
Abstract
Aim of the study
To compare the outcomes of three knee arthroplasty design philosophies and surface tribology.
• A zirconium-surfaced, bicruciate-stabilised implant designed to mimic kinematic movement and improve flexion and outcomes;
• A cobalt-chrome surfaced, multi-radius design with built-in femoral external rotation to aid balancing and patella tracking through a deeper trochlea groove;
• A zirconium-surfaced, single-radius implant designed on surface conformity, particularly within the patello-femoral joint.
Methods
313 knee replacements - 103 Journey II, 103 Genesis II and 107 Profix - were statistically assessed at a minimum of 2 years using WOMAC, Oxford and SF-12 scores, and range of movement.
Results
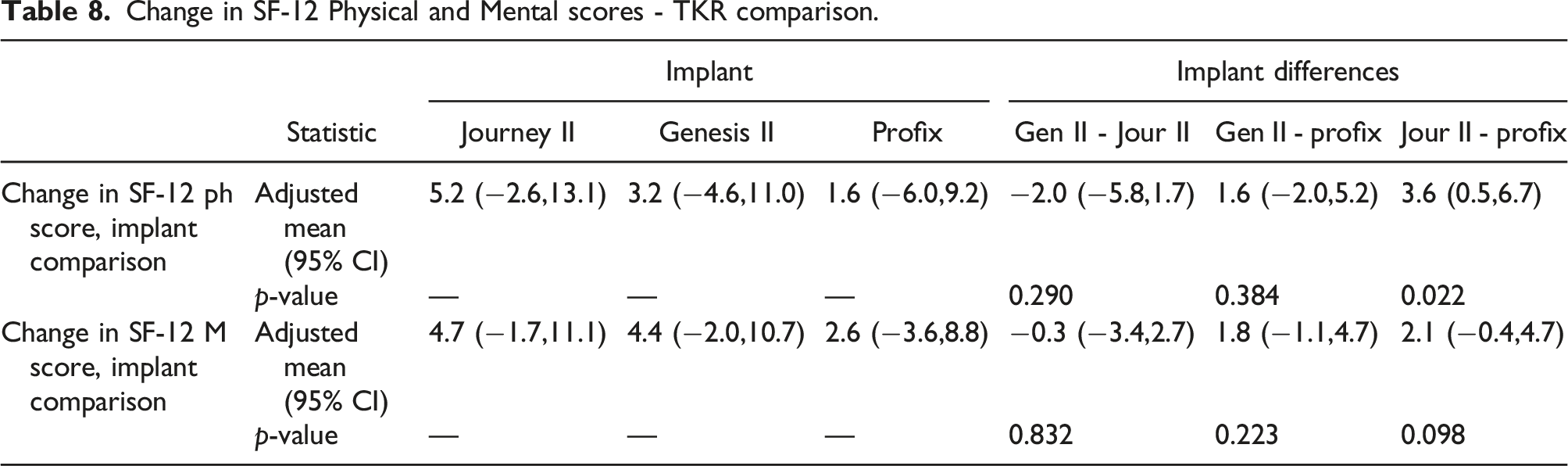
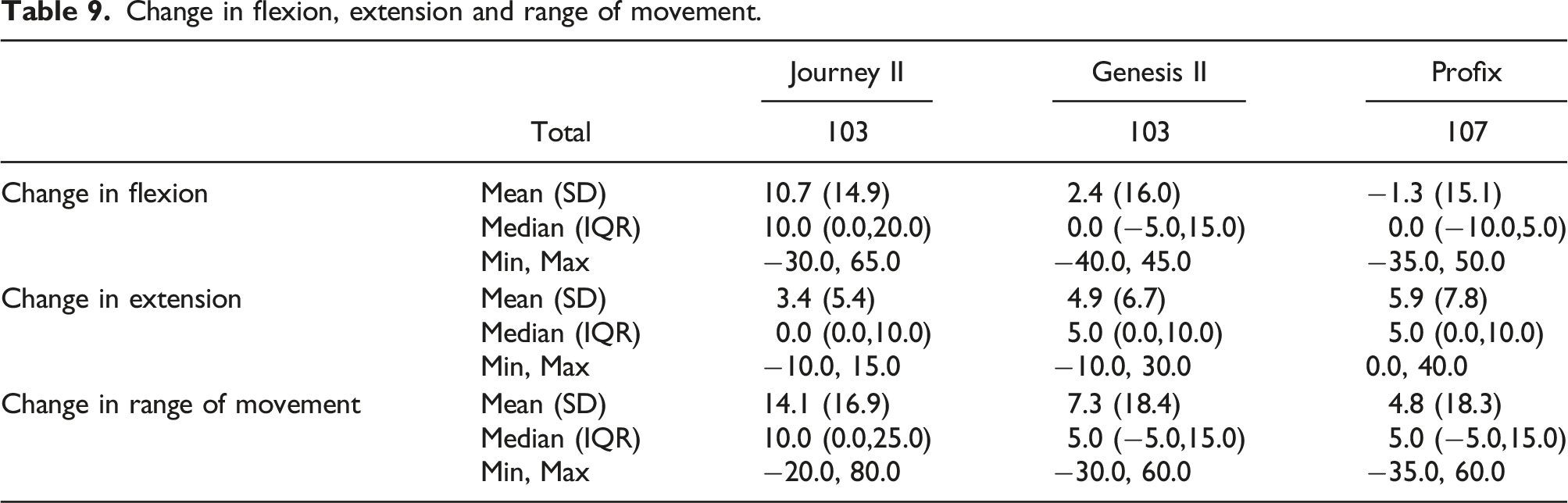
There was no difference between the actual or unit change in WOMAC scores (p = 0.140 and p = 0.287), SF-12 physical (p = 0.088) or mental scores (p = 0.975) between the three implants; or between the actual or unit change in Oxford score (p = 0.912 and p = 0.874) for the Journey II or Genesis II. The Journey II produced more flexion and range of movement than the Genesis II (p < 0.001 and p = 0.018) and Profix (p < 0.001 and <0.001) with no difference between the latter two (p = 0.402 and 0.568); with no difference in extension between the three implants (p = 0.086). There was no difference between those with or without a resurfaced patella.
Conclusion
The three design philosophies and surfaces yielded no difference in outcome scores at 2 years post-operatively. The Journey II demonstrated better post-operative flexion. Resurfacing the patella did not alter the outcome scores or flexion.
Introduction
The Journey II total knee replacement (Smith and Nephew, Watford, UK) was introduced in 2012 as a replacement for the Journey BCS, for which a number of complications had been reported including dislocation between the tibial insert peg and the femoral component which was believed to occur as a consequence of high flexion angles. The Journey II successfully addressed this issue with changes to the cam design.1,2,3 The arthroplasty was designed on the kinematic principles which theoretically would produce better movement and improved patient outcomes.1,2 It set out to achieve this through a design which replicated both anterior and posterior cruciate function; a concave medial but convex lateral tibial polyethylene insert designed to prevent paradoxical motion causing mid-range instability; and a three degree varus joint line designed to replicate the normal anatomy of the average knee. 2 In addition it was manufactured in an oxidised zirconium/niobium alloy, marketed as Oxinium, which due to its hardness had better wear characteristics than cobalt-chromium as well as a lower coefficient of friction.4,5,6,7,8 The thermally driven oxidisation process creates an oxidised zirconium/niobium alloy surface, with the hardness properties associated with a ceramic, but with the strength of a metal. The composite structure means there is no bonding weakness at the surface. 9 Oxidised zirconium/niobium implants have been shown to have good survival in the short-, medium- and long-term.4,6,8,10,11
