
Abstract
Purpose
Joint arthroplasty has become increasingly more common in the United States, and it is important to examine the patient-based risk factors and surgical variables associated with hospital readmissions. The purpose of this study was to identify stratified rates and risk factors for readmission after upper extremity (shoulder, elbow, and wrist) and lower extremity (hip, knee, and ankle) arthroplasty.
Methods
All patients undergoing upper and lower extremity arthroplasty from 2008–2018 were identified using the National Surgical Quality Improvement Program dataset. Patient demographics, medical comorbidities and surgical characteristics were examined utilizing uni- and multi-variate analysis for significant predictors of 30-days hospital readmission.
Results
A total of 523,523 lower and 25,215 upper extremity arthroplasty patients were included in this study. A number of 22,183 (4.2%) lower and 1072 (4.4%) upper extremity arthroplasty patients were readmitted within 30 days of discharge. Significant risk factors for 30-days readmission after lower extremity arthroplasty included age, Body Mass Index (BMI), operative time, dependent functional status, American Society of Anesthesiologists (ASA) score ≥3, increased length of stay, and various medical comorbidities such as diabetes, tobacco dependency, and chronic obstructive pulmonary disease (COPD). An overweight BMI was associated with a lower odds of 30-days readmission when compared to a normal BMI for lower extremity arthroplasty. Analysis for upper extremity arthroplasty revealed similar findings of significant risk factors for 30-days hospital readmission, although diabetes mellitus was not found to be a significant risk factor.
Conclusion
Nearly one in 25 patients undergoing upper and lower extremity arthroplasty experiences hospital readmission within 30-days of index surgery. There are several modifiable risk factors for 30-days hospital readmission shared by both lower and upper extremity arthroplasty, including tobacco smoking, COPD, and hypertension. Optimization of these medical comorbidities may mitigate the risk short-term readmission following joint arthroplasty procedures and improve overall cost effectiveness of perioperative surgical care.
Introduction
Joint arthroplasty is becoming exceedingly common in the United States, with approximately 7 million Americans living with either a hip or knee replacement. 1 The rates of joint arthroplasty are expected to continue to increase in the coming years, with an over 100% increase projected in both total hip and total knee replacements in the next 10 years.2,3 Similarly, there has been an exponential increase in the rate of shoulder and elbow arthroplasty that equals or even exceeds the recent increase seen in hip and knee replacements.4,5
Just as the rates of upper and lower extremity arthroplasty have been rising, so have the rates of post-operative readmissions following these procedures. Zmistowski et al. found that 5.3% of patients undergoing hip or knee arthroplasty had an unplanned readmission within 90 days of discharge, whereas Mahoney et al. reported 90-days readmission rates for total shoulder arthroplasty to be 5.9%.6,7 Hospital readmissions not only impact the quality of life of the patient but also consume valuable resources within the health care system. With the current focus on patient outcomes-based metrics and bundled payment models, readmission rates following arthroplasty have a profound effect on hospital quality ratings and reimbursement of hospitals and physicians.8-10
By identifying risk factors for readmission, physicians can better collaborate between medical specialties to optimize patients for surgery and to mitigate existing modifiable peri-operative risk factors through patient-specific interventions. The American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database collects patient data from many participating hospitals nationally. The database contains a large number of patients with various orthopaedic conditions 11 and collects data such as medical comorbidities, pre- and intra-operative surgical variables, and postoperative outcomes, including readmissions. Utilization of the NSQIP database has been shown to not only be associated with improved surgical outcomes, but also has been used to advance clinical standards of care.12,13
The purpose of this study was to evaluate the readmission rates of patients undergoing upper and lower extremity arthroplasty, as well as to identify and analyze the risk factors for readmission. Although previous studies have evaluated the risk factors for post-arthroplasty readmission,14-20 none have analyzed a population containing patient-based characteristics and surgical variables as large as the NSQIP dataset while encompassing comparison of upper and lower extremity arthroplasty.
