
Abstract
Introduction
Articular cartilage is located at diarthroidal joints throughout the body and creates a smooth, low coefficient of friction. Avascular and functioning in environments of biomechanical stress, articular cartilage may become damaged due to injury, congenital and genetic conditions, and other etiologies leading to further injury, osteoarthritis, pain, and dysfunction.1–5 Due to this, the prevalence of articular cartilage injuries in patients undergoing arthroscopy is known to be high. 2
Widuchowski et al. found significant articular cartilage lesions of the knee in 2931 patients (57.3%, n = 5233) with isolated localized Outerbridge grade 3 and 4 lesions in 5.2%.6,7 They further analyzed 25,124 knee arthroscopies with cartilage lesions as localized focal osteochondral or chondral lesion (67%), osteoarthritis (29%), osteochondritis dissecans (2%) and other types (1%) with non-isolated and isolated cartilage lesions accounting for 70% and 30% respectively. 8 They postulated that candidates for cartilage repair surgery with one to three localized grade III and IV cartilage lesions, under the age of 40 were found in 7% of patients in their study. The prevalence of these cartilage lesions increased from 36% to 38% in high-level athletes with the addition of cartilage injury prevalent in patients undergoing or status-post common procedures such as ligament reconstruction.9–21
Non-operative treatments for articular cartilage lesions created in the form of activity modifications, bracing, physical therapy, and injectables such as cortisone, viscosupplementation, and biologic treatments have seen success, but have been ineffective to restore or regenerate the articular cartilage lesion.22–25,17
Surgical techniques such as Autologous Chondrocyte Implantation (ACI), Matrix Autologous Chondrocyte Implantation (MACI), and particulated juvenile allograft cartilage have been created to regenerate tissue at the lesion site and demonstrate promising clinical results.26,28–35
Osteochondral allografting is a procedure that has been around for decades and has demonstrated consistently good results in the treatment of isolated articular cartilage lesions.36–40 One of the concerns with traditional osteochondral allografting is that a significant amount of recipient bone must be cored out to allow for implantation of the donor graft. In addition, procurement can be problematic with long lead times and limited supplies. Traditional osteochondral allografting can also be difficult to perform technically in areas such as the patella or the trochlea where matching the surface topography of the donor and recipient is challenging. More recently, a thin laser-etched osteochondral allograft (ProChondrix®, Allosource™, CO) has been developed to address some of these concerns.
Like a traditional osteochondral allograft, it contains live donor cells, an intact cellular matrix with proven chondrocyte viability and bone forming cells.10,27
In addition, its ability to be cryopreserved while maintaining chondrocyte viability has been demonstrated and a cryopreserved version has been developed.41,42 Its thin profile allows it to be implanted without compromising the recipient bone either with or without a microfracture being performed.
The graft can also be used in defects with minimal bony involvement (less than 1–2 mm). Thus, it allows for osteochondral allografting of a full-thickness articular cartilage lesion while eliminating the supply issues and the concerns about violating the recipient bone. Its flexibility allows it to be contoured to areas such as the trochlea, patella or acetabulum. In addition, the bone implanted in laser-etched shell osteochondral grafts is thinner, which offers the advantage of reducing the time needed to be resorbed and replaced by viable bone. Initial laboratory testing on ProChondrix® has been performed to demonstrate cell viability and its growth factor profile. It is believed that a cell viability of greater than 70% is important for optimizing the clinical outcome. 43 ProChondrix® has been found to have an average cell viability of 87.5% at 35 days which is the expiration date of the fresh graft. In addition cell functionality has been displayed using a cellular outgrowth model which exhibits cartilage cells growing into a fibrin glue based medium up to several millimeters. 44
This demonstrates that the cells from the graft are metabolically active and can expand into the fibrin glue occupied space. The growth factor levels in ProChondrix® have also been found to be significantly similar to unprocessed fresh cartilage for bFGF, TGFb, PRG4, BMP7 and BMP2. 44 These growth factors are believed to be important in driving mesenchymal stem cells down a pathway towards chondrogenesis. While the basic science and laboratory data around ProChondrix® is promising, the clinical efficacy remains to be demonstrated.
