus root repair), we found that the amount of residual meniscus extrusion following medial meniscus root tear repair was significantly more than the extrusion observed after lateral meniscus root tear repair (3.8 ± 1.7 mm vs 0.9 ± 1.2 mm, p < 0.001). Concerning the change in meniscus extrusion after surgery, the pooled figure for the medial side was +0.2 mm, and that of the lateral side was −1.2 mm.
Furthermore, a biomechanical study by Walczak et al. 10 reported that there were no differences in the amount of meniscus extrusion between the medial and lateral meniscus in the presence of a competent posterior root (0.338 mm vs 0.235 mm; p = 0.181). However, upon inducing posterior root detachment in both roots, the medial meniscus had consistently increased amounts of meniscus extrusion compared to the lateral meniscus (2.233 mm vs 0.471 mm; p < 0.0001).
Aga et al., 27 also compared the healing status of the repaired meniscus, as assessed on reassessment MRI, between medial and lateral meniscus posterior root repair. The proportion of patients with complete healing was significantly lower after medial meniscus root repair than compared to the lateral side (28% vs 61%; p < 0.05). In this systematic review, it was found that the proportion of knees with complete healing, as assessed on reassessment MRI, was significantly lower after medial root repair compared to the lateral side (57% vs 86%; p < 0.001).
There are no previous studies that have compared the healing status of the repaired meniscus, with reassessment arthroscopy, after medial and lateral meniscus root repair. When the healing status was assessed with second-look arthroscopy, it was found in the current systematic review that there was no difference in the pooled prevalence between medial meniscus posterior horn root tear and that of lateral meniscus posterior horn root tear; despite six out of 109 medial meniscus root repairs failing to heal, compared to none in the lateral meniscus root repair cohort.
The distribution of “complete healing” + “partial healing” versus “failed healing” between MRI assessment and arthroscopy assessment for medial meniscus root repair cohorts were 94% vs 6% (MRI) and 94% vs 6% (Arthroscopy), while that for lateral meniscus root repair cohorts were 96% vs 4% (MRI), and 100% vs 0% (Arthroscopy). However, a significant difference in the healing rate was only found in the MRI assessment cohorts (total number: 440) but not in arthroscopy assessment cohorts (total number: 163). The smaller sample size of the second-look arthroscopy cohorts may be a possible explanation for the observed discrepancy. Further studies with adequate sample size can be performed in the future to answer this question.
The differences in outcomes observed between medial and lateral posterior root tear repairs could potentially be explained by several different factors. Firstly, differences in the demographics between patients with medial and lateral meniscal root tears have been reported in the literature. In a recent comparative study, Krych et al. found that patients with medial meniscus root tears had a significantly higher mean age mean BMI, and were predominantly female; lateral meniscal root tears were significantly associated with concomitant ligamentous injuries. 9 These findings were also observed in the current systematic review (age: 55.2 vs 27.6 years; BMI: 26.3 vs 24.6; female sex: 83% vs 33%; concomitant ACL injury requiring ACLR: 0.3% versus 91%). (Table 2). It was likely that the primary cause of medial meniscus root tear was degenerative in nature, while that of lateral meniscus was traumatic in origin. This led to a discrepancy in the healing rate, as observed in the MRI cohorts of the current systematic review, and may also be associated with a difference in residual meniscus extrusion found on reassessment MRI.
Secondly, anatomical differences exist between the medial and lateral meniscus. Meniscofemoral femoral ligaments (ligament of Humphrey and ligament of Wrisberg) are normal variants attaching the posterior horn of lateral meniscus to the femur, and can be found in 60%–70% of the population. 3 The corresponding structure is not found in the medial meniscus. In a biomechanical study of cadaveric knees, following transection of the posterior lateral meniscus root alone, Forkel et al. 47 found no significant increase in the contact pressure in the lateral component of the knee. However, significant increases in contact pressure was noted when the meniscofemoral ligament was cut. As meniscus extrusion is found to result in the reduction in contact surface area, and a subsequent increase in joint contact pressure, 2 the finding of the biomechanical study of Forkel suggested that an intact meniscofemoral ligament may serve to prevent meniscus extrusion despite deficiencies in the root of the posterior horn of the lateral meniscus. The presence of the meniscofemoral ligaments may explain why significantly less meniscus extrusion was observed after repair of lateral meniscus posterior horn root tear when compared with the medial one.
