
Abstract
Purpose
The purpose of this study is to compare the open Latarjet procedure versus the all-arthroscopic autologous tricortical iliac crest bone grafting (AICBG) technique for recurrent anterior-inferior glenohumeral instability with glenoid bone loss.
Methods
All open Latarjet and AICBG procedures for recurrent anterior-inferior shoulder instability with glenoid bone loss performed at two institutions between September 2015 and April 2019 were retrospectively analyzed. Inclusion criteria were a traumatic etiology, a glenoid surface deficiency >13.5%, and a minimum follow-up (FU) of 18 months. Primary outcomes included the subjective shoulder value, the Western Ontario Shoulder Instability (WOSI), Rowe scores including subdomains, and the four subdomains of the Constant score (pain, activities of daily living, internal rotation, external rotation). Secondary outcomes were subjective shoulder instability, EQ-5D-3 L, pain level on the VAS, level of overall satisfaction, operative time, return-to-work rate, and return-to-sports rate.
Results
Forty-three patients were available for final analysis (Latarjet: n = 21; AICBG: n = 22) at an average FU of 34.9 months (range, 22–66 months). Both techniques provided good outcomes and improved stability. The Rowe score, Rowe-range of motion, and CS-internal rotation (p = 0.008, p<0.001, p = 0.001) were slightly better in the AICBG group. Furthermore, the WOSI physical symptoms subdomain was significantly better (p = 0.04) in the AICBG group, while its total score did not reach statistical significance (p = 0.07). There was no statistically significant difference in the secondary outcomes besides operative time, which was significantly shorter in the Latarjet procedure group (p = 0.04). Overall complication rate was similar in both groups (Latarjet: 9.5% (n = 2), AICBG: 9.1% (n = 2)).
Conclusion
Open Latarjet and AICBG procedures provide comparable clinical outcomes except for significantly better Rowe score, Rowe-range of motion, WOSI physical symptoms subdomain, and internal rotation capacity in the AICBG group. However, these results should be carefully interpreted in the context of known minimal clinically important differences of these scores.
Introduction
In cases of recurrent anterior-inferior shoulder instability with glenoid bone loss, anatomic and non-anatomic bony stabilization procedures, including open and arthroscopic techniques, have been described. 1 In contrast to the non-anatomic Latarjet procedure, during the all-arthroscopic tricortical iliac crest bone grafting (AICBG) technique, the bone block can be positioned in an extra-articular and non-anatomic fashion or in an anatomic and intra-articular fashion.1–6
While both techniques provide reasonable outcomes, to date, no clear superiority of one technique over the other has been demonstrated. 5 However, some authors suggest that the benefits of using the AICBG procedure include smaller, arthroscopic incisions with less soft-tissue damage, repair accessibility, better outcomes for external rotation, and preservation of the integrity of the subscapularis (SSC) tendon.2,3 This may theoretically reduce the risk of SSC dysfunction, muscle atrophy, and fatty infiltration due to tendon repair failure.1–4
The purpose of this study is to compare the open Latarjet procedure versus the all-arthroscopic autologous tricortical iliac crest bone grafting (AICBG) technique for recurrent anterior-inferior glenohumeral instability with glenoid bone loss as to date, there is no study comparing these two procedures.
Materials and methods
This study has been authorized by the local ethical committee and was carried out in accordance with the Ethical standards of the 1964 Declaration of Helsinki as updated in 2004. All participants gave written consent.
All open Latarjet procedures and AICBG procedures for recurrent anterior-inferior shoulder instability with glenoid bone loss performed at two institutions between September 2015 and April 2019 were retrospectively analyzed.
Inclusion criteria were a traumatic etiology, a glenoid surface deficiency >13.5% measured per the method described by Barchilon on parasagittal magnetic resonance imaging, 7 and a minimum follow-up of 18 months.
Exclusion criteria included the presence of osteoarthritis define as more than grade 1 on the Samilson – Prieto scale, posterior instability, multidirectional instability, and any concomitant neurological lesion or disorder including epilepsy.
Between September 2015 and April 2019, 64 patients met the inclusion criteria (Latarjet: 28; AICBG: 36). Ten patients were excluded. Forty-three patients were available for final analysis (Latarjet: n = 21; AICBG: n = 22).
The two surgical techniques were performed by one senior surgeon with special focus on shoulder surgery in each of the two centers. The respective technique (open Latarjet and AICBG) is the standard of care for the abovementioned same inclusion criteria in each respective center.
