
Abstract
Background
The anatomical positioning of the graft during anterior cruciate ligament reconstruction (ACLR) is of great significance for restoring normal knee kinematics and preventing early joint degeneration. Therefore, the adjustment of the mispositioned guide pin becomes extremely important. Our research aims to test the time-zero biomechanical properties in adjusting inaccurate guide pins to the center of the tibial footprint in anatomical anterior cruciate ligament single-bundle reconstruction.
Methods
Porcine tibias and bovine extensor tendons were used to simulate a transtibial ACL reconstruction in vitro. Load-to failure testing was carried out in 4 groups: control group (n = 45): the guide pin was drilled at the center of the ACL footprint; group I, group II and group III (n = 45, respectively): the guide pin was respectively drilled 1 mm, 2 mm and 3 mm away from the center of the ACL footprint. In the experimental groups, a small tunnel with a 4.5 mm reamer is made and the guide pin is shifted to the center of the footprint. All the reamed tibias were scanned by CT to measure the area of the tunnel in the footprint, and time-zero biomechanical properties were recorded.
Results
All graft-tibia complexes failed because the grafts slipped past the interference screws. Compare to control group, the ultimate load, yield load, and tunnel exit area in group III decreased significantly (p < 0.05). Regarding to the ultimate load, yield load, tensile stiffness, twisting force and tunnel exit area, t-test showed no significant differences between control group and group I, group II respectively (p > 0.05). Pearson test showed that tunnel exit area was negatively correlated with other characteristics (p < 0.05).
Conclusions
Surgical adjustment of the guide pin to the center of the tibial footprint may have significant influence in time-zero biomechanical properties in anatomical anterior cruciate ligament single-bundle reconstruction when the adjusted tibial tunnel was significantly enlarged compare to the standard tibial tunnel.
Keywords
Background
Anterior cruciate ligament reconstruction (ACLR) has been used in patients with ACL-reconstructed knee deficiencies, to improve the knee stability and prevent long-term joint degeneration. 1 Currently, accurate anatomic positioning the graft is under raising consideration in ACLR techniques.2,3 That is, anatomic tunnels were proven to restore near-normal anteroposterior (AP) and rotational stability to the knee by biomechanical research, and clinically superior outcomes compared to traditional isometric tunnel positioning.4,5
Therefore, the accurate positioning of the tunnel is crucial in achieving anatomic ACLR, which demands to place tunnels in the center of the native ACL footprint. Though current reconstruction surgeries also focus on anatomic replacement, significant postsurgical tibial tunnel misplacement remains questioning. Previous studies reported that only around 25% of patients had maximal (100%) overlap between the native tibial footprint and tibial tunnel after ACLR. 6 Nevertheless, improper surgical technique may continue to be a leading cause of failure of ACL surgery.4,7,8
As known, misplacement of the guide pin is one of the fundamental causes of tibial tunnel misplacement. Thus, correction of the misplaced guide pin to the center of the footprint is important for further anatomical ACLR. 1 Previous studies1,9 have developed a technique for adjusting inaccurate drill guide placement to the center of the tibial footprint in anatomic single-bundle ACLR, which can solve the inaccurate drill guide placement problems that may be encountered during this surgical procedure. However, surgeons often agitate that this technique may enlarge the tibial tunnel, affecting the stability of the graft and ultimately inducing the failure of ACLR reconstruction. However, the affection of such adjustment on the biomechanics properties of tibial tunnels has not been researched before. Therefore, in this study we aimed to test the time-zero biomechanical properties of tibial tunnel adjustment technique in vitro. We hypothesis that: (1) this technique will enlarge the tibial tunnel diameter; (2) there is significant difference in the biomechanical properties of the tibial tunnel after this surgically adjusting during ACL reconstruction.
Method
This experiment was approved by the Regional Ethics Committee of our hospital.
