
Abstract
Objectives
Palliative treatment options for bone metastasis are limited, especially in cases where standard protocols have already failed. The purpose of this study was to evaluate the efficacy and safety of percutaneous ablation, either by cryoablation or radiofrequency, combined with percutaneous cementoplasty using cone-beam guided navigation. The objective was to relieve symptoms and improve functionality in patients suffering from pain secondary to bone metastases, as well as evaluate local disease progression post ablation.
Methods
We conducted a retrospective study of 13 patients (average age 63.6 ± 9.8, nine females) with symptomatic skeletal metastases treated using 3D imaging with navigation and followed for at least 12 months. The treatment protocol was implemented either after failure of first line treatment, or as first line when mechanical instability was present. Percutaneous lesion ablation was performed along with percutaneous cementation.
Results
In this study, we observed a statistically significant decrease in pain. The mean Visual Analog Scale pain score decreased from 7.1 ± 0.4 prior to CRA/RFA to 2.2 ± 0.3 after the procedure (p < 0.001). At the 12-months follow-up, all patients were able to ambulate with no assistance (Eastern Cooperative Oncology Group <2). One minor adverse event (paresthesia) and one major adverse event (drop foot) were resolved at 1 year of follow-up.
Conclusions
Treatment of bone metastasis with RFA and CRA in conjunction with cementoplasty using Cone-beam computed tomography navigation provides patients with significant palliative outcomes and in most cases, local tumor control.
Introduction
In the field of oncology, metastases of the bone are among the most common sites of spread along with metastases to the liver and lungs. 1 While some lesions are asymptomatic, other metastatic bone lesions cause debilitating pain, disability, and predisposition to pathologic fractures.2–5 The management of these metastatic lesions is challenging and requires a multi-disciplinary approach. 6 Existing treatment options such as radiotherapy, chemotherapy, surgery, and analgesia have been shown to reduce symptoms either partially or completely in up to 70%–80% of all cases. However, for the 20%–30% of patients who are unresponsive to conventional treatment options, alternative solutions to address both the spread of cancer and concurrent pain are necessary. 7 As a second line treatment option in unresponsive patients, image-guided percutaneous ablation procedures such as radiofrequency ablation (RFA) and cryoablation (CRA) have displayed promising results both in its palliative properties as well as a potential curative measure.8–11 This treatment together with post-ablation cementoplasy can increase the structural integrity of the bones, alleviate symptoms, and may reduce the probability of a pathologic fractures.12,13 A targeted approach, such as intra-operative image guidance for primary and secondary bone lesions allows for the patient to be treated in a precise and relatively safe manner. To date, most studies that involve this technology have been based on traditional imaging modalities, such as ultrasound (US), magnetic resonance imaging (MRI) and most frequently computerized tomography (CT) scans. 14 Each of these modalities, however, presents its own set of challenges. While US guided procedures are difficult to rely on and are more operator dependent, MRI guided procedures are costly and are therefore a less available option in many countries. CT guided ablation, though effective, is dependent on continuous scans and exposes the patient to excessive radiation. 15 While the field of image-guided percutaneous ablation procedures has shown great potential for palliative treatment of bone metastasis, the use of a more advanced imaging modality such as a cone-beam computed tomography (CBCT) provides the option for an enhanced alternative further improving the ablation procedure by increasing accuracy. 16
With no consensus established regarding the approach to skeletal metastasis refractory to traditional treatment, it is hypothesized that the integration of all current approaches may yield the optimal result in patients with high comorbidities.
In this study, we describe our approach to navigation system guided, minimally invasive percutaneous surgery. The purpose of this study was to evaluate the clinical and oncological outcomes of either CRA or RFA ablation methods combined with cementoplasty using the CBCT navigation system in patients suffering from metastatic bone tumors. The primary objective was to measure and compare pain scores using the Visual Analog Scale (VAS) pre- and post-ablation as well as functional status using the Eastern Cooperative Oncology Group (ECOG) functional scale at 12 months follow-up. Assessment of local disease progression post-ablation was the secondary objective.
Material and methods
Patient selection
Demographic details of the participants.

Clinical and oncologic status of the participants.

Inclusion and exclusion criteria
Inclusion criteria included: (1) single or oligo skeletal metastases at the extremity or pelvis (2) above 18 years of age (3), at least 12 months of follow-up and (4) underwent RFA or CRA followed by percutaneous cementoplasy under CBCT. Exclusion criteria included: (1) under the age of 18 years old, (2) pathologic fractures, and (3) spinal metastasis.