Methods
NSQIP data from 2008–2018 were obtained, and patients were identified based on Current Procedural Terminology (CPT) code. CPT codes for upper joint arthroplasty included 23470 (shoulder hemiarthroplasty), 23472 (total shoulder arthroplasty), 25446 (total wrist arthroplasty), and 24363 (total elbow arthroplasty); those for lower joint arthroplasty included 27130 (hip arthroplasty), 27438 (patellofemoral arthroplasty), 27446 (unicompartmental knee arthroplasty), 27447 (total knee arthroplasty), and 27702 (total ankle arthroplasty). Surgical data, including American Society of Anesthesiologists (ASA) classification, type of anesthesia, operative time, and postoperative time to discharge were collected. Patient demographics and medical comorbidity data were also gathered.
Univariate logistic regression analysis was performed to determine the effect of different risk factors on postoperative hospital readmission. The independent variables with univariate analysis p-values of <0.2 were further analyzed with multivariate logistic regression. We discretized the continuous variables based on previous studies and reports to improve interpretation in our multivariate regression analysis. Body mass index (BMI) was categorized based on the WHO classification for weight status as follows: <18.5 kg/m2 (underweight), 18.5 kg/m2–24.9 kg/m2 (normal weight), 25 kg/m2–29.9 kg/m2 (overweight), 30 kg/m2–34.9 kg/m2 (Class I obesity), 35 kg/m2–39.9 kg/m2 (Class II obesity), and >40 kg/m2 (Class III obesity). Age variable was categorized based on a study by Fang et al. 21 As follows: less 50 years of age, 51–60 years of age, 61–70 years of age, 71–80 years of age, 80 years of age or greater. Length of stay was also discretized to less than 2 days and 2 days or more. Operative time was categorized as: (1) operative time +/− one standard deviation from the mean; (2) operative time between +/−1 standard deviation AND +/− 2 standard deviations from the mean; and (3) operative time greater than +/−2 standard deviations from the mean. In order to be included within Multivariate analysis, variables must have been reported in at least 80% of the cohort. The performed surgical procedure was added to the multivariate analysis in order assess for the common effects associated with 30-days readmission among the upper extremity arthroplasty group and among the lower extremity arthroplasty group. Odds ratios (OR) with 95% confidence intervals (CI) are reported for both analyses. Odds ratios with CI not crossing 1.0 coupled with a p-value <0.05 were considered significant. The C-statistic was utilized to measure discriminative capacity, and the Hosmer and Lemeshow Goodness of Fit Test was employed to assess model calibration.
Results
Summary statistics of patient population who underwent upper or lower extremity arthroplasty.

Summary statistics demonstrated sample size and 30-days readmission rates per procedure performed.

Results of univariate logistic analyses for the influence of risk factors on readmission for lower extremity joint arthroplasty.

Significant Results of Multivariate Logistic Analyses for the Influence of Risk Factors on Readmission for Lower Extremity Joint Arthroplasty. C statistic = 0.627.

*Mean = 92.23 min, standard deviation = 38.14 min.
Other factors associated with 30-days readmission for lower extremity arthroplasty patients included: partially dependent functional status (OR 1.658 95% CI: 1.533, 1.794; p < 0.001), totally dependent functional status (OR 1.547 95% CI: (1.092, 2.191; p = 0.014), and ASA classification ≥3 (OR 1.302 (1.264, 1.342); p < 0.001). In descending severity of risk, medical comorbidities that were identified as factors for readmission include the following: chronic obstructive pulmonary disease (COPD), presence of pre-operative open wound, chronic steroid use, bleeding disorder, dyspnea at rest, smoking, dyspnea at exertion, diabetes mellitus, and hypertension (Table 4). Patients who underwent total ankle arthroplasty (OR: 0.500 95% CI: 0.341, 0.734; p=<0.001), and uni-compartmental knee arthroplasty (OR: 0.771 95% CI: 0.688, 0.863; p < 0.001) had lower odds of 30-days readmission when compared to patients who underwent total knee arthroplasty; whereas patients undergoing total hip arthroplasty had higher odds of 30-days readmission when compared to total knee arthroplasty patients (OR: 1.089 95% CI: 1.057, 1.121; p < 0.001).