The Genesis II total knee replacement (Smith and Nephew, Watford, UK) was first introduced in 1996 and is one of the more commonly used knee replacements in UK, Europe and North America with over 1.4 million implanted world-wide to date. 12 It is based on a principle of built-in external rotation of the femur to aid balancing and patella tracking coupled with a deeper and more lateralised trochlea groove. The cross-section of the femoral component is a multi-radius design to maximise range of movement, stability and minimise wear. 7 It is available in cobalt-chromium as well as oxidised zirconium/niobium alloy femoral components with standard metal and all polyethylene tibial bases. 13 There are a large number of publications confirming its good short-, medium- and long-term survival.7,13,14
The Profix total knee replacement (Smith and Nephew, Watford, UK) was first introduced in 1994 as an innovative knee arthroplasty design based upon improved characteristics with respect to implant conformity with a single radius of curvature to provide a high degree of femoro-tibial contact area throughout flexion with a short small-radius posterior condyle were to improve the terminal range of movement. In particular its trochlea was sunken and asymmetrical making it a reportedly patella-friendly design. These features aimed to reduce polyethylene wear and in addition it was designed as an adaptable replacement to allow it use in a diversity of indications.15,16 Similar to the Genesis II arthroplasty, it was available in cobalt-chromium as well as oxidised zirconium/niobium alloy femoral components with standard metal and all polyethylene tibial bases. 16 It was phased out of circulation in 2010 as a result of an upgrading of the Smith and Nephew portfolio but had good medium-term outcomes in a number of publications.11,15,16
Based on the aforementioned claims by each implant manufacturer, it is theorized that the modern kinematic design of the Journey II should improve function as compared to the more traditional designs. If however, it is the zirconium/niobium surface that is the factor that determines outcomes, then the Journey II should fair no better than another standard zirconium/niobium surfaced arthroplasty but better than a cobalt-chromium implant. The aim of this study was to investigate this claim, our null hypothesis being there was no difference in functional outcomes between the modern and traditional designs or between the bearing surfaces.
Materials and methods