Data collection
Medical records were reviewed for general demographics, location of the tumor, type of primary tumor, and previous treatments. Pre-operative CT scans were reviewed to measure the metastatic volume and to evaluate the staging of the disease at the time of the ablation. Additionally, pre-operative VAS scores were gathered for each patient. Intraoperative data included the type of ablation and additional measures taken during the intervention such as fixation or neuro-monitoring. Immediate and late post-operative complications were documented and classified according to the SIR Adverse Event Classification Guidelines. 17 Lastly, pathology reports were assessed. Post-operative data was collected at three to 6 months intervals at the follow-up visit until last follow-up or until death to determine local reoccurrence and/or systemic progression of the disease. Positron Emission Tomography-Computed Tomography (PET-CT) images taken at the 12-month follow up were additionally analyzed to assess disease progression. VAS scores were used to demonstrate clinical improvement of symptoms and were recorded at 12-months post-operatively and were compared to the pre-operative score. Functional status was evaluated at 12 months post-operatively according to the ECOG Performance Status guidelines. 18 All patient scores were recorded at the time of their clinic visits.
Statistical analysis
Dependent variables were represented as mean ± SE. A t-test was performed using pre- and post-surgery VAS scores. A p-value of <0.05 was considered statistically significant. Statistical analysis was computed via SPSS software (IBM v25).
Pre-operative planning
All cases were pre-operatively planned using a digital 3D model, defining the exact trajectory, depth, and volume coverage of each needle in order to cover the whole tumor. The decision regarding RFA or CRA was determined based on tumor size. In cases when the lesion was more than 3 mm, CRA was used. RFA was employed in cases when the lesion was less than 3 mm. Regardless of tumor size, CRA was employed in cases where the tumor laid near nerves or if the patient had existing neuropathy. In cases where surgical time was important, RFA was used regardless of size, as to circumvent the thaw time experienced in CRA. All cases were first discussed with a multidisciplinary team including surgeons, radiologists, oncologists, and pathologists before proceeding with surgical treatment.
3D imaging and navigation
All procedures were carried out in the operating room. All ablations were performed under general anesthesia on a fluoroscopy capable operating table and carried out by the senior author (O.S.), a fellowship trained orthopaedic oncologist. Optical tracking instruments were properly placed and secured. An initial scan was made using the Cone-beam navigation system (o-arm® scanner Medtronic Sofamor, Danek Memphis, TN, USA). A 3D image was then generated by the navigation system (StealthSta-tion®, Medtronic Sofamor, Danek Memphis, TN, USA). After capturing an initial image, the relevant instruments were calibrated in the system (suretrack ®, Medtronic Sofamor, Danek Memphis, TN, USA). Once it was confirmed that the generated image and calibration and the preoperative image were consistent, the ablation protocol was implemented.
Ablation preparation
The ablation procedure included either of the two mentioned ablation modalities (RFA or CRA). Ensuing steps were then all made under Cone-beam navigated guidance. Surgical instruments, including the Jamshidi needle, probes, and cannula for cementation were calibrated and synchronized in order to display them on the navigation system, which reduced intraoperative fluoroscopy and CT scans. Next, a calibrated Jamshidi needle was used to enter the cortex of the tumor. The calibrated ablation probes were then guided to the precise location within the lesion determined by pre-operative planning. A second scan was then performed to ensure the probe was accurately positioned according to the pre-operative plan to ablate the entire necessary region. A sample was extracted for pathologic evaluation before beginning the specific ablation protocol.
Radio frequency ablation (RFA) protocol
RFA is a thermo-ablative procedure that causes coagulative necrosis inside the tumor19,20 A 15-cm RF probe needle (Covidien Ltd. USA, cool tip 15-cm long) was inserted into the center of the tumor, generating heat by conducting alternate currents throughout the needle within a range of 350-500KHZ. This increased the intra lesion temperature to over 900°. 17 The ablation phase was a total of 16-min.
