
Abstract
Background
Surgical techniques related to soft tissue management play critical roles in optimizing surgical outcomes and patient satisfaction in total knee arthroplasty (TKA). Despite the importance of wound closure and bleeding management approaches, no published guidelines/consensus are available.
Methods
Twelve orthopedic surgeons participated in a modified Delphi panel consisting of 2 parts (each part comprising two rounds) from September–October 2018. Questionnaires were developed based on published evidence and guidelines on surgical techniques/materials. Questionnaires were administered via email (Round 1) or at a face-to-face meeting (subsequent rounds). Panelists ranked their agreement with each statement on a five-point Likert scale. Consensus was achieved if ≥70% of panelists selected 4/5, or 1/2. Statements not reaching consensus in Round 1 were discussed and repeated or modified in Round 2. Statements not reaching consensus in Round 2 were excluded from the final consensus framework.
Results
Consensus was reached on 13 goals of wound management. Panelists agreed on 38 challenges and 71 strategies addressing surgical techniques or wound closure materials for each tissue layer, and management strategies for blood loss reduction or deep vein thrombosis prophylaxis in TKA. Statements on closure of capsular and skin layers, wound irrigation, dressings and drains required repeat voting or modification to reach consensus.
Conclusion
Consensus from Asia-Pacific TKA experts highlights the importance of wound management in optimizing TKA outcomes. The consensus framework provides a basis for future research, guidance to reduce variability in patient outcomes, and can help inform recommendations for wound management in TKA.
Introduction
Total knee arthroplasty (TKA) is an effective orthopaedic surgical procedure to address end-stage arthritic conditions, providing pain relief and restoring mobility.1–3 Soft tissue management in TKA encompasses a balance of factors; although the implant itself constitutes a substantial proportion of the total cost of surgery and remains a focus in orthopaedic procedures, 4 surgical techniques related to soft tissue management, and knee positioning during surgery 5 also play key roles in achieving desired surgical outcomes and improving patient satisfaction.6,7
Improper soft tissue handling during surgery can lead to pain, fibrosis, infection, reoperation or other complications,4–5 which have an impact on functional recovery, 8 quality of life and patient satisfaction with TKA, 4 and also lead to a substantial economic burden on the healthcare system. 9 Therefore, optimal wound management, which includes the methods of wound closure as well as bleeding management strategies, is critical for the success of the procedure and in alleviating associated economic burden.
The method of wound closure is important as poorly healing wounds in TKA can lead to complications such as infection and implant failure.10,11 These complications, when matched to uncomplicated primary TKA, can impose significant economic burden to tertiary care and patients in terms of hospital readmissions (e.g. TKA with periprosthetic joint infections [PJIs]: 3.6 days vs 0.1 days for uncomplicated TKA), clinic visits (TKA with PJIs: 6.5 vs uncomplicated TKA: 1.3 days) and costs (TKA with PJIs: $116,383 US dollars [USD] vs uncomplicated TKA: $28,249 USD). 12
Bleeding is a major issue in TKA due to the extensive soft tissue release and bone resection associated with the procedure, 13 and can also lead to significant economic burden. In primary and revision TKA procedures, the presence of thrombotic complications, such as pulmonary embolism and deep vein thrombosis, can result in 30% higher hospitalization costs than those without complications. 4 Additionally, postoperative bleeding in major orthopaedic surgery patients before hospital discharge can increase hospital length of stay and inpatient charges (1.8 days longer and $7,593 USD higher inpatient charges). 14 Complications from bleeding, including hematoma, increased risk of PJI, delayed rehabilitation, protracted hospitalization and blood transfusions, 15 also contribute to significant economic burden.
Aims
To our knowledge, despite the importance of wound management in TKA, there are no specific published guidelines or consensus on this topic. Guidelines are available from the Centers for Disease Control and American Academy of Orthopaedic Surgeons (AAOS) on the prevention of surgical site infections (SSIs), 16 management of SSIs 17 and surgical management of knee osteoarthritis. 18 However, these do not explicitly mention the role of wound closure techniques/materials or methods of bleeding management, and their impact on SSIs or other TKA outcomes.17,18 For those recommendations that do exist, the evidence supporting the majority of them is weak or there is no recommendation and the issue is unresolved. 16
Consensus in the areas of wound closure and bleeding management stands to impact the overall success of TKA by helping to reduce the risk of complications and inconsistencies in surgical outcomes, and by providing a useful guide for future surgical education. To address the information gap, we conducted a modified Delphi panel to determine and consolidate expert consensus, first on key wound closure and bleeding management goals in TKA and the challenges associated with achieving these goals, and second on principles and strategies to address these challenges.