Whilst, previous studies have revealed that porcine tibias showed similar biomechanical properties to young adult human tibias and bovine extensor tendons have similar viscoelastic, structural, and material properties to human tendons.10,11 Consequently, the combination of the porcine tibias and extensor tendons provide good surrogates of human tissues in ACLR investigation. 12
On the basis of the ultimate load with tibial fixation of the graft after ligament reconstruction, 13 a pre-study power analysis was performed. To achieve a power of 0.80 with an α of 0.05, 45 specimens were required in each group, 14 resulting totally 180 porcine tibias (age: 11 ± 2.7 months) and 180 bovine tendons used in this study to establish the model of transtibial ACLR in vitro. Both the tibias and tendons were stored at −20°C. The tibias and tendons were thawed to room temperature 12 hours before specimen preparation.
Graft preparation
All soft tissues were dissected and removed from the bovine extensor tendons. Then, the tendons were trimmed and folded in half to produce a 2-stranded soft-tissue graft (i.e. 85 mm in length and 8 mm in diameter). Following the same methods from previous studies, grafts were adjusted to the tunnel diameter until modest resistance was felt when the tendon was put into the tunnel of 8 mm.13,15 The length of grafts was controlled within internally 40 mm in tibial tunnel and 45 mm externally (i.e., 25 mm for fixation by the testing machine and 20 mm for free). All grafts were subjected to 20 N of pretension for 10 minutes to eliminate viscoelasticity. The ends of the grafts were whipstitched with No. 2 Ethibond suture (Ethicon, Somerville, NJ) in a similar fashion (11 stitches with a length of 40 mm). Then, the grafts were wrapped in 0.9% saline solution-soaked gauze until use.
Tibial tunnel groups and fixation techniques
All the tibias were cut to a residual length of 15 cm. Then the tibias were divided into four groups (Figure 1). As reported,