Percutaneous CRA
In this procedure damage to the cell membrane incites apoptosis causing cell death.21,22 Adequate needle placement and number was calculated as part of the preoperative planning to ensure optimal coverage of the whole lesion. An ice rod needle (Galil Medical Ltd. Yokneam Israel) was placed into the center of the tumor to perform the ablation (Figure 1). This phase included 10 min of freezing, 5 minutes of thawing, followed by 10 more minutes of freezing. During the freezing interval, temperatures were kept below minus 40 degrees Celsius creating an ice ball encompassing the entire tumor. We were unable to and therefore did not observe the ice-ball intraoperatively. Constant warm saline was pumped to hydro-dissect the neighboring tissues, preventing thermal damage. Metastatic lesion to the acetabulum. (a + b) intraoperative image of the CRA needle located in the lesion before ablation.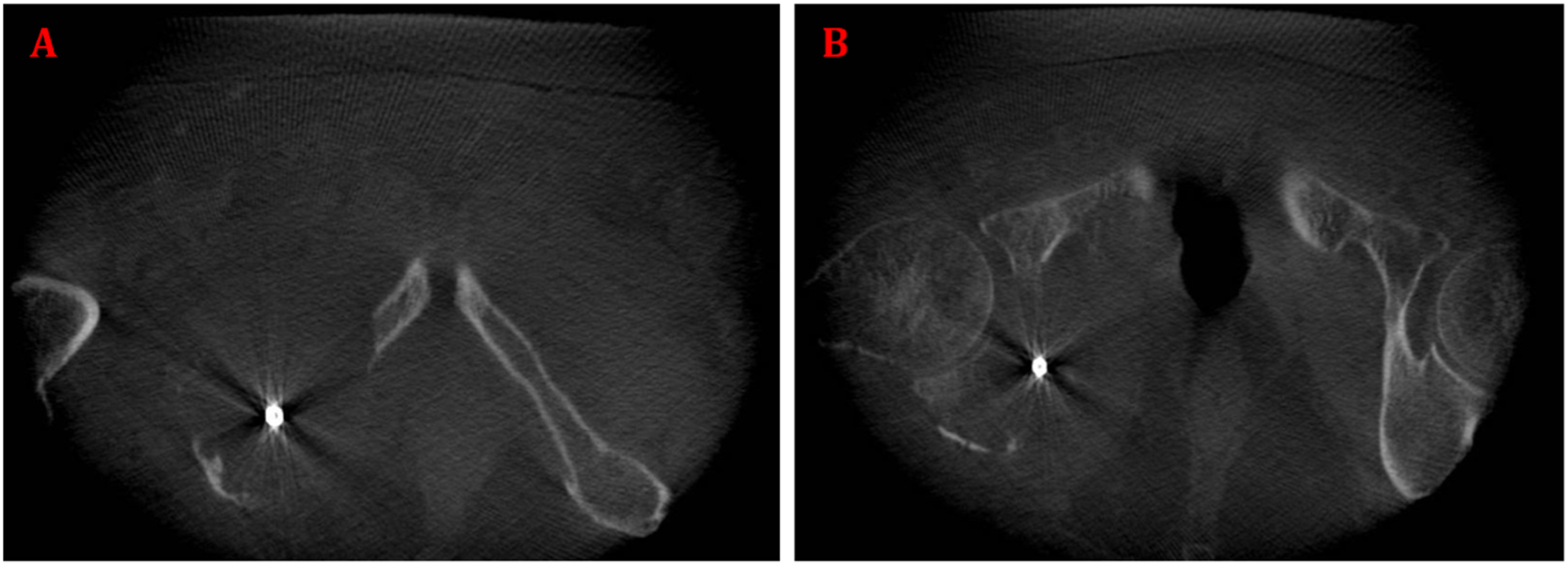
Percutaneous cementation
This procedure was used to add structural integrity to the lesions post-ablation. Cementation was performed using a polymethyl methacrylate (PMMA; Osteopal V, Heraeus Medical, Wehrheim, Germany) injection through a 10-gauge bone trocar. All instruments were calibrated, and cementation was performed under navigated guidance. Only after the location of the cannula was verified under 3D CT image, we inserted the cement and verified adequate placement under fluoroscopy. A thermal reaction solidifies within the tumor, filling the cavity. Though not intended to reduce the tumor burden, this procedure is successful in increasing the stability of the bone thereby reducing local pain and the potential for pathologic fractures.20,23,24
Additional preventive measures
In patients with an impending fracture and a high Mirels score, preventative intramedullary fixation was performed following the ablation with a long Gamma nail (GN-3;
Results
A total of 13 patients underwent ablative procedures: 5 (38.5%) patients received CRA and 8 (61.5%) received RFA. 11 patients (11/13, 84.6%) underwent previous treatments with conventional methods such as chemotherapy and radiotherapy. Three patients (3/13, 23.1%) did not receive neo-adjuvant therapy and were treated with navigated percutaneous ablation as a first line treatment due to an impending fracture. Primary tumor types and locations are presented in Table 1. The volume of the tumors ranged between 10*10 mm (100mm2) to 30*30 mm (900 mm2), with an average volume of 481.8 ± 267.6 mm2. Two patients with tumor diameters less than 3 mm received CRA due to history of peripheral neuropathy. Two patients with tumor diameters greater than 3 mm were changed to RFA due to proximity to neuro-vasculature. Overall, there were no deviations from the original pre-surgical plan. All interventions were performed using intra-operative CT imaging and individualized 3D navigational guidance. In addition, the navigation system allowed for optimal instrument placement with no need to reposition the ablation probes after the confirmatory CT scan. In total four patients (4/13 30.8%) (two from the RFA group and two from the CRA group) had a high Mirel score and were therefore treated with intramedullary femoral nailing to prevent impending fractures. The Mirel score was reported for four patients with lesions located in long bones with an average score of 8.5. Twelve (12/13, 92.3%) patients were treated with percutaneous cementation using a PMMA injection. One patient (1/13, 6.7%), was scheduled for cementation, but the decision was made intra-operatively to not proceed due to risks of intra-articular leakage.