Methods
Selection and qualification of participants
Ten orthopaedic surgeons from 6 Asia-Pacific countries were invited to participate as expert panelists: 3 from China, 2 from Japan, 2 from South Korea, 1 from Thailand, 1 from Malaysia, and 1 from Australia. Panelists satisfied 75–100% of the following criteria: • High-volume surgeon with 50+ TKA cases per annum • Holds a senior position within a hospital and/or a training position • Has exposure to and/or experience with advanced wound closure and bleeding management technologies • Has a strong interest in wound and/or bleeding management, evidenced by authorship of associated publications, or prior domestic or international speaking engagements
A Steering Committee, comprising 2 independent orthopaedic surgeons: 1 from the USA and 1 from Australia, reviewed questions, consensus definitions, and feedback from the panel, and facilitated meeting discussions. The Steering Committee satisfied the above criteria for the expert panel, as well as the criterion of having a strong record of participation in professional meetings. All contacted surgeons provided consent and agreed to participate.
Study design
A modified Delphi method with two parts, each comprising two rounds, was used to establish consensus on the key goals and challenges in wound closure and bleeding management in TKA (‘Delphi part 1: challenges’), and the associated strategies to address these (‘Delphi part 2: strategies’). The Delphi panels took place between 14th September and 13th October 2018.
The first-round questionnaire of Delphi part 1: challenges, was conducted through an online platform (SurveyMonkey) via email. All subsequent rounds were conducted through the same online platform at a face-to-face meeting in Beijing, China, where the expert panel was given the opportunity to raise questions and clarify their viewpoints.
Targeted literature review (TLR) and statement development
Questionnaires for the first rounds of the Challenges and Strategies Delphi panels were developed based on a review of published evidence and guidelines reporting on the following aspects of wound management: • Surgical techniques and materials used for wound closure at the capsular, subcutaneous and skin layers in TKA • Surgical, pharmacological and non-pharmacological bleeding management strategies in TKA
Literature searches were performed between July and August 2018 and carried out in MEDLINE and Embase (simultaneously via Ovid SP). The Cochrane Library database, the Chinese Knowledge Infrastructure (CNKI) database, and the KoreaMed database were also searched. Searches were date-limited to 2016 onwards. The list of search terms used are presented in the Supplementary Materials. In addition, the following sources of grey literature were searched: Asia-Pacific Arthroplastic Society (http://apasonline.org/useful_links.html) and the Asia-Pacific Knee Society (https://www.apoaonline.com/knee-section.php).
Information on patient factors, surgical techniques and surgical materials that can impact wound closure and bleeding management outcomes in TKA were extracted and developed into statements. Statements were grouped into one of the following three categories: (1) a goal of wound closure or bleeding management in TKA, (2) a challenge to achieving these goals or (3) a strategy to address these challenges. If a challenge statement did not gain consensus, the corresponding strategy statement(s) were not included in Delphi part 2: strategies.
The Steering Committee reviewed and finalized the statements to be included in the first round of questionnaires.
Delphi procedure
A flowchart illustrating the steps involved in the modified Delphi process is shown in Figure 1. The Delphi panel was conducted in two parts. In Delphi part 1: challenges, the expert panel was asked to respond to two sets of statements: • The first set of statements addressed goals in TKA; panelists indicated their agreement with each statement as a goal of wound management on a 5-point Likert scale: 1 = Strongly Disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly Agree. • The second set of statements addressed challenges in TKA; the expert panel was asked to indicate how important each challenge statement is to achieving wound management goals on a 5-point Likert scale: 1 = Not Important At All, 2 = Of Little Importance, 3 = Moderately Important, 4 = Important, 5 = Very Important. Delphi procedure. *After the expert panel discussion, the steering committee finalized the statements for Rounds 2.

In Delphi part 2: strategies, the expert panel indicated their agreement that each strategy statement is appropriate to address consensus challenges in wound management in TKA on a 5-point Likert scale: 1 = Strongly Disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly Agree.
Pre-determined consensus thresholds were used to ascertain which statements would progress through each round. Consensus was achieved if ≥70% of answers were a score of 4 or 5
After each round, statements that did not reach consensus were discussed amongst the steering committee and expert panel, and included once more in the next round, either as a repeated statement (without modification) or as a statement modified to better reflect the goal, challenge or strategy in TKA. If consensus was not reached for modified or repeated statements in the second round, they were not included in the final consensus framework.
Processing and synthesis of results
Responses were collated electronically through SurveyMonkey and downloaded in Microsoft Excel format for analysis. All statistical analyses to determine whether statements met consensus were performed in Microsoft Excel. Specific comments from the panel were also captured in Microsoft Excel; the relevance of each comment to the Delphi panel was later determined on a comment-by-comment basis.
Results
All ten surgeons who were invited to participate in the modified Delphi panel took part in Round 1 of Delphi part 1: challenges. There were nine surgeons who participated in all the subsequent rounds, including attending the face-to-face meeting.