15
the tibial tunnel was made by utilizing a tibial drill guide aimer (Acufex Director Drill Guide, Smith and Nephew, Andover, MA), inserted at 55° from the standard anteromedial portal. Then, A guide pin (2.0 mm) was drilled from the anteromedial aspect of proximal tibia passing through the tibial footprint. In the Control group (n = 45): the guide pin was drilled at the center of the ACL footprint. In the Experimental groups: Group I (n = 45): the guide pin was drilled 1 mm away from the center of the ACL footprint. Group II (n = 45): the guide pin was drilled 2 mm away from the center of the ACL footprint. Group III (n = 45): the guide pin was drilled 3 mm away. Then we reamed the tibial tunnel with a smaller diametric reamer (4.5 mm) to create a separate and small tunnel particularly in the experimental groups. A straight clamp was used to secure the tip of the guide pin. Gradually, we attempt to shift the center of the tunnel toward the center of the tibial footprint and finally, all the tunnels was reamed with a 8.0 mm reamer to match the graft’s diameter. All tunnels were 50–55 mm in length and nearly 8.0 mm in diameter. We cleared the bone debris within the tunnel to avoid damage to the graft. The bone mineral density (BMD) of the porcine tibias was assessed using dual-energy X-ray absorptiometry to eliminate the influence of BMD on fixation strength. Indication of control and experimental groups. Representation of adjusting the eccentrically placed guide pin in the anterior cruciate ligament tibial footprint.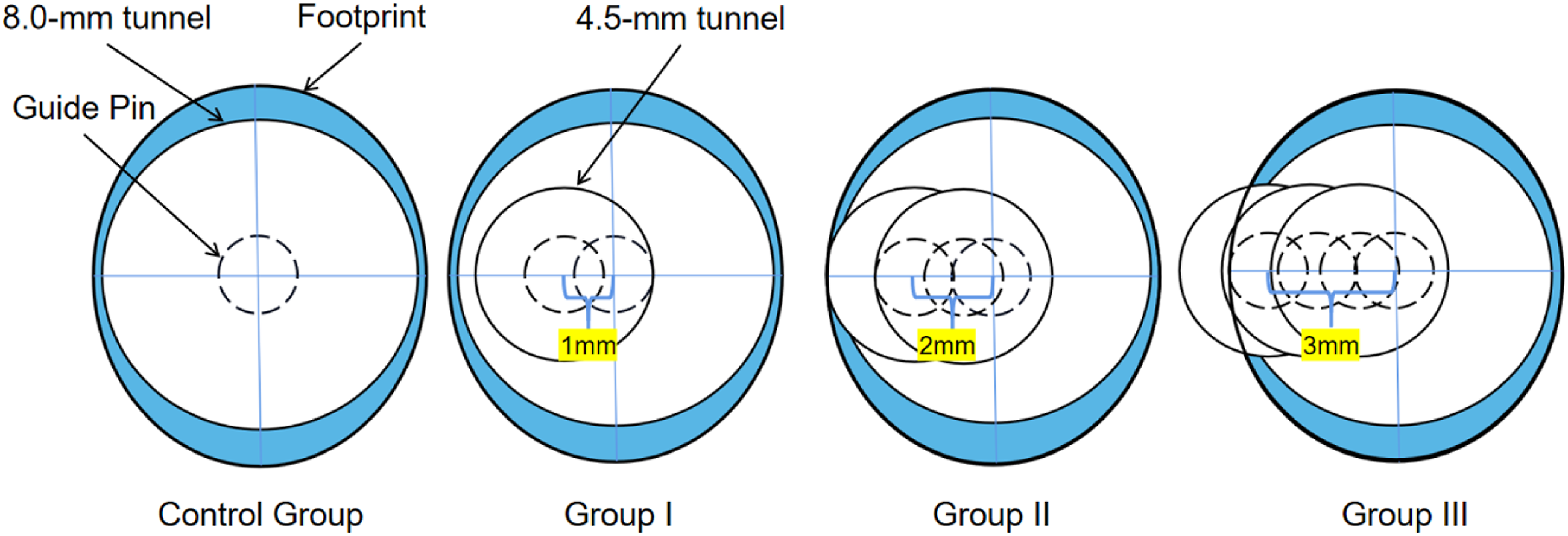
Before the biomechanical experiment, all the drilled tibias were scanned with computerized tomography (CT) to measure the area of the tunnel in the footprint (Figure 2). After the pulling graft through the tibial tunnel, an 8 × 25 mm titanium disposable interference screw (Guardsman; ConMed Linvatec, Largo, FL) was inserted between the graft and the tunnel along a guidewire, aligning the screw tail with the anterior tibial bony cortex (corticocancellous screw fixation).