In this study, we examine the short-term results of a novel technique to treat isolated, symptomatic, full-thickness articular cartilage lesions of the knee using a Prochondrix® thin laser-etched osteochondral allograft (T-LE allograft).
Methods
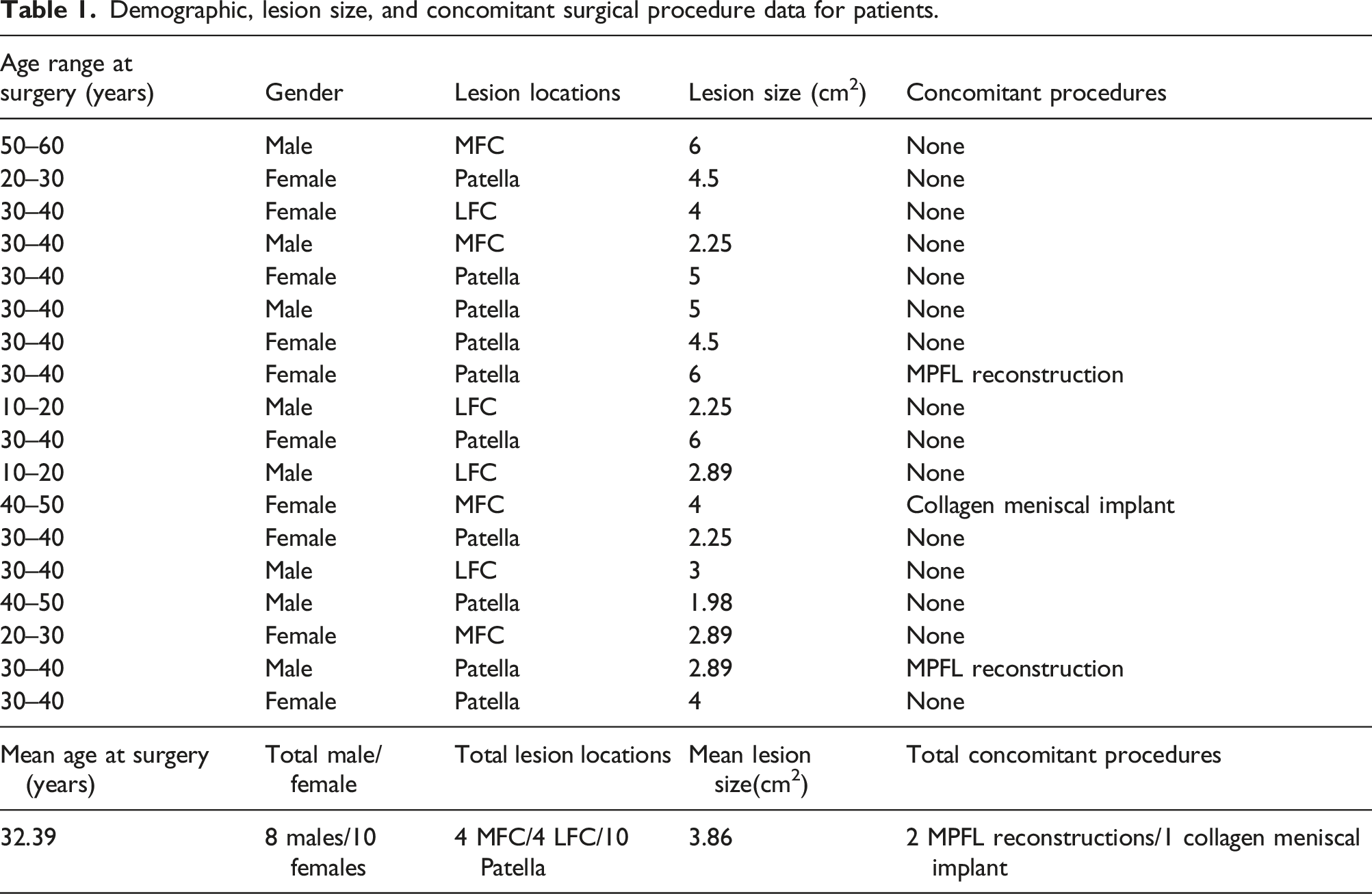
Institutional Review Board approval was obtained prior to beginning this study. Eighteen consecutive patients with symptomatic, full-thickness, articular cartilage lesions of the knee smaller than 30 × 30 mm in size were included in this study. Patients over the age of 60 years old and patients who had lesions with significant bone loss were excluded from the study. The patients were identified retrospectively but outcome data was collected prospectively during the normal pre and post-operative follow-up of these patients. Ten of these 18 patients (56%) involved grade 3-4 lesions of the patella (10% superior, 40% central and medial facet, 40% medial facet, 10% central).