We identified from our prospectively collated departmental registry, all Journey II implants that were a minimum of 2 years post-operation. In addition, we identified all cobalt-chromium Genesis II arthroplasty patients who had had their surgery over the same time period as the Journey II cohort. A cohort of patients who had had an oxidised zirconium/niobium Profix arthroplasty were identified working backwards from the last implant in 2010 and over the same time period as the other two groups. This produced three groups of patients with three different implant designs allowing a comparison of an oxidised zirconium/niobium bicruciate stabilised kinematic design (Journey II) against a cobalt-chromium multi-radius anatomical design (Genesis II) against an oxidised zirconium/niobium single radius anatomical design (Profix). The implants were analysed for any differences in post-operative range of movement, outcome scores or complications with regard to design philosophy, manufacture (zirconium/niobium alloy or cobalt-chromium) or not. In addition, the study allowed us to assess the influence of patella resurfacing in these cohorts.
Since 1999, all patients undergoing a total knee replacement in our hospital are prospectively added to the departmental registry along with demographic data, pre-operative measurements of function and pre-operative WOMAC, SF-12 and Oxford scores. Prior to 2010, all patients were offered a Profix arthroplasty, with the younger, more active or those with higher demands offered a zirconium/niobium implant although there were no strict rules regarding age constraints. In 2010, the Profix was replaced by the Journey BCS and the Genesis II, and since 2013, the Journey II and Genesis II have been used. The Journey II was only available in zirconium/niobium but the Genesis II was available in both cobalt-chromium and zirconium/niobium varieties. Before 2010 only WOMAC and SF-12 scores were recorded, with all three after this date; hence Oxford scores were not available for the Profix implants.
The departmental registry was used to identify all patients who had undergone a total knee replacement in each of the three implant groups – Journey II, Genesis II and Profix – and who had a full pre- and post-operative data collection. To account for the wide variation in short-term outcomes, such as initial variations in flexion due to swelling and to give a more accurate indication of the implant outcome, only patients who were a minimum of 2 years post-operation were studied. All Genesis II patients were restricted to those who had a cobalt-chromium rather than an oxidised zirconium/niobium femoral component. The Profix cohort were identified working backwards from the last implant in 2010 and over the same time period as the other two groups and checked to ensure they had had a zirconium/niobium femoral implant. Updated information from the arthroplasty follow-up clinic was correlated against that of the registry to ensure all complications were identified.