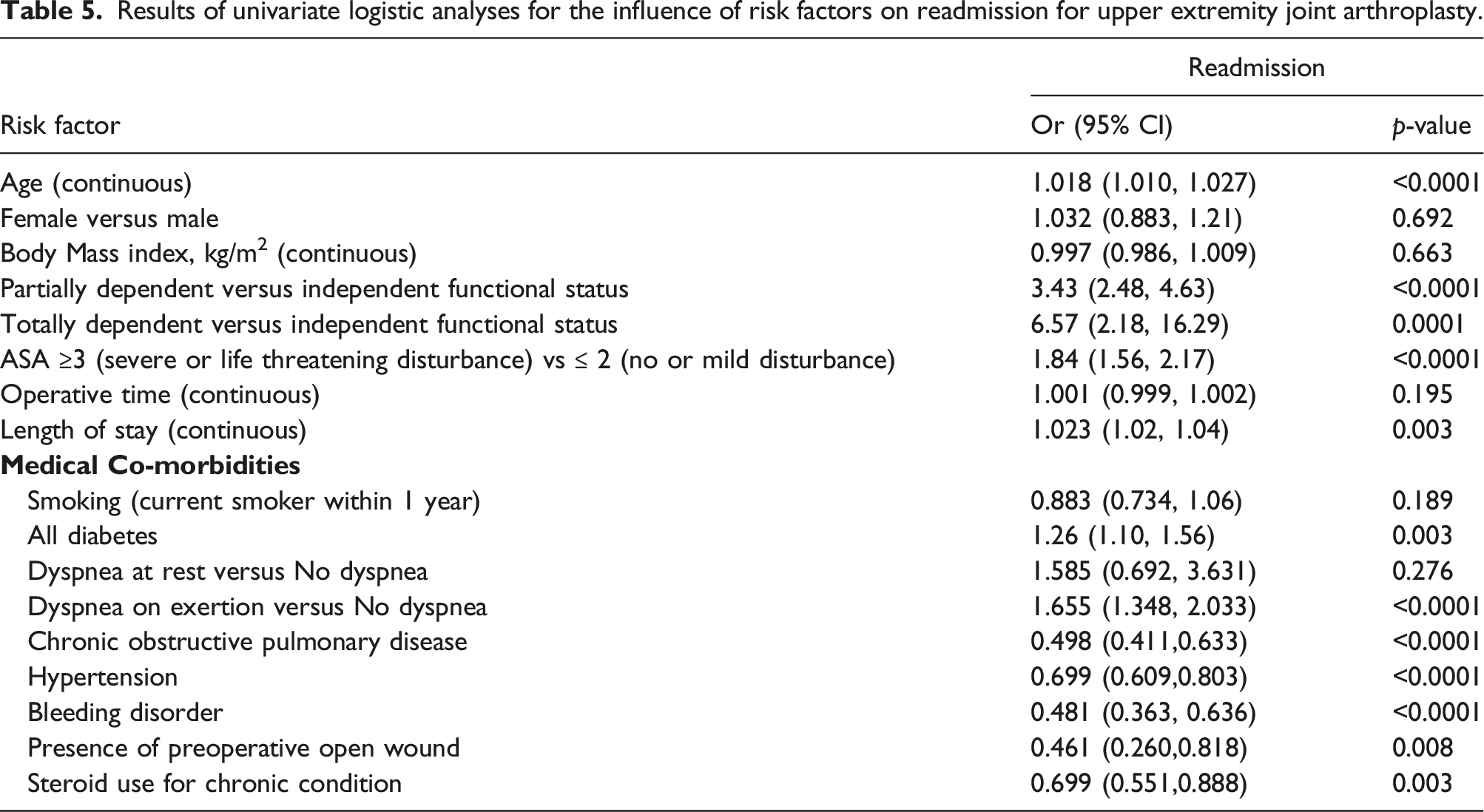
Results of univariate logistic analyses for the influence of risk factors on readmission for upper extremity joint arthroplasty.
Significant results of multivariate logistic analyses for the influence of risk factors on readmission for upper extremity joint arthroplasty. C-statistic = 0.623.