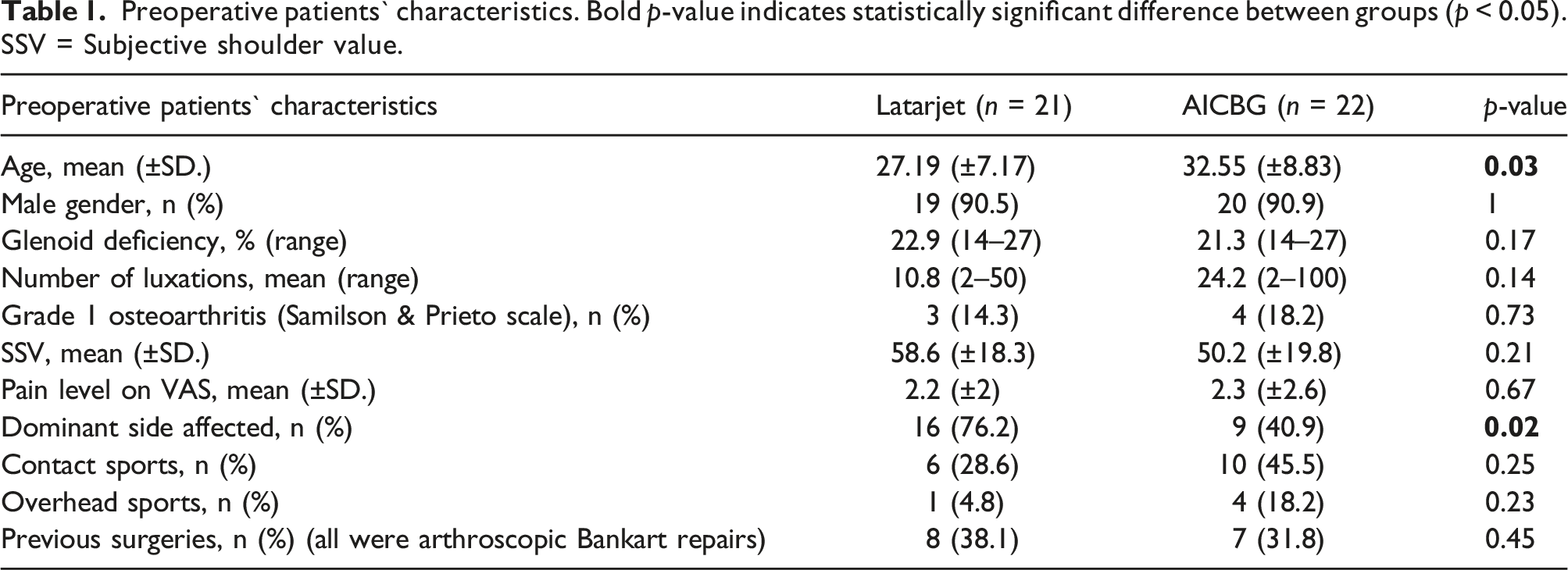
Preoperative patients` characteristics were determined and compared between the groups. These included age, sex, number of glenohumeral luxations, glenoid surface deficiency, grade of osteoarthritis according to the Samilson–Prieto scale, subjective shoulder value (SSV), pain level on the Visual Analogue Scale (VAS), laterality, proportion of of athletes engaged in overhead and contact sports, and type and number of previous surgeries.
Primary outcomes included the subjective shoulder value (SSV), the German version of Western Ontario Shoulder Instability Index (WOSI) and its subdomains, 8 the Rowe score and its subdomains, and four subdomains of the Constant score (CS) (pain, activities of daily living, internal rotation, external rotation).
Secondary outcomes were subjective shoulder instability (SSI), defined as a patient’s subjective assessment expressed as a percentage of an entirely unstable shoulder, which would score 100%, the 3-level version of the EuroQoL 5-dimensional instrument (EQ-5D-3 L), pain level on the VAS, level of overall satisfaction on a 4-point Likert scale, operative time, return-to-work rate, and return-to-sports rate. In addition, postoperative complications were compared.
Open latarjet technique
All Latarjet procedures were done in the beach chair position under general anesthesia. In addition, patients received an interscalene nerve catheter for postoperative pain management. The technique as described by Walch and Boileau was performed, utilizing a horizontal muscle split of the SSC between the superior two-thirds and inferior one-third in line with its fibers and suturing of the lateral capsular flap to the medial 1 cm of the coracoacromial ligament, which remains attached to the coracoid. 6 In deviation from the original description, the bone block was fixed with two 3.5 mm conventional small fragment cortex screws (Synthes, West Chester, Pennsylvania) instead of AO malleolar screws.