16
The aforementioned process was collaboratively completed by the same surgeon team. CT scan of control and experimental groups.
Biomechanical testing
The tibia was fixed in a custom testing jig, and the graft was clamped solidly to a testing apparatus as in Figure 3. The tibial fixation point was 2 cm inferior to the entrance of the tunnel.
12
In an attempt to achieve posterior declination of a normal ACL (about 45°–50°).
17
An electronic universal testing machine (AG-X series vertical machine; Shi madzu, Kyoto, Japan) was used to establish a model of pull-to-failure loading. All grafts were loaded at 10 mm/min to failure. The parameters including load-elongation curve, tensile stiffness (in newtons per millimeter), ultimate load (in newtons), yield load (in newtons), energy absorbed to failure (in joules), and failure mode were recorded. We defined tensile stiffness as the slope of the linear region of the load-elongation curve. Ultimate load and yield load were determined by the load-elongation curve. Energy absorbed to failure was determined by the maximum working capacity of the testing machine in the process. All these data were collected by Trapezium X software. The modes of failure were monitored by visual observation. Biomechanical test setup.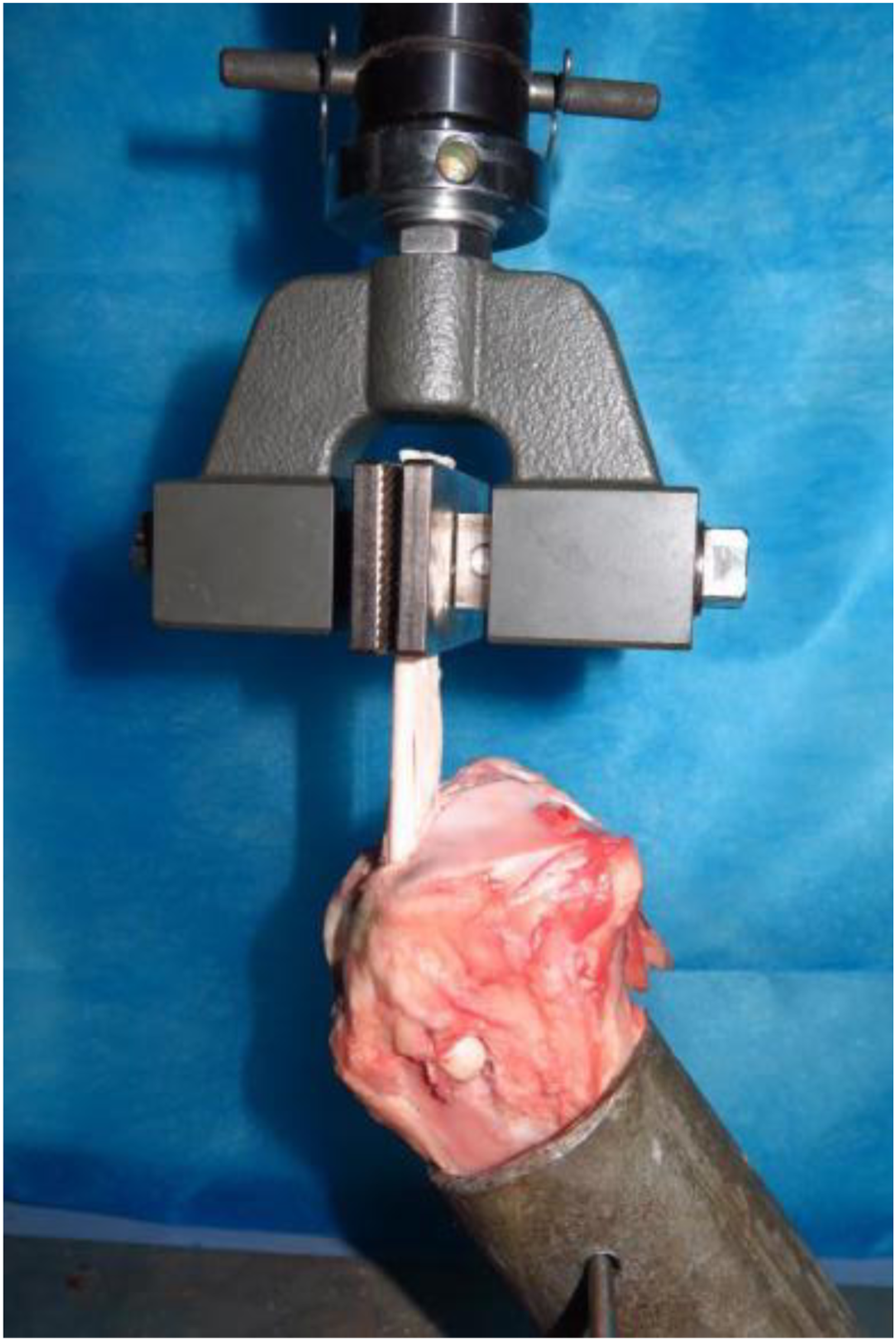
Statistical analysis
Statistical analysis was performed in software Prism 9 (Version 9.2.0). T-test was used to test the mean differences between control group and experimental groups respectively. Pearson test was used to analyze the correlation between tunnel exit area and other characteristics. p < 0.05 was set to be statistically significant.
Results
Basic characteristics of graft and tibia
Basic characteristics of specimens.