All operations were undertaken in laminar flow theatres by four consultant surgeons (AJAS, JSD, JVB and AP) or by a senior surgical trainee under the direct supervision of those surgeons with an identical routine post-operative rehabilitation as per the department’s protocol. All patients were assessed pre-operatively as part of the routine care pathway, which involved collection of demographic data, outcome scores and range of movement using a goniometer. The same post-operative data was collected by clinical physiotherapy specialists (JP and JY) as part of the routine post-operative follow-up schedule where demographic data was collected, outcome scores taken and range of movement measured using a goniometer. Patients were followed up at 3 months, 1 year and regular intervals thereafter with the same data collected at each consultation. The data was added prospectively to the registry.
In addition to the standard outcome scores we have also looked at the ‘unit’ change in scores. A patient with a pre-operative Oxford score of 10 who improves post-operatively to 48 has increased their score by 38. Another patient with a pre-operative score of 15 who also improves post-operatively to 48, has improved by 33 hence appears to have a lesser improvement although both have improved by their maximum amount. By dividing the improvement in score by the difference between the pre-operative score and 48 gives a proportionate ‘unit’ improvement, which in these two cases would be 1.0. A similar calculation can be done with WOMAC scores, dividing the improvement in scores by 96. We have called this the ‘unit’ change in score.
Minimal clinical improvement score was assessed for both the WOMAC and Oxford Knee Score and set at the level of a decrease by 15 points and increase by five points respectively to take into account values identified in the range of papers in the literature.17,18,19,20
A total of 313 knee replacements were identified, consisting of 103 Journey II, 103 Genesis II and 107 Profix implants and data was assessed by a medical statistician (MG). Descriptive statistics were summarised for all scoring systems for all three knee replacements. Counts and percentages were presented for those who did and did not reach minimal clinical improvement and binomial test was used to test for a difference between proportions between each criteria and overall. For all scoring systems, the changes from pre-op to post-op were calculated and descriptive statistics of the changes were summarised. A mixed model (SAS proc mixed) was used to test for treatment differences between the pre- and post-op scores and outcomes. All mixed models were adjusted for patient’s age and gender, whilst also adjusting for baseline scores (pre-op scores) to account for potential imbalances. Mixed models were also used on WOMAC and Oxford unit improvement, however as these did not have pre-op scores, baseline could not be adjusted for and was taken out the model leaving adjustment for age and gender only. A Kruskal–Wallis test was used to test for differences in the treatments for these changes. A two-sample Wilcoxon is used for pairwise comparisons when there has been a significant Kruskal–Wallis test. All statistical tests were performed at the 5% level.
Ethical approval for the registry containing patient data was obtained locally through the Liverpool Research Trials Centre (refs 1893 and 2060); early data were held on a database in Scotland requiring ethical approval through the Multi-Centre Research Ethics Committee for Scotland (ref MREC/04/10/004), who classified this as audit data which did not require a formal review by an ethics committee. Patients consented to having their data added to the registry and that it may be used in subsequent research publications and presentations.
Results
Demographic data - Body mass index (BMI) (*Genesis II significantly older than Journey II and Profix (p < 0.001); no difference in ages between Journey II and Profix).

Implant data.


Genesis II CoCr total knee angled view CR.

Genesis II CoCr PS exploded view.
There were a total of four intra-operative events in the 313 replacements amounting to 1.3%. These were a small cut to the patella tendon and a femoral crack in the Journey II cohort; and a partial tear of the patella tendon and a slight stripping of the medial collateral ligament in the Genesis II cohort. None of these four patients required a change to the operation or post-operative rehabilitation. There were no intra-operative events in the Profix cohort. Post-operatively there was one infection in the Genesis II cohort and three in the Journey II cohort that required surgical debridement. One patient with a Profix implant required a manipulation under anaesthesia for stiffness. These five patients amounted to 1.6% of the 313 knee replacements. One patient in the Genesis II group underwent a secondary patella resurfacing at 15 months post-operatively for persistent anterior knee pain and improved thereafter. One patient in the Journey II cohort was revised at 3 years for aseptic loosening of the tibia and made a good recovery. None of the Profix cohort have had further surgery to date. One of the Genesis II patients died at 5 years after surgery from unrelated causes (Figures 3 and 4). Genesis II CR zirconium. JOURNEY II BCS zirconium and CR.