All-arthroscopic autologous tricortical iliac crest bone grafting (AICBG) technique
All AICBG procedures were also done in the beach chair position under general anesthesia. In addition, patients received an interscalene nerve catheter for postoperative pain management. In all patients, the tricortical bone graft was harvested first in the supine position from the ipsilateral anterior iliac crest before the arthroscopic procedure.
In seven consecutive patients, the bone block was positioned and fixated in the technique as described by Scheibel. 4 Due to the hypothetical concern that the temporary percutaneously placed K-wire fixation and subsequent overdrilling from the deep anterior-inferior portal might disturb the integrity of the SSC and harm the axillary nerve, this technique was abandoned at the end of 2017. Henceforth, the bone block was positioned and fixated as described by Taverna in the remaining 15 consecutive patients. 2
In both techniques, the capsulolabral complex was reattached with knotless anchors (BioComposite PushLock anchor, 2.9 mm x 15.5 mm, Arthrex, Naples, Florida) in a way that positioned the bone block extra-articularly.
Postoperative care
Both groups were postoperatively treated in a 15-degree abduction splint (medi SAS® 15, medi GmbH & Co. KG, Bayreuth, Germany) following a four-phase treatment protocol. Pendulum exercises and passive movements of shoulder, elbow, wrist, and finger joints were allowed in both groups after the first postoperative day. After the Latarjet procedure, external rotation was restricted for 6 weeks, while after the AICBG procedure, patients were allowed to rotate externally up to 20° in the first 4 weeks. Active movements up to full range of motion and two-handed weight-bearing up to 11 pounds were allowed in both groups from the sixth week.
In the Latarjet cohort, unrestricted full weight-bearing was allowed after the twelfth week, while weight-bearing in the AICBG cohort was more restrictively with a limit up to 22 pounds until the twelfth week, and unrestricted full weight-bearing only after 6 months.
Statistical analysis
Descriptive statistics were calculated. Chi-squared tests and Fisher's exact tests were used to examine the distribution of categorical variables. Interval and ordinal dependent variables were compared using the Mann–Whitney U test.
For subgroup analysis of more than two groups, one-way analysis of variance (ANOVA), and Bonferroni post hoc test were used to perform pairwise comparisons between group means.
The confidence level (CI) was set at 95% (p < 0.05). Data analysis was performed with SPSS 26.0 (IBM, Armonk, New York), and Microsoft Excel 2019 (Microsoft Corporation, Redmond, Washington).
Results
Preoperative patients` characteristics. Bold p-value indicates statistically significant difference between groups (p < 0.05). SSV = Subjective shoulder value.
Mean ± SD of patient outcomes of Latarjet and AICBG group. Bold p-value indicates statistically significant difference between groups (p < 0.05). SSV = Subjective shoulder value, CS = Constant Score.

In the analysis of our secondary outcomes, there was no statistically significant difference between groups except for operative time, which was significantly shorter in the Latarjet group (p = 0.04) (Table 2). Each of the 43 patients reported that they would undergo their corresponding operation again, if necessary.
In the Latarjet group, 18 patients (85.7%) were “very satisfied” and 3 patients (14.3%) were “satisfied”. In the AICBG group, 18 patients (81.8%) were “very satisfied”, and 4 patients (18.2%) were “satisfied”. No statistically significant difference in the rates of return-to-work or return-to-sports could be determined. All patients returned to full-time work and reported a full work capacity. In addition, Figure 1 shows the distribution of patient-reported level of sports performance at final FU compared to before surgery. Patient-reported level of sports performance at final FU compared to before surgery. Blue bars = Latarjet. Orange bars = AICBG
Complications
Overall complication rate was similar at 9.5% (n = 2) in the Latarjet group and 9.1% (n = 2) in the AICBG group. Each group had one major complication in the form of a recurrent luxation after more than 1 year postoperatively (Latarjet: 4.8%; AICBG: 4.5%). While the etiology was traumatic during snowboarding in the patient after AICBG, the recurrent luxation occurred atraumatically during sleeping in the patient after Latarjet procedure. Furthermore, one patient (4.5%) complained of persistent sensory disturbances around the scar of the donor site in the AICBG group, but without any functional impairment. One case of symptomatic screw back-out (4.8%) required implant removal after 1 year in the Latarjet group.