Demographic, lesion size, and concomitant surgical procedure data for patients.
Post-operative MRIs and repeated arthroscopies.

Surgical technique
All surgeries were performed by a single surgeon. A standard parapatellar arthrotomy was used in all cases. No case was performed completely arthroscopically. Once the lesion was identified, it was prepared for microfracture by creating vertical shoulders using a curette and removing the calcified cartilage layer also with a curette.
Standard microfracture was performed using a microfracture awl or non-threaded k-wire. The T-LE allograft was removed from its packaging and gently rinsed in room temperature saline. Fibrin glue was placed at the base of the cartilage defect and next the T-LE allograft was placed on top of this thin layer of fibrin glue. An additional layer of fibrin glue was placed on top of the T-LE allograft to further secure it within the lesion. The knee was taken through a range of motion to assess the stability of the graft and if accessory fixation was necessary. Accessory fixation was performed as deemed necessary using an anchor and suture when the graft did not seem stable enough with fibrin glue fixation alone.
Rehabilitation
Physical therapy was initiated 1 week after surgery and focused on early range of motion using a validated protocol, and specifying the protocol to individual patients as needed. Lesions of the femoral condyle were kept non-weight bearing for a period of 4 weeks where the patient was allowed to partially and fully weight-bear as tolerated by 6 weeks. Lesions of the patella were allowed to weight-bear as tolerated immediately. Physical therapy was also initiated 1 week after surgery focusing on early range of motion. Early flexion was limited for the first 2 weeks and 90 degrees of flexion was not allowed until 6 weeks to avoid stressing the graft.
Statistical analysis
Demographic and intra-operative data was recorded as well as pre- and post-operative International Knee Documentation Committee (IKDC) (MD = 27.33, SD = 19.32,
Short Form-36 (SF-36) was used to measure patient physical function (MD = 32.15, SD = 22.73,
A paired T-test was performed for each patient measuring the difference in pre-operative and post-operative data points for the surveys mentioned. A p-value of 0.05 was used to determine statistical significance. All 18 subjects had a minimum follow-up period of 48 months. Failures requiring reoperation were also recorded.
Results
At a mean follow-up of 2.5 years (6–43 months), statistically significant increases were seen in SF-36 Physical Functioning (+25.20, Pre-operative and post-operative SF-36 scores. Pre-operative and post-operative KOOS scores. Pre-operative and post-operative tegner and VAS scores. Pre-operative and post-operative subjective IKDC scores.



Discussion
In this study we report the early results of a thin, laser-etched osteochondral allograft on the treatment of full thickness cartilage lesions of the knee. We demonstrate good early results as evidenced by significant increases in validated clinical outcome scores and significant decreases in the visual analogue pain scale. These positive results were maintained throughout the course of the study and did not show degradation with time with seventeen out nineteen patients (89.5%) two and a half years post-operatively.