Questionnaire results
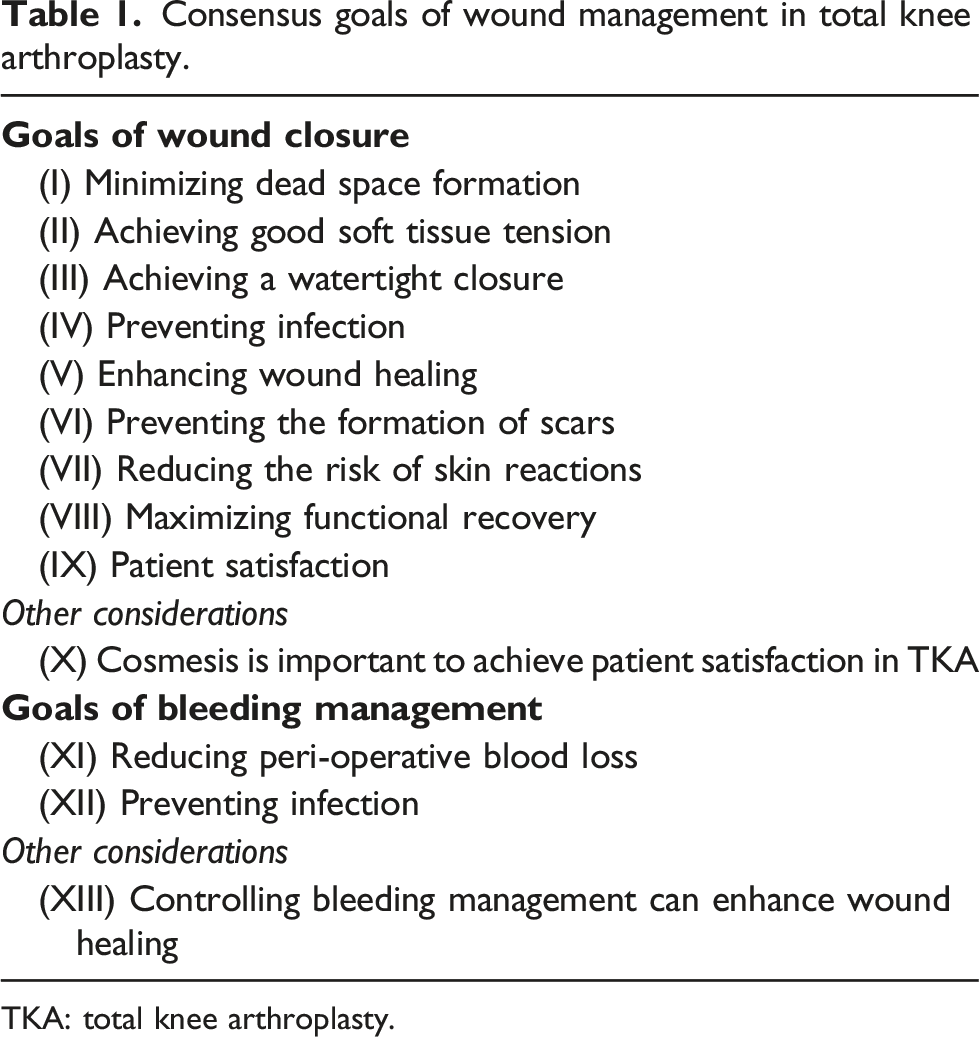
In Delphi part 1: challenges, seven proposed goals and 42 associated challenges were included in Round 1, while Round 1 of Delphi part 2: strategies, included 70 strategy statements (Figure 2). Overall, consensus was reached on 13 goals of wound closure and bleeding management, including: minimizing dead space formation, achieving good soft tissue tension and watertight closure, preventing infection or scarring, reducing blood loss and maximizing functional recovery (Table 1). Panelists agreed on 38 challenges associated with achieving these goals and 71 mitigation strategies (Figure 2). The challenges and strategies statements were grouped into subtopics to create a framework for consensus (Tables 2–9). Statements on patient factors, closure of the capsular and skin layers, bleeding management, wound dressings, drains and suction required repeat voting or modification to reach consensus, while statements for two subtopics: navigation, instrumentation, and technique and wound irrigation prior to closure, did not gain consensus and were not included in the consensus framework (Supplementary Materials). Modified challenges and strategies Delphi panel results flow diagram. Consensus goals of wound management in total knee arthroplasty. TKA: total knee arthroplasty. Patient factors: goals, challenges and strategies in total knee arthroplasty reaching consensus in the modified Delphi panel. TKA: total knee arthroplasty. Wound closure and bleeding management: goals, challenges and strategies in total knee arthroplasty reaching consensus in the modified Delphi panel. TKA: total knee arthroplasty. Capsular, subcutaneous and skin closure: goals, challenges and strategies in total knee arthroplasty reaching consensus in the modified Delphi panel. TKA: total knee arthroplasty. Wound closure materials and dressings: goals, challenges and strategies in total knee arthroplasty reaching consensus in the modified Delphi panel. TKA: total knee arthroplasty. Bleeding management: goals, challenges and strategies in total knee arthroplasty reaching consensus in the modified Delphi panel. TKA: total knee arthroplasty. Deep vein thrombosis prophylaxis: goals, challenges and strategies in total knee arthroplasty reaching consensus in the modified Delphi panel. DVT: deep vein thrombosis. Wound drain and suction: goals, challenges and strategies in total knee arthroplasty reaching consensus in the modified Delphi panel. Rehabilitation and follow-up: goals, challenges and strategies in total knee arthroplasty reaching consensus in the modified Delphi panel. TKA: total knee arthroplasty.