Actual and unit change in WOMAC score.
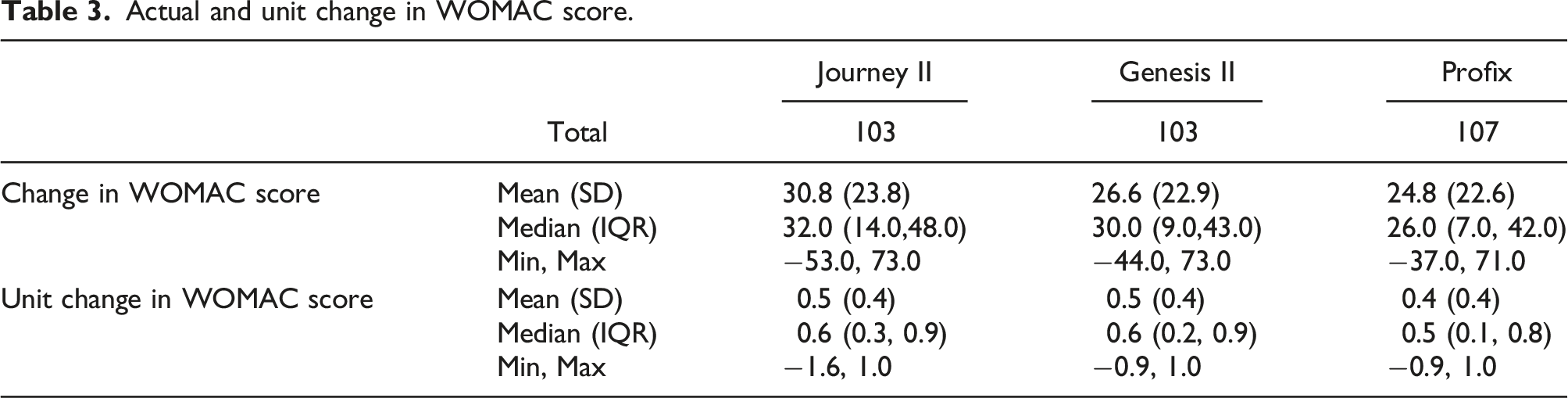
Actual and unit change in WOMAC score - TKR comparison.

Actual and unit change in Oxford score.

Actual and unit change in Oxford score - TKR comparison.

Change in SF-12 Physical and Mental scores.

Change in SF-12 Physical and Mental scores - TKR comparison.
Change in flexion, extension and range of movement.
When re-analysing the data to take into account the difference in patella resurfacing percentages between the Journey II and the other two implants, the outcomes remained the same with a significantly greater flexion and range of movement for the Journey II as compared to both the Genesis II (p = 0.001 and 0.002) and the Profix (p < 0.001 and p < 0.001) but not between the Genesis II and the Profix (p = 0.164 and 0.542). Similarly when re-analysing the extension data accounting for patella resurfacing, both the Journey II and the Genesis II showed significantly improved extension when compared to the Profix (p = 0.035 and 0.011) but there was no difference when comparing the Journey II to the Genesis II (p = 0.962). Hence, resurfacing the patella in the Journey II did not alter the differences in flexion or extension when compared to the other two implants (Figures 5 and 6). JOURNEY II BCS zircoium and CR-angled view. JOURNEY II BCS zirconium-exploded view.

Discussion
This paper has shown that when comparing three knee replacements of different design philosophies and different surface bearings, there was no difference in functional outcome scores at a minimum of 2 years post-operatively, although the Journey II showed a significant improvement in post-operative flexion and range of movement over the other two arthroplasties. In addition, there were no measurable differences for those which had the patella resurfaced compared to those that were unresurfaced (Figure 7). Profix CR.