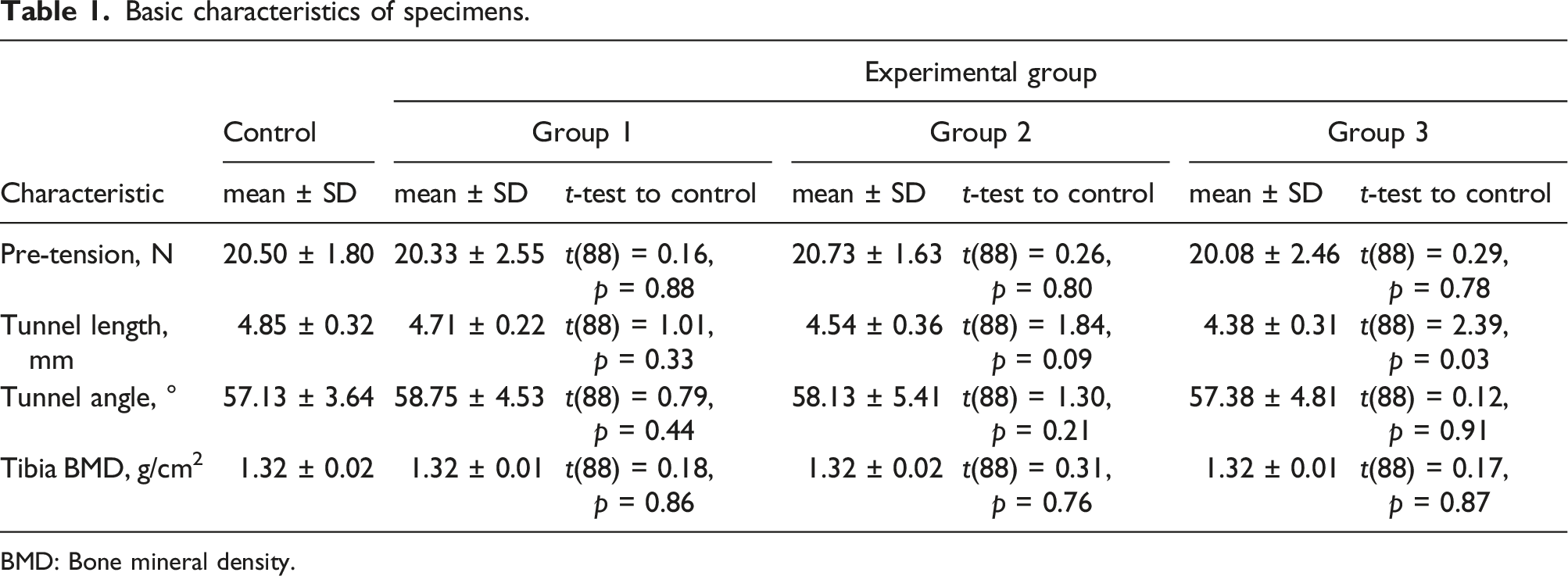
BMD: Bone mineral density.
Outcomes of biomechanical testing
No differences were found in modes of failure. All graft-tibia complexes failed by the grafts slipping past the interference screws.
Biomechanical properties of graft-tibia complexes.

Discussion
The most important findings of our study were that this surgical adjusting technique may influence the time-zero biomechanical properties during transtibial ACL reconstruction. In this study, a single-bundle ACL graft was used to simulate an in vitro model of transtibial ACL reconstruction. The results of our study showed the time-zero biomechanical properties in terms of ultimate load and yield load decreased when the adjusted distance was more than 3 mm away of the center of footprint of ACL. The results of our study confirm our hypothesis: (1) such surgical adjusting technique may enlarge the tibial tunnel in ACL reconstruction; (2) the biomechanical properties will be affected when the final tibial tunnel produced by such surgical adjusting technique was significantly enlarged compare to that of the standard tibial tunnel.
The incidence of ACLR surgeries is increasing and so is the number of ACLR failure, and the failure can be broadly grouped into surgeon, patient, and biological factors, and surgeon-related or technical factors is the most common reason for ACLR failures. 18 In Jaeckers’s series of 167 patients with failed ACLR, technical errors were found in 64.5%. Malpositioned tunnels of ACLR may lead to inadequate restoration of stability (especially rotational) and graft impingement with the roof of the intercondylar notch, posterior cruciate ligament (PCL) or lateral femoral condyle.19,20 While inadequate rotational stability predisposes the graft to mechanical failure, graft impingement can cause attritional rupture or interfere with biological healing. Hence, the anatomical placement of the graft within the anatomical ACL footprint plays a crucial role in the success of single-bundle ACLR. However, it is not always possible to ream the guide pin into the center of the ACL footprint, and making it difficult to redrill the tunnel, as well as delaying time of the operation. This technique is able to eccentrically place the tibial guide pin into the center of the tibial footprint without the need for additional redrilling.