Patient factors
Panelists noted that various patient demographics (e.g. age and smoking status) can increase the risk of wound complications, while haematological abnormalities and concomitant medications (among other factors) can increase the risk of bleeding complications. Therefore, risk factors should be reviewed by specialists and optimized before TKA to determine the most appropriate approach to manage at-risk patients (Table 2).
General wound closure and bleeding management
More than half of the panelists (70%) agreed that an “important” or “very important” challenge in TKA is the anatomy and vascular supply of the knee joint (Supplementary Materials). This may pose unique challenges to achieving an optimal balance of wound tension and blood perfusion. Additionally, almost all panelists (90%) agreed that soft tissues at each layer of the knee joint (capsular, subcutaneous and skin) can pose different challenges to wound closure and infection prevention (Table 3).
Capsular, subcutaneous and skin closure
Knee position was identified as important for capsular closure, due to potential effects on strength and functional recovery of the joint. Furthermore, all panelists “agreed” or “strongly agreed” that the knee should be placed in a position to allow reapproximation of the arthrotomy during closure. A similar level of agreement was reached favoring flexion of the knee to facilitate anatomic closure and avoid excessive tension on repair. At the subcutaneous level, it is imperative that dead space is minimized as clinical results indicate this challenge is crucial to eradicate or prevent infection. Also, at the skin level, because the skin is typically thin and fragile (e.g. for TKA in elderly patients), it is important to consider skin tension, reapproximation and the avoidance of blistering while maintaining mechanical integrity (Table 4).
Wound closure materials and dressings
There was consensus that a skin closure system that consists of adhesives and self-adhering mesh could be considered for TKA. Ideally, wound closure systems should minimize the risk of secondary allergic reactions (Table 5). All panelists believed that the type of wound closure material, including sutures for capsular and subcutaneous closure, and sutures or staples for skin closure, was “important” or “very important” for each tissue layer (Table 4). To that end, potential shortcomings in the functionality of wound dressings were identified, such as inadequate provision of protection, absorbability, or leakage. Factors relating to wound management, such as frequent dressing changes and wound hygiene practices, also posed challenges that impact wound closure and healing. Importantly, nine strategy statements reached consensus that indicated potential ideal characteristics for dressings to facilitate optimal wound management (Table 5).
Bleeding management
Panelists indicated that bleeding management approaches should be individualized; considerations include patient-specific risk factors, the complexity of the surgery, and the expected volume of blood loss. Addressing the concerns on the safety of tranexamic acid in certain patient populations, the panelists agreed that topical hemostatic agents may be used as an adjunct to reduce bleeding risk. In addition, for patients contraindicated to pharmacological anti-fibrinolytic agents, biological tissue adhesives may be considered (Table 6).
Deep vein thrombosis (DVT) prophylaxis
Panelists agreed that there is a role for both mechanical and pharmacological methods of DVT prophylaxis and individualized according to the patient’s DVT risk profile. Challenges associated with mechanical methods include ease of implementation, while with pharmacological methods, the risk of thrombosis should be considered against the risk of excessive bleeding leading to infections, hematomas and wound drainage (Table 7).
Wound drain and suction
Two challenges were agreed amongst the panelists, namely that not using wound drains may lead to bruising and hematomas; and that prolonged wound drainage may be indicative of a poorly healing wound, requiring additional or adjunct intervention. Strategies that reached consensus to address these challenges included deciding on use of a wound drain on a case-by-case basis, based on individual patients’ bleeding risk profile. Addressing prolonged wound drainage, it was agreed that early detection of wound drainage can be managed through various conservative measures (e.g. limit range of motion, hold DVT prophylaxis, compression, ice, elevation, knee immobilization) and negative pressure wound therapy can be considered prophylactically (Table 8).