Thirdly, the peripheral border of the posterior horn of the medial meniscus is attached to the joint capsule and subsequently the tibia through the meniscotibial ligament. 3 Meniscus tear was most commonly observed in the posterior horn of medial meniscus, resulting in meniscotibial ligament injury in this region. In a recent case-series by Krych et al., it was found on serial MRI scans that meniscotibial ligament disruption can result in medial meniscal extrusion despite an intact medial meniscus root. 9 New medial meniscus root tears was found in subsequent serial MRIs, suggesting that the observed meniscus root tear was a result of meniscus extrusion, rather than its cause. This finding may provide a possible explanation as to why 1) a majority of medial root tears occurred in older patient in the absence of obvious injury; and 2) a lack of correction in the degree of meniscus extrusion is observed despite successful medial meniscus root repair and healing. Instead, it was because the root cause of the meniscus extrusion (i.e. disruption of meniscotibial ligament) was not corrected. Further clinical study needs to be carried out to test this hypothesis.
Limitations
There were a number of limitations in the current systematic review. The major limitation of the current meta-analysis is the “poor quality” of the included studies. There was a serious risk of bias in all the included studies as assessed by the ROBINS-I criteria. Unfortunately, the recruited studies already represent the best evidence currently available in the literature. It is also technically impossible to carry out an experimental study to investigate the differences in root repair between MMPRT and LMPRT.
Second, despite pooling the available data in the literature, the sample size of the LMPRT cohort (total lateral repair: 122) was likely to be too small. The failure of demonstrating a difference in arthroscopy assessed healing of root repair may be secondary to the issue of sample size. It is worthwhile to repeat similar systematic reviews in the future when further data on lateral meniscus root repair is available.
Third, there was no available data on the classification of root tear in most of the studies included in this systematic review (e.g. by LaPrade classification 5 ). It was likely that the exact location and morphology of the root tear affected the result of its repair. Therefore, selection bias was present. To partly overcome this issue, a subgroup analysis was carried out in this systematic review. The comparison between medial meniscus root repair and its lateral counterpart were separately analysed for those operated by transtibial pull-out suture and those by mid-substance repair. It was found that the same conclusion in residual meniscus extrusion and meniscus healing was reached in the “transtibial pull-out suture” subgroup, but not in the “mid-substance repair” subgroup.
Fourth, the timing of reassessment MRI was not standardized among the studies recruited. Bias was present in the assessment of outcome. Unfortunately, this bias cannot be addressed by the current systematic review.
Despite the exact cause of the tear was not reported in some of the recruited studies in the current meta-analysis, it was likely that most of the medial meniscus posterior horn root tear was degenerative in nature and the lateral meniscus posterior horn root tear was traumatic in origin. Hence, one of the limitation of this study was that “apple” was compared with “orange”. However, the most important reason to differentiate degenerative meniscus tear from traumatic tear is to predict the healing potential of the tear. Degenerative meniscus tear is believed to have no healing potential. Hence, it should be treated either non-operatively or by partial meniscectomy. On the other hand, healing potential is present in acute traumatic meniscus tear. Hence, acute tear with appropriate tear pattern in the correct zone should be repaired. It was shown in the current study that despite being degenerative in nature, medial meniscus posterior horn root tears had healing potential if they were repaired. Complete healing were found in the repaired medial meniscus posterior horn root tear in 57% of post-operation MRI and 79% of second-look arthroscopy (Table 3). When both complete healing and partial healing were included, the corresponding figures were increased to 94% and 94% respectively (Table 3). Thus, the traditional concept that “degenerative meniscus tear has no healing potential” is not applicable to medial meniscus posterior horn root repair. However, despite the relatively high healing rate in medial meniscus posterior horn root repair, the correction of meniscus extrusion in medial meniscus posterior horn root repair was not satisfactory. There was an average of 0.2 mm deterioration of meniscus extrusion in medial meniscus posterior horn root repair (compared with 1.2 mm improvement in the lateral meniscus posterior horn root repair). On top of the ability to heal, it was likely that there were other reasons leading to this observed difference. Future studies should be designed to find out the reasons behind in order to further improve the results of medial meniscus posterior horn root repair.
Finally, there was no standard method in measuring the meniscus extrusion among the recruited studies. Bias existed in the type of MRI images used for measurement (e.g. T1 image versus T2 images; coronal images versus sagittal images) and the method of measurement (measured at a pre-determined anatomical region, e.g. mid-portion of tibial plateau; or the maximum meniscus extrusion among all the cuts, etc.). Reporting bias were presented.
Conclusion
The current systematic review showed that there were significant differences between medial and lateral meniscus posterior horn root tear and its repair in terms of pre-operative presentation, amount of meniscus extrusion, percentage of successful meniscus repairs, and post-operative functional outcomes. There was less residual meniscus extrusion and higher healing rates in the post-operation MRI after lateral meniscus posterior horn root repair when compared to its medial counterpart.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.