The Journey BCS total knee replacement was designed to replicate the normal kinematics of the knee with the intention that this would produce better patient outcomes. When it was replaced by the Journey II in 2012, the design principles were maintained but the cam and peg construct was improved, with the cam re-positioned superiorly and the post increased in height and placed more anteriorly, coupled with slight smoothing of the lateral femoral contour. These changes rendered the risk of dislocation negligible. 1 The polyethylene insert was maintained with a concave medial but convex lateral surface and the joint line was kept angled at a three degrees varus. The knee redesign replicated both anterior and posterior cruciate function throughout the full range of movement; the risk of patella impingement was addressed; near-anatomical femoral roll-back was achieved with reduction in iliotibial band and iliotibial-patellar band tension. Finally the tibial post height reduced patellar impingement in flexion, while maximising the dislocation safety factor. These design features produced a knee that was described as having ‘guided motion’ to produce normal kinematics, having a better range of motion and improved stability which should in theory produce an implant that provides better functional outcomes than the previous arthroplasties, such as the Genesis II or Profix, which at the time of their release were innovative in their design features.1,2,3,13,15,16,21,22 This would appear to hold true with the original Journey BCS implant, with Victor et al. showing axial rotation patterns similar to the normal knee but less in magnitude in 86 patients by assessing in vivo kinematics using fluoroscopy during weight-bearing deep knee bend. However there were variations between surgeons suggesting that the outcome is surgical technique dependant. 21 Certainly in our study we showed that the Journey II had better flexion and range of movement that either of the other two implants and this did not vary as to whether the patella was resurfaced or not.
The zirconium/niobium metal alloy consists of 97.5% zirconium and 2.5% niobium which is oxidised at 500 degrees Celsius to produce a 5um thick surface that is approximately 4,500 times harder than a cobalt-chromium equivalent. 23 The alloy demonstrates a decrease in both adhesive and abrasive wear with any scratches that occur on the surface being shallower and smoother than the equivalent on a cobalt-chromium implant. This leads to a reduction both in number and size of polyethylene particles that arise as a result of movement between the two surfaces. It was postulated that this would produce less wear and a longer lasting implant, hence could be used in younger patients or those with greater functional demand. Hence the bearing surfaces may not improve function compared to other implants, as we have shown, but their use may be relevant when considering the long-term survival of the implant. This cannot be assessed in our study due to the short-term analysis. 4,5,6,8,11,23 Another potential advantage is the lack of demonstrable nickel impurities, potentially allowing its use in the nickel allergic patient. The coefficient of friction in the zirconium/niobium alloy is 50% less than a cobalt-chromium equivalent and perhaps as a result of this Laskin 23 reported a more rapid return to flexion and regaining functional milestone in zirconium/niobium compared to cobalt-chromium implants.
Harris et al. reported on 209 patients with a Journey II implant across 12 sites in the USA with 188 available for 24 months data analysis. 24 The baseline operative and peri-operative data was collected retrospectively with post-operative data for six, 12 and 24 months collected prospectively. Within these limitations on data collection, there was a statistically significant improvement in Knee Society Score. Of those patients with complications, 10 underwent a manipulation for stiffness and three implants were revised – one for deep infection but with only the polyethylene insert and patella button replaced; one for a retained bone fragment; and one for an insert mismatch. None required the femoral or tibial components to be revised producing a revision rate at 24 months of 1.48%. Harris concluded that in the short-term, the Journey II knee replacement ‘appears to be a safe and effective device.’ Ahmed’s paper looked a total of 303 oxidised zirconium/niobium Genesis II knee replacements in 278 patients and recorded 10-year survival rate of 97.1% for revision for any reason using Kaplan-Meier analysis. 25 They noted no revisions for loosening, osteolysis or implant failure. Two were revised for infection and six patients had a secondary patella resurfacing out of the 171 who did not have this undertaken at primary surgery. At 10 years there was a statistically significant improvement in the WOMAC score and whilst pre-op scores were not recorded, the 10-year KOOS scores were consistently high indicating a high level of patient satisfaction. They concluded that the oxidised zirconium femoral component gave comparable long-term rates of survival and functional outcomes to conventional implants but could not determine whether it led to fewer revisions for polyethylene wear and osteolysis compared to conventional cobalt-chromium to justify its selective use in younger patients. Sanz-Ruiz retrospectively assessed the difference between the original Journey BCS and the LCS total knee replacement. 26 They reported a statistically significant greater post-operative mean range of movement and a statistically significant improvement in the functional subsection of the WOMAC score in the Journey BCS but equally there were higher pain levels on the WOMAC score and higher iliotibial band irritation in that implant. The HSS score showed no difference between the two implants.