VAS scores were documented pre- and post-operatively. All patients showed improvement in the average VAS scores by the 3-month interval and concurrently at the 12-months follow-up. In addition, 12 patients (12/13, 92.3%) had ECOG score <2. The average VAS pre-ablation was 7.1 ± 0.4 and post-ablation was 2.2 ± 0.3 (p < 0.001). Final imaging using Positron Emission Tomography-Computed Tomography (PET-CT) took place at the 12-month follow up. Nine patients (9/13, 69.2%) had no uptake, two patients had stable disease (2/13, 15.4%), and one patient had local disease progression (1/13, 15.4%). One patient passed away (1/13, 7.7%). Immediate post-operative complications were recorded in three patients of the RFA group (3/8, 37.5%): One patient experienced transient paresthesia with sciatic nerve involvement, one patient had a drop-foot, and one patient had excessive bleeding during the ablation phase. All three patients were ablated under nerve conduction surveillance using electromyography (EMG), which showed no indication for any nerve involvement during the ablation. For the third patient, the bleeding presumably did not originate from any major vessel; the patient was monitored and had normal vital signs throughout all phases of the procedure. All symptoms were resolved by the 12 months follow-up.
Discussion
Adequate palliative outcomes in unresponsive patients with bone metastases is a problem that requires innovative treatment methods. Despite major therapeutic advancements in cancer treatment and research, oncologic patients continue to experience high levels of morbidity and mortality. Bone metastases are common in advanced cancer and its presence commonly signifies serious morbidity and a poor prognosis. 25 In most cases palliative care is therefore an essential component of treatment.1,3,5,7 Minimally invasive treatments boast low rates of surgical complications ideal for the oncologic patient with a high degree of comorbidities. However, CRA, RFA, and cementoplasty are complex, challenging procedures necessitating multiple instruments and radiographic techniques for proper results. The treatment techniques for bone metastases described in this study demonstrates high feasibility, efficacy, and symptom improvement. With no consensus established regarding the approach to skeletal metastasis refractory to traditional treatment, our results suggest that the integration of all current approaches may yield the optimal result in patients with high comorbidities. The principal finding of this study was to demonstrate significant improvement in patient symptoms and function following navigated ablation. Significant improvements in patient symptoms as well as disease control in most cases were established by favorable results at the 12 month follow up.
Percutaneous ablation has been shown to produce favorable outcomes for local pain control.11,21 Gallusser et al., 26 showed a 75% improvement in pain score rating using a similar method as the one demonstrated, and Goetz et al. 9 has showed improvement in VAS scores in 95% of his cohort, and notable reduction of opioid consumption. The present study reinforces previous literature of successful local pain control as demonstrated by the 100% VAS score improvement. The authors attribute this slight improvement in results with respect to the aforementioned studies to the use of the combined, multi procedure approach. The analgesic potential of cementoplasty has been attributed to the stabilization of intangible microfractures, and the thermal ablation of local nociceptors along with the cancer lesion itself. When combined with RFA or CFA that reduce structural integrity of bone, cementoplasty can restore the stability of the bone to improve overall quality of life.27,28 Furthermore, the addition of navigation guidance under CBCT optimized the accuracy and execution of each procedure.
Another important outcome of any palliative treatment is to improve functionality mainly by maintaining ambulating capability. Utilizing the ECOG system, 18 an analysis of our cohort showed functional improvement at the 12 month follow up. Excluding the single patient that died, all other patients maintained an ECOG of zero or one at the 12 months follow up. Furthermore, percutaneous ablation as a measure of achieving local disease control has been previously evaluated in several studies. Our results are consistent with the findings of both Mcmenomy at el. and Gallusser et al. They demonstrated local disease control in 63% and 68% of patients using percutaneous guided ablation, respectively.26,29
Additionally, PET CT scans at the 12-month follow up of our study sample showed no uptake in 69.2% of patients and no progression in 15.4% of patients. This further demonstrates the efficaciousness of the procedure in disease progression. The last surgical technique described, cementoplasy, is an excellent method of reducing pain by restoring the structural integrity of the affected bone (Figure 2).