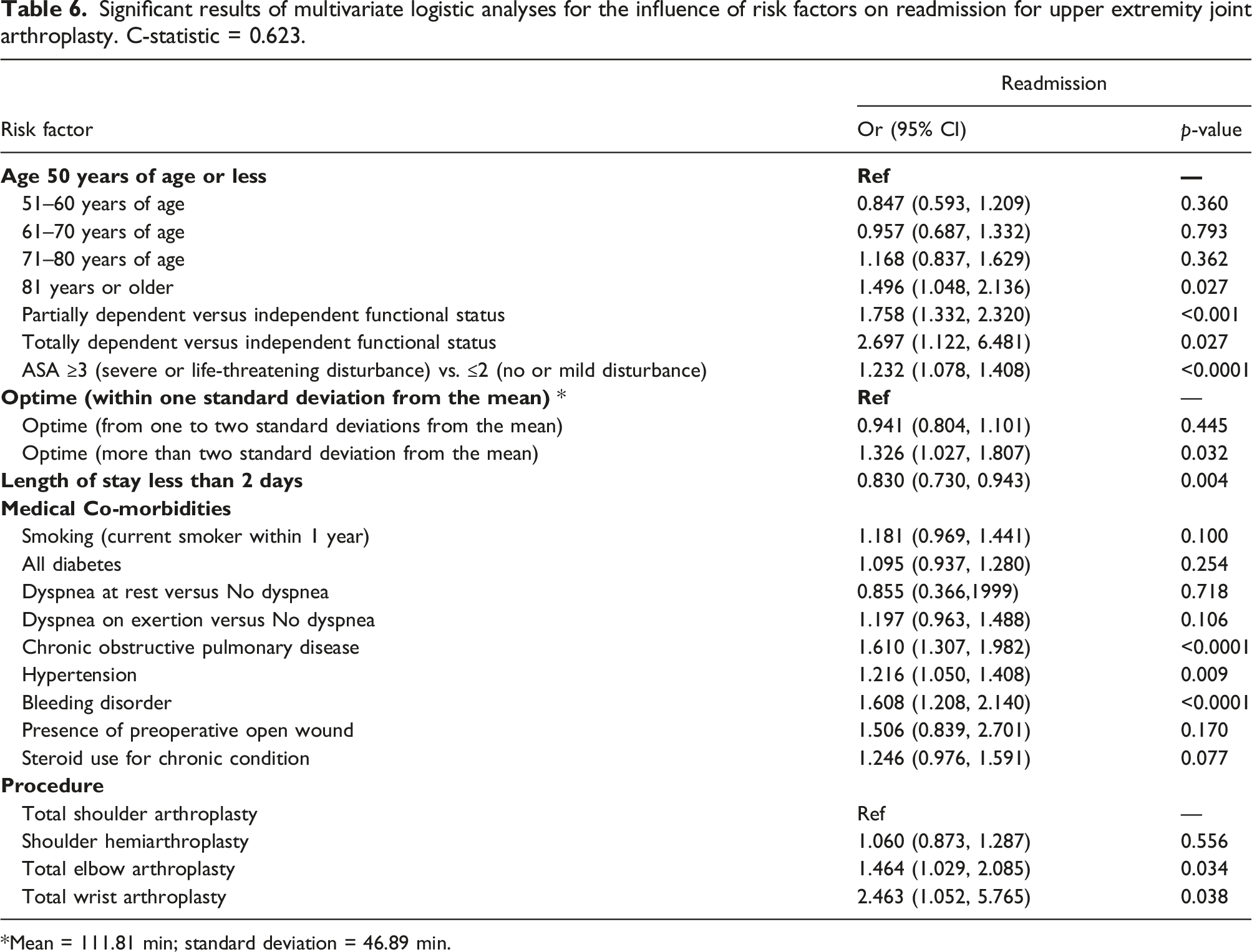
*Mean = 111.81 min; standard deviation = 46.89 min.
Discussion
With the increasing emphasis on outcomes-driven ratings and reimbursement in the contemporary healthcare model, it is important for hospitals and physicians to identify the risk factors and potential mitigation strategies for readmissions. This study reveals that approximately one in 25 patients with upper or lower extremity arthroplasty will experience unplanned hospital readmission within 30-days of index surgery. Furthermore, the current results identify several modifiable risk factors for postoperative readmission rates, while also highlighting similarities and differences in these between lower and upper extremity arthroplasty.