The results are comparable to the short-term results of other cartilage restoration procedures currently in use today
Farr et al. 31 reported the short-term (2 year) results of DeNovo and also reported similar improvements in clinical outcome scores with one graft delamination out of twenty-five patients.
Some preliminary MRI data and second look data was also able to be collected. One patient had a chondral defect to the medial femoral condyle that was treated with ProChondrix® (Figure 5(a)). The ProChondrix® graft was found to be intact and incorporating well with a gross appearance similar to the surrounding articular cartilage (Figure 5(b)). In addition, several patients underwent post-operative MRIs at 3, 6, 12, 18, and 24 months revealing good fill of the lesions, and two patients required a second arthroscopy at 22 and 40 months after their initial post-op (Table 2 and Figure 6). A separate MRI study is underway to formally evaluate the post-operative MRI findings. There were two failures noted during this study. One was due to early graft dislodgement. The case involved a patellar lesion that was treated with a ProChondrix® graft with no accessory fixation. Arthroscopic images of a femoral lesion prior to placement (A). and at 6 Months post-operatively (B). MRI Images of a Lateral Femoral Condyle Lesion Treated with ProChondrix® (Black. Arrow is pointing to treated lesion).

The patient did poorly and underwent a second look arthroscopy and was found to that the graft dislodged adjacent to the lesion (Figure 7(a)). Interestingly, there was still some fill noted in the lesion despite graft dislodgement (Figure 7(b)). The second patient initially did well but as she returned to high level cycling began to experience anterior knee pain similar to prior to the procedure. She subsequently underwent conversion to a patella-femoral arthroplasty. At the time of surgery, a biopsy of her cartilage restoration site was taken which revealed what appeared to be viable articular cartilage (Figure 8). Arthroscopic Images of a Dislodged ProChondrix® Graft (A), The Lesion. Demonstrates some Fill even after Dislodgement (B). Microscopic images of a biopsy from a ProChondrix® treated lesion (H&E staining).

The results are comparable to the short-term results of other cartilage restoration procedure currently in use today. A meta-analysis of osteochondral allografting demonstrated a mean 86.7% survival rate at 5 years with significant improvements in clinical outcome scores. 38 Likewise, MACI has been demonstrated to have similar short-term improvements in clinical outcome scores and similar survival rate (87.5%) at 2 years45,46 Farr et al. 31 reported the short-term (2 year) results of DeNovo and also reported similar improvements in clinical outcome scores with one graft delamination out of twenty-five patients.
While this study demonstrates encouraging early results of the use of ProChondrix® on full-thickness articular cartilage lesions of the knee, it has several weaknesses. Firstly, the sample size is relatively small and performed by a single surgeon. Data was also collected, compiled and analyzed by the same surgeon which introduces a number of biases.
Secondly, follow-up is relatively short. It has been established from other cartilage procedures that short term results can deteriorate fairly rapidly as longer-term outcomes are analyzed. A larger, multi-center study with longer follow-up is necessary to better understand the results of ProChondrix® in a broader population and to help determine its durability over a longer period of time as well as comparing Prochondrix® with other allograft procedures to determine its efficiency as well as with a comparison group. Currently, additional studies are underway to evaluate MRI, biopsy and prospective series evidence to further understand the biology and efficacy of this novel approach.
Lastly, the defects treated in our study are relatively small, focal, contained lesions.
There is no data in our study or in current literature that supports its applicability for larger, uncontained chondral lesions.
Conclusion
This study demonstrates encouraging early outcomes with an acceptable revision rate in the treatment of symptomatic articular cartilage lesions using a laser-etched osteochondral allograft, ProChondrix®. The study shows statistically significant increases in outcome when compared pre-operatively and lends promise to further widespread research and treatment of focal cartilage defects with ProChondrix® and other similar allograft.
Footnotes
Declaration of conflicting interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Mehta reports personal fees from Arthrex, personal fees from Allosource, personal fees from Stryker, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. Allosource donated five ProChondrix grafts that were used in this study.