Subgroup analysis
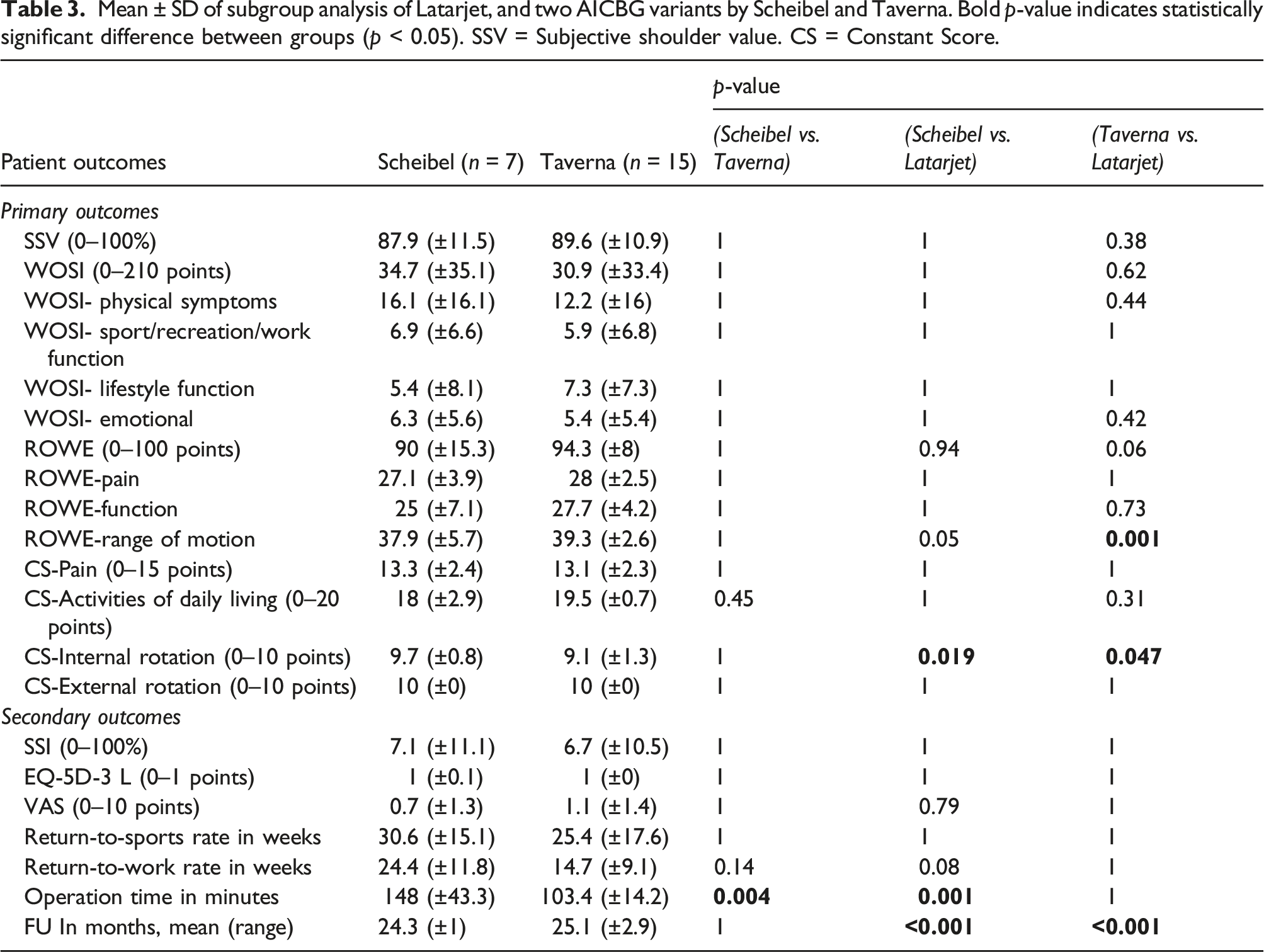
Mean ± SD of subgroup analysis of Latarjet, and two AICBG variants by Scheibel and Taverna. Bold p-value indicates statistically significant difference between groups (p < 0.05). SSV = Subjective shoulder value. CS = Constant Score.