Rehabilitation and follow-up
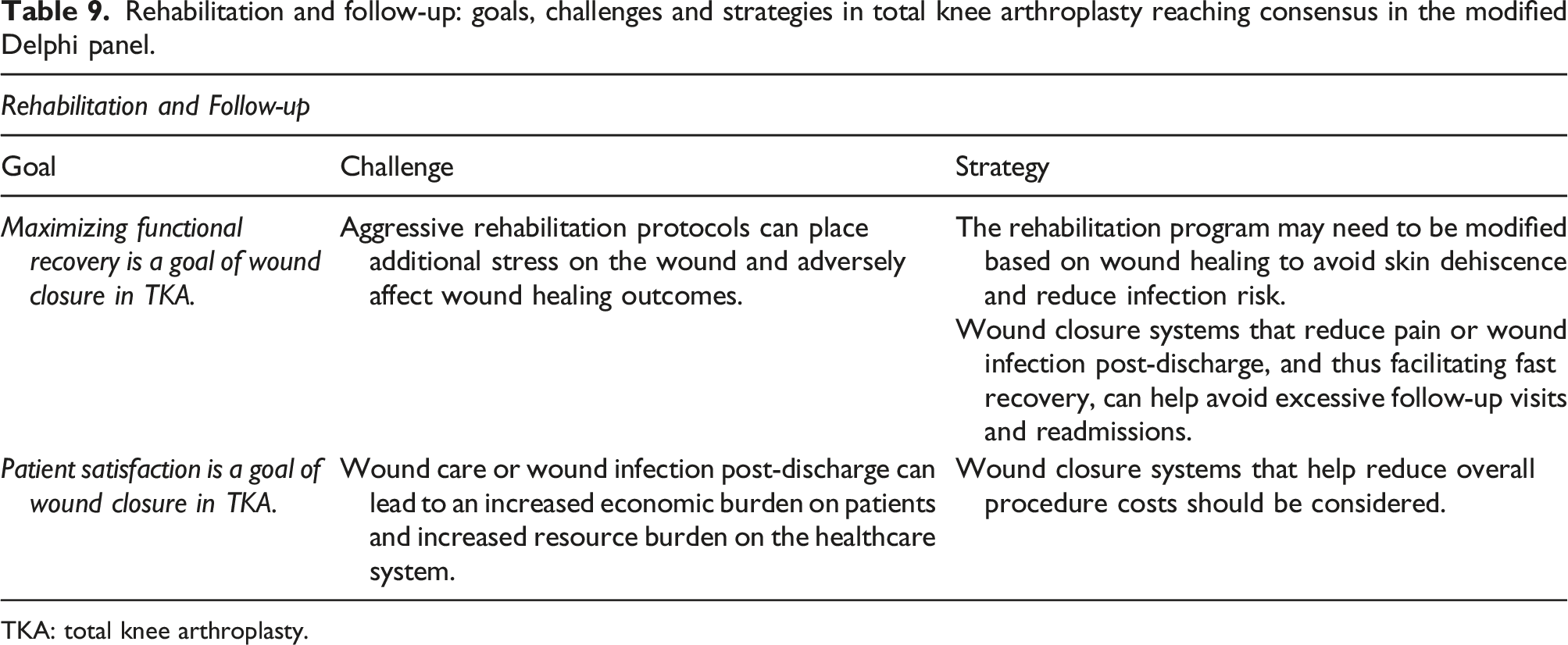
Consensus was reached that in order to maximize functional recovery the rehabilitation program may need to be modified based on wound healing to avoid skin dehiscence and reduce infection risk. Wound closure systems that reduce pain or wound infection post-discharge, and thus facilitating fast recovery, can help avoid excessive follow-up visits and readmissions (Table 9).
Discussion
Wound closure and bleeding management are two critical considerations in TKA that can significantly influence the success of the procedure; however, there is currently no available expert consensus on these complex aspects. Surgical outcomes and patient satisfaction in TKA could potentially be improved by developing consensus and continuing to raise awareness of these topics amongst surgeons.
Compared with the classical Delphi methodology, the modified Delphi methodology may be more appropriate to address complex and multifaceted clinical aspects. 19 Therefore, to reach consensus on wound closure and bleeding management, a modified Delphi methodology was used. This consisted of two Delphi panels conducted predominantly at a face-to-face meeting, which was important to allow panelists a platform for discussion and exchange of information, to resolve disagreements and allow for clarification. The modified method also facilitated the synthesis of goals, challenges and strategies statements that were not initially generated from the TLR.
Goals of wound closure and bleeding management in TKA
The number of wound closure and bleeding management goals in TKA expanded from 7 statements in the original list to 13 statements in the consensus list. The 6 additional statements contributed by advisors highlighted specific aspects of wound closure and tissue management that were not necessarily explicit in literature but were of sufficient importance to articulate from the perspective of orthopaedic surgeons. These included: minimizing dead space formation, achieving good soft tissue tension, and achieving a watertight closure.
Wound closure
Four key aspects of TKA emerged from the Delphi Panel as having an impact on whether wound closure goals may be met: patient factors, knee and tissue anatomy, wound closure materials and dressings, and risk of infection.