For lower extremity arthroplasty procedures, age, sex, BMI, operative time, functional status, ASA Classification, length of stay, and specified medical comorbidities were identified as independent risk factors for readmission in our study. Previously, older age, male sex, higher BMI, and increased length of stay were found to be independently predictive of post-arthroplasty readmissions.7,16,18,22-26 This study found that a dependent functional status is an additional risk factor. Patients who are functionally dependent or admitted from a chronic care facility may be deconditioned or less mobile, potentially predisposing them to adverse clinical outcomes. A multidisciplinary care approach including discussion with patients and caregivers before and after surgery of their goals and anticipated post-operative rehabilitation plan may help reduce some unanticipated hospital readmissions.27,28
Increased operative time was identified as an independent risk factor for readmission after lower and upper extremity arthroplasty. Longer operative time may be reflective of surgeon experience and/or volume, which have been previously shown to be risk factors.18,29 Furthermore, operative time may also reflect the degree of surgical complexity which should be identified, discussed with the patient, and stratified in the outcomes-driven health care system.
The highest categories of BMI were identified as risk factors for readmission after lower extremity arthroplasty in the current study. However, there was no association between BMI and readmission for upper extremity arthroplasty. BMI has been previously identified as a risk factor in lower extremity arthroplasty for postoperative wound complications, infection, and readmissions,30-33 but previous work in upper extremity arthroplasty have not found BMI to be a risk factor for readmission.34,35 One explanation may be that higher BMI increases the risk of upper extremity arthroplasty failure from instability, which is a longer-term outcome that may not be represented in the 30-days readmission rate. In total shoulder arthroplasty, disproportionate truncal obesity and/or pannus formation alongside the increased extremity weight are thought to lead to an increased risk for implant loosening, instability or dislocation, and mechanical failure over time.36-38 An interesting finding in our analysis was the protective setting of an overweight BMI, which was associate with a lower odds ratio of 30-days readmission compared to normal BMI in lower extremity arthroplasty. Previous studies have found decreased acute complication rates following total hip arthroplasty and have termed this the “obesity paradox”.39,40 Our results assessing 30-days readmission rates in lower extremity arthroplasty show a similar finding, and further studies are needed to decipher the exact reasoning for this.
One possible explanation for the difference between risk factors for upper and lower extremity arthroplasty readmissions is the cause for readmission. Medical complications such as deep vein thrombosis or pneumonia cause the majority of readmissions after total shoulder arthroplasty, with surgical complications such as infection or dislocation responsible for a minority (18%–33%) of readmissions.14,41 Interestingly we found that diabetes was a risk factor for readmission following lower extremity arthroplasty, but not upper extremity arthroplasty. This is consistent with other published studies which have shown diabetes as a risk factor for readmission following total hip and knee arthroplasty 42 but not following total elbow or shoulder arthroplasty.43,44 The exact reasoning for this finding is unclear and further studies are needed to better define the role of diabetes, perioperative glucose control, and target thresholds for hemoglobin A1c on readmission after joint arthroplasty.
Limitations of this study are primarily due to the selected information available through the NSQIP database. Data on the health and functional status among readmitted patients was not consistently reflected, as there may be some readmissions for rehabilitation given that dependent functional status was found to be independent risk factors. In turn, differences between the specific arthroplasty procedures in individual length of stay and rehabilitation, as well as those that deviate from the norm, may impact readmission and represent an area of future study. Additionally, the severity and treatment of patients’ disease and comorbidities are unknown. The current database only tracks readmissions within 30 days of arthroplasty, so readmissions at more extended timepoints were not accounted for. Lastly, some of the differences in readmission rates may be related to the sample size and statistical power, as lower extremity arthroplasty occurs at an order of magnitude greater than those of the upper extremity.
Conclusion
This study represents the latest comparative analysis of 30-days readmission rates and independent risk factors for readmission following upper and lower arthroplasty. Nearly one in 25 patients undergoing upper and lower extremity arthroplasty experiences hospital readmission within 30-days of index surgery. There are several modifiable risk factors for 30-days hospital readmission shared by both lower and upper extremity arthroplasty including COPD and hypertension. Optimization of these medical comorbidities may mitigate the risk short-term readmission following joint arthroplasty procedures regardless of the arthroplasty type and improve overall cost effectiveness of perioperative surgical care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.