Discussion
This is the first study comparing the open Latarjet procedure and AICBG procedure for recurrent anterior-inferior glenohumeral instability with glenoid bone loss. Both techniques provide comparable good outcomes with low complication rates. Except for modest statistically significant differences in the Rowe score and CS-internal rotation between the two techniques, no clinically relevant differences between the two techniques were noted. The proposed benefits of the arthroscopic procedure for better internal and external rotation and faster return to sports as a result of a minimally invasive approach could not be confirmed by this study. 2
This study demonstrated a statistically significant modest mean difference in the Rowe score and CS-internal rotation between Latarjet and AICBG procedures. However, this statistically significant difference must be carefully interpreted in the context of the minimal clinically important differences (MCIDs) of these scores. The MCID of the Rowe score has been reported to be at least 9.7 in patients who underwent arthroscopic stabilization surgery using an anchor-based method. 9 Therefore, the mean difference of 8.2 points in the Rowe score between groups in this study may not be clinically relevant.
To the best knowledge of the authors, no MCID exists for CS-internal rotation in the literature. 10 However, internal rotation is known to be compromised after the open Latarjet procedure. In a prospective, randomized trial, Moroder has shown internal rotation being significantly worse by 2–3 vertebral levels on average after the open Latarjet procedure compared with an open ICBG (J-bone graft) procedure. 5 A reason for these significant differences in internal rotation capacity might be the permanent split of the subscapularis by the conjoined tendon with potential structural damage. 5
Although the Latarjet procedure has the advantage of not requiring separate donor-site morbidity, adverse events such as symptomatic screw back-out requiring revision surgery have been described in the literature,5,11,12 and present a motivation for the investigation of alternative fixation techniques using resorbable material or suture buttons. 5 In this study, the complication rate of symptomatic screw back-out was low (n = 1, 4.8%), but slightly higher than described by Moroder (n = 1, 3.3%). 5 Similarly, donor site–related adverse events in the AICBG procedure are known to be common, mostly involving sensory disturbances around the scar following bone graft harvesting from the iliac crest, and present a motivation for investigation on alternative techniques using allografts or other donor sites. Surprisingly, the rate of this complication in this study was low (4.5%) compared with reported results by Moroder (n = 8, 26.7%), but nevertheless in the range of reported prevalences in reviews of larger datasets.5,13
This study has some limitations. This study was retrospective in design, and our sample size was limited, especially in subgroups comparisons of technical variants. The mean follow-up period was short and significantly different between groups. In addition, the outcomes of this study are mainly patient-reported. Besides SSV, no primary outcomes were analyzed preoperatively. We were not able to assess range of motion, strength, or imaging evaluation such as x-ray, CT, or MRI follow-up in this study. This is why, no conclusions can be drawn concerning incidence of osteoarthritis, graft resorption or union rate.
The two surgical techniques were performed by one senior surgeon with special focus on shoulder surgery in each of the two centers. This may affect the external validity of the reported results. Furthermore, the selected cut off value of 13.5% glenoid bone loss is not commonly accepted. A defect size of 13.5% has been referred as “subcritical bone loss” by some authors.14,15 These suggested significantly worse outcomes in case of defects greater than 13.5% in highly active patients when only soft tissue stabilization is performed.14,15 For these reasons, this cut off value was used by the authors.
In addition, the similar complication rates have to be considered carefully due to the potential heterogeneity of the subjects as for example prevalence of preoperative bipolar lesions has not been evaluated.
Taverna described specific indications for the AICBG procedure, and a decision algorithm with regard to the question of when the Latarjet procedure and AICBG procedure should be performed. These criteria considered the amount of glenoid bone loss, ISIS score, young age, number of dislocation episodes, timing of initial instability, and capsular tissue consistency. 2 These criteria are not taken into account in the two study institutions of this trial for choosing the indication or procedure. Preoperative patients’ characteristics in this study included patients of older age and the preoperative number of dislocations ranged up to 100 events. Nevertheless, both techniques provided comparable reasonable results and similarly low complication rates without any clinically relevant differences in this study. Therefore, our results call into question previously described criteria, and surgeons may opt to choose surgical technique based on their preference, experience, and technical familiarity.
Conclusion
Open Latarjet and AICBG procedures provide comparable good clinical outcomes except for significantly better Rowe score, Rowe-range of motion, WOSI physical symptoms subdomain, and internal rotation capacity in the AICBG group. However, these results should be carefully interpreted in the context of known minimal clinically important differences of these scores.
Footnotes
Acknowledgements
The authors would like to thank all the participating patients. We acknowledge support by the German Research Foundation (DFG) and the Open Access Publication Fund of Hannover Medical School (MHH).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.