Patient factors
Consistent with published evidence, there was consensus that the risks associated with wound complications in TKA are increased by various patient demographics.20,21 These should be reviewed and specialists consulted prior to the procedure to enhance wound healing. 22
Another patient-factors aspect regarded the use of traditional medicines, which relate to the culture-specific knowledge, skills and practices involved in the maintenance of health and the prevention, diagnosis or treatment of illnesses. 23 Traditional medicines are commonly used in Asia-Pacific and, in some countries, are indeed viewed as appropriate and complementary to Western medicines; examples include acupuncture for treatment of pain, 24 and herbal medicine for wound healing 25 and treatment of soft tissue infections, although randomized controlled trials (RCTs) for the latter are lacking. 26 However, in our Delphi panel, no consensus was gained on whether traditional medicines impact on wound closure outcomes; this could reflect a lack of high-level evidence regarding the effects of traditional medicines on wound closure outcomes, a broad acceptance of their safety, and/or differences in orthopaedic experts’ attitudes towards traditional medicines, so that the consensus threshold could not be met. In addition, because there are regional differences in traditional medicines, this may also have impacted panelists’ attitudes and explain why consensus was not met on this topic.
Surgical techniques
Consensus from the Delphi panel was that achieving watertight closure and soft tissue tension, and minimizing dead space were key wound closure goals in TKA. At the capsular layer, the knee is subjected to high tensile forces and undergoes immense pressure during rehabilitation post-TKA; therefore, capsular closure needs to be watertight and robust. The importance of knee position to the achievement of capsular closure, in addition to flexion of the knee to facilitate anatomic closure and avoid excessive tension on repair, was emphasized by the panelists. The latter consideration is supported by a recent meta-analysis of 10 RCTs involving 962 knees, which reported less blood loss and better range-of-motion when the knee was positioned in flexion during TKA. 27 However, it should be noted that included studies had ‘moderate’ risk of bias as per the Cochrane Collaboration recommendations.
Wound closure materials and dressings
All panelists felt that the type of wound closure material, including sutures for capsular and subcutaneous closure, and sutures or staples for skin closure, was “important” or “very important” for each tissue layer. This was due to the risk of infection and other issues, which can in turn lead to greater healthcare costs and resource utilization, as well as affecting wound healing and cosmesis. The relative importance of cosmesis was found to be particularly controversial at the Delphi panel and highlighted region-specific differences. For some advisors, cosmesis and preventing the formation of scars are considered secondary to the goal of wound healing, maximizing functional recovery, or preventing wound complications. However, for patients in Japan, and especially in females, cosmesis may be as important as the other goals of wound care. In Malaysia, it was noted as important that the size and shape of the scar be minimized as far as possible. Another advisor also posited that a well-healing wound was important as it could aid cosmesis.
Deep wound closure
Panelists agreed that a variety of sutures and techniques could be used to reconstitute the watertight capsule; all panelists “agreed” or “strongly agreed” that barbed sutures are suitable for deep wound closure due to their ability to maintain continuous tension across the wound, to eliminate the need for knots, and due to their flexible and pliable mechanical properties.
One panelist was “neutral” about whether sutures that avoid the entrapment of bacteria in filaments should be used for deep wound closure, while all other panelists “agreed” or “strongly agreed”. Although an in vitro study has shown that bacterial colonization may occur beneath the barbs of barbed sutures, and recommends caution with their use in septic surgery, 28 other literature supports the use of barbed sutures for capsular closure in TKA in terms of maintaining maximal watertightness after knee-joint capsule closure, 29 by decreasing the number of sutures needed, and by reducing operating time compared to traditional interrupted sutures. 30 In other recent systematic reviews, barbed sutures were also found to reduce deep wound closure time compared with traditional sutures, with no difference in complication rates or outcomes.31,32
Skin closure
Challenges of wound closure at the skin layer are particularly related to the need for removing the wound closure material (in the case of staples or nylon sutures), which can require more clinic visits or cause pain. Based on qualitative evidence from two studies reporting on pain in orthopaedic surgery included in a systematic literature review and meta-analysis, the removal of staples is associated with more pain than sutures. However, other evidence indicates that staple use is associated with fewer follow-up visits. 33 Evidence for the effect of wound closure materials on length of stay, however, is variable, indicating no difference between closure materials in some cases, 34 but longer and shorter length of stay for staples in other reports. 35
Ideally, wound closure systems should minimize the risk of secondary allergic reactions. Such reactions include allergic contact dermatitis cases, which have been reported for 2-octyl cyanoacrylate,36,37 and may be exacerbated by factors such as heat, 38 and difficulties with removal. 39 However, these cases are rare and one study including 360 primary knee arthroplasty procedures conducted at a single institution supports the consensus from this Delphi panel; successful use of 2-octyl cyanoacrylate adhesive and polyester mesh in final skin closure of high-tension knee arthroplasty wounds was demonstrated, with a low rate of superficial wound complications and no cases of infections or dehiscence. 40
Wound dressings
Post-operative wound care is critical for wound healing and numerous strategy statements reached consensus that indicated potential ideal characteristics for dressings to facilitate optimal wound management (Tables 4 and 5). Evidence supporting this consensus indicates that hydrofibre dressings, which may help to maintain an environment conducive to wound healing, were preferable to standard and absorbent dressings in terms of infection risk, number of dressing changes and blistering events. 41 A second study similarly demonstrated a lower incidence of wound complications with the use of active dressings, such as film and hydrofibre dressings, rather than dressings that are gauze-based, although the rate of SSIs did not differ between dressing types. 42
Prevention of infection
Extensive evidence and guidelines are available discussing the risk of infection due to orthopaedic surgeries, including TKA. Almost all panelists (90%) agreed that the challenge to prevent infection, internally (i.e. from aspects of the TKA procedure) or externally (i.e. from aspects of wound breakdown and/or care) were “important” or “very important”. Intra-operative contamination was identified as a challenge to preventing infection and it was agreed by panelists at the Delphi panel that the risk may be mitigated through the choice of suture and use of wound irrigation. Factors relating to the wound, such as watertight skin closure and dressings that keep the wound sealed and prevent bacterial entry, were also deemed important to prevent infection.