30
Cazzato et al.,
12
conducted a meta-analysis including 10 studies that measured the pre- and post-ablation VAS scores. According to the results, 68.2% displayed significant improvement in VAS scores, 27.4% reported mild improvement and only 4.4% experienced no change at all. Further analysis of functional improvement post ablation resulted in 71.9% of patients with significant improvement, and 22.1% of patients with mild improvement. Results in our cohort displayed superior outcomes in both VAS scores and functional scores suggesting that the combination of ablation together with cementation, under navigation guidance, is preferable to solely cementation. (a). Lytic lesion in a patient suffering from bone metastasis in the left midshaft femur. (b). Intra-operative placement of cryo-needle. (c). Intra-operative imaging with intramedullary nail insertion and cementoplasty. (d). Post-operative imaging after ablation, cementoplasty, and prophylactic intramedullary nail insertion.
Currently there is limited data on CBCT navigated ablation for bone metastases in the scientific literature. Percutaneous interventions can be challenging especially when in proximity to neuro-vasculature and other vital structures. The current use of image guided ablation relies on repetitive scanning of the patient and excessive radiation exposure. Cone beam guided ablation procedures have been shown to reduce radiation exposure with respect to regular CT guided ablation. 31 By using the stealth station navigation system, the surgeon is able to ascertain his position and improve accuracy, maintain relatively low radiation exposure to the patient and staff, and operate on a high confidence level.32,33 Much of the success demonstrated by the post-ablation data on tumor progression and pain levels can be attributed to the efficiency and accuracy of this system.
In the current standard for this procedure, many ablations are performed by interventional radiologists. In our study, however, the presence of an orthopedic surgeon proved to be a vital component in the success of the treatment, specifically in four patients who also required intramedullary nailing fixation for impending femoral shaft fractures (Figure 2). Iatrogenic fractures are a well-known complication following bone tumor ablations. 34 The loss of structural integrity from the loss of bone stock due to osteonecrosis puts patients at increased fracture rates. 35 While no iatrogenic fractures were observed in this cohort, having an orthopaedic surgeon as the provider effectively enables immediate fixation of impending or iatrogenic fractures should they arise. In patients with metastases around the acetabular cup of a total hip arthroplasty, the experience of an orthopedic surgeon is required to appropriately navigate this unique location. Additionally, there is inherent variability of intra-operative blood loss during this procedure. From our experience, encountering an intraoperative bleed after the ablation of a RCC metastasis, performing the ablation procedure in the operating room by an orthopaedic surgeon enabled efficient transition to open surgery for successful management. The need for the CBCT guided ablation procedures to be conducted by a capable orthopedic surgeon in the operating room setting is critical.
One patient (1/13 patients, 7.7%) suffered from transient nerve-related complications despite normal intra-operative nerve conduction monitoring during the ablation. This can be explained by the fact that most electromagnetic instruments are affected by the electronic current during the ablation procedure. 24 This remains a disadvantage in RFA ablation procedures.
Limitations of this study are the small sample size and heterogeneity of the study group regarding tumor location and volume, in addition to the relatively short follow up period. Furthermore, in order to assure the superiority of the 3D navigation method, there is a need for a control group which would employ other image guided navigation for comparison.
Conclusion
Percutaneous CBCT navigated ablation procedure and cementation is a safe, efficient, and reliable second-line treatment for symptomatic bone metastases. Performing complex percutaneous surgery in a stepwise fashion is possible and safe under cone bean guided navigation. Additionally, performance of the procedure by an orthopaedic surgeon in an operating room is an essential component to the success of the procedure, especially if additional orthopaedic procedures are necessary. Favorable outcomes and low complication rates with respect to previously published methods places this approach as an appropriate bone metastases treatment.
Footnotes
Authors’ contributions
BE and OS came up with the idea for the study. BE and AB were the main authors. AL, AE, AE, DR and UR collected and analyzed the data. YG, SD, AS, OM and OS are part of the orthopedic oncology team who participated in the procedures. All authors revised and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s note
All methods were carried out in accordance with relevant guidelines and regulations.
Ethics approval
The study was approved by the ethical committee at Tel Aviv Medical Center (approval number: 0173-21).
Informed consent
All authors declare consent for publishing the study.
Data availability
All data are available upon request from the corresponding author.