Although such adjustment brings us some intraoperative convenience, a significant misplacement of the pin may require a classic corrective step, otherwise it will enlarge the tunnel. So that the best adjustment is that the adjusted tunnel is included in the final tunnel in order that the tunnel will perfectly match the graft. If the diameter of the final tunnel is 8.0 mm, considering the guide pin diameter is 2 mm, the maximum acceptable adjusted distance is 1.75 mm when operated with a 4.5 mm reamer. Thus, if the diameter of the final tunnel are 9 mm and 11 mm, the maximum acceptable adjusted distance 2.25 mm and 3.25 mm respectively (Figure 4). The maximum adjustment distance varies with the diameter of the tunnel.
Additionally, while using this technique for adjusting the guide pin within the ACL tibial footprint in single-bundle ACLR, 1 the guide pin is held by a clamp, and which may result in toggling of the guide pin within the tunnel and producing metal particles while reaming. Large metal particles show a risk of direct mechanical abrasion of articular cartilage. Moreover, Pedowitz et al. 21 finds that metallic microparticles could induce intra-articular damage through a synoviocyte-mediated cytokine response if their concentrations reach clinically significant levels. Therefore, once the correct position of the center is achieved, the guide pin is fixed in the femoral notch roof to guarantee the accurate correction of the axis, without toggling of the guide pin inside the tunnel and metal dusting.
Limitations
There were some limitations in our study. First, a main limitation of this biomechanical study was that we only focused on the time-zero outcomes and did not perform cyclic loading, which was used to simulate the postoperative rehabilitative process. This might have an important effect on the biomechanical properties of the graft during the postoperative period. Second, a titanium interference screw was selected to fix the graft instead of bio-interference screws or PEEK (polyether ether ketone) screws, which are commonly used in clinical practice. One reason was that the titanium interference screw was commonly used in biomechanical studies of soft-tissue graft tibial fixation.22,23 Moreover, Aga et al. 9 have observed no significant differences in soft-tissue fixation properties among the 3 screw materials.
Conclusions
Surgical adjustment of the guide pin to the center of the tibial footprint may significantly influence in time-zero biomechanical properties in anatomical anterior cruciate ligament single-bundle reconstruction when the adjusted tibial tunnel was significantly enlarged compare to the standard tibial tunnel.
Supplemental Material
Supplemental Material - Surgically adjust tibial tunnel in anatomical anterior cruciate ligament single-bundle reconstruction: A time-zero biomechanical study in vitro
Supplemental Material for Surgically adjust tibial tunnel in anatomical anterior cruciate ligament single-bundle reconstruction: A time-zero biomechanical study in vitro by Hong Wang, Yuanjun Teng, Bo Peng, Gengxin Jia, Hua Han, and Yayi Xia in Journal of Orthopaedic Surgery.
Footnotes
Author contributions
Y X, H H designed and performed the study. H W, B P and G J performed biomechanical test. H W wrote the manuscript and performed the data collection and interpretation. H W and Y T made figures. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The National Natural Science Foundation of China (81874017, 81960403, 82060413, and 82060405); Lanzhou Science and Technology Plan Program (20JR5RA320); Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2017-ZD02, CY2021-MS-A07), and TCM inheritance and Innovation Platform construction project of Lanzhou University Second Hospital (TCM-IPC-2020-05). The funding body made no other contributions to any aspects of this study.
Ethical approval
The protocol for this study was approved by the Scientific Ethics Committee of the Second hospital of Lanzhou University.
Informed consent
All data generated or analyzed during this study are included in this published article.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.