Bleeding Management
Results from the Delphi panel indicate that bleeding management approaches should be individualized; considerations include patient-specific risk factors, the complexity of the surgery, and the expected volume of blood loss. Discussion from the panelists indicated that wound exudation and bleeding management could be linked. Further research may be needed to determine how bleeding management practices can control wound exudation.
Patient factors
In line with published evidence, panelists noted that patient factors can increase the risk of bleeding complications, and that bleeding risk factors should be reviewed and optimized before TKA. 43
Preventing bleeds
Surgical Approaches
Panelists highlighted the interactions between application of good wound management principles and its impact on bleeding management: for example, ensuring a watertight closure can minimize the risk of hematoma formation.
Transfusions and Other Strategies
In Delphi part 1: challenges, Round 1, all panelists felt that the concerns regarding risks associated with blood transfusion, such as disease transmission and hemolytic or allergic reactions, were “important” or “very important”. Similarly, all panelists “agreed” or “strongly agreed” that a ‘zero’ allogenic post-operative transfusion rate should be targeted. However, agreement and disagreement on the appropriate alternative to blood transfusions varied amongst panelists.
Panelists acknowledged the availability of tranexamic acid and tourniquets for bleeding management; however, there was no consensus on the precise risks of these strategies, such as whether these may lead to delayed bleeding or potential DVT. In the final consensus framework, only tranexamic acid was included (but not tourniquets), with panelists agreeing that its use, either intravenously, orally, or topically, is appropriate. This is broadly in line with the AAOS guidelines on surgical management of knee osteoarthritis, which stated the availability of “strong” evidence supporting treatment with tranexamic acid, but of only “moderate” evidence supporting the use of tourniquets. 18
Substantial discussions at the Delphi panel revolved around the role of topical hemostatic agents, such as fibrin glue and sealants, which are not discussed in existing guidelines. Consensus was reached when the statement on topical hemostatic agents was modified to describe its role as an “adjunct”, rather than as an “alternative”, to tourniquets and tranexamic acid. This is likely due to the availability of simpler, less expensive methods for hemostasis, which can be used in the first instance, while the use of topical hemostatic agents is reserved for specific patients. Several panelists highlighted their lack of experience with topic hemostatic agents.
Another topic of dissent was the role of wound drains in bleeding management. Panelists did not agree with the statement that wound drains can lead to complications (e.g. oozing, bruising and hematomas). However, panelists agreed that the converse is true (i.e. not using wound drains may lead to bruising and hematomas). The AAOS guidelines state that there is “strong” evidence to support not using a wound drain with TKA, as there is no difference in complications or outcomes. 18 The lack of consensus on the use of wound drains among Asia-Pacific surgeons may reflect differences in healthcare systems between regions, or region-related patient factors that may necessitate the use of drains.
Panelists were unable to agree on whether a thicker pre-patellar fat layer is a risk of infection and wound complications, although there have been some studies supporting this.44,45 Finally, panelists agreed that for patients contraindicated to anti-fibrinolytic agents, biological tissue adhesives may be considered. A systematic review explored the use of fibrin sealants for surgical incision closure 46 ; more recent systematic reviews have looked at the evidence for specific surgeries, including liver resection, 47 peripheral nerve repair 48 and non-emergency surgery. 49 Notably, in the most recent systematic review by Edwards (2016) designed to support a health technology assessment for the UK setting, a lack of data supporting the use of fibrin sealants in orthopaedic surgery was reported. 49
DVT prophylaxis
All challenges and strategies statements on DVT prophylaxis in TKA reached consensus in the first round of the Challenges and Strategies Delphi panels. Panelists agreed that there is a role for both mechanical and pharmacological methods of DVT prophylaxis. Both approaches are associated with benefits and risks, which highlights the need for an individualized regimen for TKA patients. Challenges associated with mechanical methods include ease of implementation, while with pharmacological methods, the risk of thrombosis should be considered against the risk of excessive bleeding leading to infections, hematomas and wound drainage. Religious and/or cultural beliefs may also necessitate an individualized DVT prophylaxis regimen, for example regarding pharmaceuticals of animal origin such as Clexane, 50 as may ethnic differences in outcomes between patients. 51
Limitations
In general, a limitation of using a modified Delphi methodology, such as in our study, is that the anonymity of the expert panel during the statement review and voting process may be lost. Pooled opinions from group interactions therefore risk being influenced by factors such as the viewpoints of more dominant individuals and pressure for conformity. 52 However, given the complex topic of wound closure and bleeding management in TKA, and the current lack of guidelines or consensus on these topics, the modification of the Delphi methodology to include a face-to-face meeting was important to facilitate synthesis, discussion and agreement of goals, challenges and strategies. Another limitation of our study was that, as a multi-national expert panel took part in this modified Delphi, translation between languages may have affected the interpretations of some of the questions.