We undertook this analysis between the three implants to assess whether the theoretical design features of the Journey II and/or the theoretical advantages of an oxidised zirconium/niobium surface would produce better outcomes compared to a more standard anatomically designed cobalt-chromium knee arthroplasty. The results have shown that the Journey II has better change in WOMAC scores as compared to the Profix but not when compared to the Genesis II and that there are no differences when comparing the Oxford scores. This suggests that the WOMAC score may detect a small difference in the design feature of the Journey II compared to an older design but that the zirconium/niobium surface may not be a factor.
We showed improvement in flexion and range of movement in the Journey II over both the other two implants. Both the Journey II and Genesis II showed an improvement in extension compared to the Profix. As range of movement is largely determined by flexion rather than extension then it is to be expected that the former would improve if the latter did. This could be attributed to either the design of the Journey II implant or due to patella resurfacing in that implant. The Profix knee replacement was designed to be ‘patella-friendly’ with a femoral component designed for compatibility with the native patella so that the standard teaching was that the patella did not require resurfacing. 27 In line with this philosophy, we routinely did not resurface the patella unless in cases of extreme patella mis-shape or mal-tracking. This is seen in the data when only one of the 107 implants had the patella resurfaced. Similarly, the patella was not routinely resurfaced when the Genesis II was introduced as is seen with an 8% primary resurfacing rate. The Journey II, being a bicruciate stabilised knee, appears to fair better with the patella resurfaced and this is demonstrated in a previous study form our institute with 69% of the implants having a patella button in place. 1 However in this current study, whilst there was considerably more patellas primarily resurfaced in the Journey II group than the other two implants, the differences between these prostheses with regard to flexion and range of movement - better in the Journey II when compared to the other two - was independent of whether the patella was resurfaced. This data, coupled with our previous work, 1 suggests that whilst the Journey II outcomes are better when the patella is resurfaced, the improvement in range of movement over the other two arthroplasties are more to be attributable to its design rather than whether the patella is resurfaced. Further work is required to assess the role of the patella in the Journey II in more detail.
The differences seen in the Journey II in both flexion and range of movement do not appear to be reflected in the functional outcome scores with only a significant difference seen between the Journey II and Profix for adjusted mean change in WOMAC score. This could be because the Oxford and WOMAC scores are based mainly on day to day functional activities that would not require deeper flexion such as ascending stairs, shopping, walking and rising from a chair. Deep flexion might improve higher level activities such as lunge, deep step, stepping over obstacles, riding a bicycle and crouching. Hence the WOMAC and Oxford scores may not be sensitive enough to reflect an improvement in flexion in the activities they measure.
The Genesis II cohort were significantly older than the other two cohorts however there was no difference in any outcome score or movement analysis between this cohort and either the Journey II or the Profix cohort suggesting that age was not a factor between these three implants. The minimal significant improvement was achieved for all three implants in both WOMAC and Oxford scores but was better for the latter than the former. This may be explained by the required improvement in the Oxford score amounting to 8% whereas for the WOMAC it is 16% hence a high percentage gain required in the latter.
The limitations of this study are the relative small numbers to date with just over 100 in each group. However as the statistical analysis is not close to significance for most outcomes, it is highly unlikely that the outcomes would have been different in a larger cohort of patients. This is a short term outcome analysis and hence medium and long term outcomes cannot be inferred from this study. In addition but for the same reasons, we have made no calculation of survival analysis.
Conclusion
The Journey II, Genesis II and Profix knee replacements represent different design philosophies and different surface bearings; however there is no difference between the three with regard to outcome scores at a minimum of 2 years post-operatively. The Journey II showed a significant improvement in post-operative flexion and range of movement over the other two arthroplasties but there was no difference when comparing those which had the patella resurfaced to those who did not have it resurfaced.
Footnotes
Acknowledgments
Smith and Nephew fund the knee fellow at Liverpool University Hospitals NHS FT. One author(AJAS) had received honorarium from Smith and Nephew for teaching.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.