Additionally, a key observation that arose from the extensive discussions between panelists was that surgical techniques employed by the participating surgeons, and surgical materials available in their respective countries, to achieve goals in wound closure and bleeding management in TKA differed on many levels (i.e. by regions, countries, institutions and individuals) – possibly due to differences in availability of, and/or demand on, healthcare resources. Hospitalization periods also vary depending on healthcare insurance systems, which differ between countries, and the environment of wound treatment – both during hospitalization and after discharge. As surgical experience and differences in exposure to specific techniques or products between regions may have influenced the responses of members of the expert panel this may in turn have affected the feasibility of gaining consensus amongst even this small group of surgeons. Gathering insight from a larger panel of surgeons would potentially increase the robustness of the consensus results. However, the panelists included in this study represent a wide range of nationalities and each bring their unique background and experiences, and thereby offers valuable perspective.
Conclusions
The extensive discussion observed at the Delphi panel reflects that there are differences in the levels of awareness of the role of wound closure and bleeding management on TKA outcomes, and highlights the need for further surgical education in this area. Overall, however, panelists agreed that a greater focus on wound management will play an important role in achieving optimal TKA outcomes, with patient factors, knee and tissue anatomy, wound closure materials and dressings, and risk of infection identified as key areas. Bleeding management approaches should be individualized, and should consider patient-specific risk factors, the complexity of the surgery, and the expected volume of blood loss. The resulting consensus framework of the goals of wound management in TKA, the challenges to these goals and strategies to address the challenges, will provide useful guidance for further surgical education on the importance of wound management to improve patient outcomes. The framework will also help to shape future guidelines for wound management in TKA. Future studies may investigate how orthopaedic surgeons interpret the consensus goals and challenges of wound closure and bleeding management in TKA, or apply the consensus strategies in a clinical practice.
Supplemental Material
Supplemental material - Goals, challenges and strategies for wound and bleeding management in total knee arthroplasty: A modified Delphi method
Supplemental material for Goals, challenges and strategies for wound and bleeding management in total knee arthroplasty: A modified Delphi method by Matthew Lyons, Ryan M. Nunley, Amran Ahmed Shokri, Tyson Doneley, Hyuk-Soo Han, Kengo Harato, Ayano Kuwasawa, Dae-Hee Lee, Xin Qi, Wenwei Qian, Siripong Ratanachai, Weijun Wang, Brian Po-Han Chen, and Walter Danker III in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
The authors thank the investigators and their teams who took part in this study. The authors acknowledge Akie Seno for input on a previous version of the manuscript and also acknowledge Ruth Le Fevre, Costello Medical Consulting Ltd and Schezn Lim, Costello Medical Singapore Pte Ltd for medical writing and editorial assistance based on the authors’ input and direction. The authors also acknowledge and authorize Claudia Tay Siu Wen, Costello Medical Singapore Pte Ltd for assistance with submitting this article on behalf of the authors. Support for third-party writing and submission assistance for this article was funded by Johnson & Johnson in accordance with Good Publication Practice (GPP3) guidelines (![]() ).
).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M Lyons: Received personal fees and non-financial support from Johnson and Johnson-Ethicon; grants from DePuy Synthes; personal fees from Corin and Zimmer Biomet. RM Nunley: Served as a paid consultant for Biocomposites, DePuy, Medtronic, Microport, Mirus, Smith & Nephew and ROM Tech; received stock options, royalties from Hyalex, Microport and ROM Tech; served as designer from Depuy, Smith & Nephew and Microport. T Doneley: Received personal fees from DePuy, stock options from Hip360 (Kico innovations). HS Han: Received grants from Korea Health Industry Development Institute and National Research Foundation of Korea. BPH Chen, W Danker III: Employee of Ethicon (Johnson and Johnson). AA Shokri, K Harato, A Kuwasawa, DH Lee, X Qi, W Qian, S Ratanachai, W Wang: Nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Johnson & Johnson.
Supplemental Material
Supplemental material for this article is available online.