
Abstract
Background
Treatment of bone lesions involved with the articular cartilage at the talus is challenging. We report the management of talus lesions, particularly tumors and avascular necrosis (AVN), at the articular surface through treatment with cement augmentation and autologous bone graft.
Methods
Eight benign bone tumors and three cases of AVN were reviewed retrospectively at a mean follow-up of 56 months (range, 12–162). The mean age of all patients was 36.1 years old (range, 15–73) when assessed between February 2005 and November 2021. Curettage of tumorous and necrotic lesions resulted in significant bone defects filled with bone cement augmentation. Cartilage defects of the talar dome were supported with autologous cancellous bone graft. Tolerable weight-bearing ambulation was permitted immediately after surgery. Radiological and functional evaluations were recorded.
Results
We observed an increase in the average The American Orthopaedic Foot and Ankle Score (AOFAS) (p = .003) and a decrease in the average Visual Analogue Scale pain score (p = .003). There was no statistically significant decrease in ROM before or after surgery (p = .114). Additionally, no talus collapse of the ankle joint occurred. Talar dome status did not aggravate before or after surgery, except for one patient. Despite no radiographic osteoarthritis exacerbation before or after surgery in six patients, five patients had osteoarthritic change.
Conclusion
Cement implantation and autologous bone graft performed simultaneously for benign bone tumors with joint cartilage damage and AVN are technically simple, have good outcomes, and may be a suitable alternative to standard treatments.
Introduction
The talus is anatomically complex, surrounded by the tibia, fibula, calcaneus, and navicular, and therefore requires a complex operative approach. Additionally, its lack of blood supply with a wide cartilaginous portion creates difficulty in treating abnormal bone lesions located at the talus, despite the variety of options available. 1
Bone tumor and avascular necrosis (AVN) are separate disease entities sharing the similarity of abnormal bone lesion occurrence. These diseases are also challenging when arising at the talus, particularly when articular cartilage is involved, which can lead to functional disability.
Benign bone tumors without cartilage involvement can be treated by curettage and filling with bone graft or bone cement; however, cartilage invasion is more challenging.2,3 AVN invades cancellous and subchondral bone, which often causes collapse and cartilage damage, requiring bone graft and arthrodesis.4-6 Eventually, functional impairment can occur.
This study aimed to provide insights into an effective operative treatment method for talar bone lesions, particularly tumors and AVN. We report the management of talus lesions involving the articular surface with bone graft and cement augmentation.
Materials and methods
Patient demographics
11 patients with benign bone tumors or AVN at the talus who underwent curettage and cement augmentation between February 2005 and November 2021 were included in the study. Patients with osteomyelitis, malignant bone tumor, and rheumatoid arthritis at the talus were excluded.
Five patients were male and six were female. Eight had presented with benign bone tumor of the talus, four had a chondroblastoma, two had a giant cell tumor, one had a simple bone cyst, and one had chondromyxoid fibroma. The remaining three patients had AVN of the talus.
Demographic features.

The protocol for this study was reviewed and approved by the Institutional Review Board (IRB No. 20211454). The need for informed consent was waived because of the retrospective nature of this study. A comprehensive agreement for academic use of clinical information such as type of treatments, treatment progress, or any other data acquired during their treatments was obtained from the patients at the time of their hospitalization or outpatient visit. No identifiable participant information is included in the manuscript.
Operative treatment
All procedures were performed with the patient supine with an ipsilateral thigh tourniquet.
Patients with bone tumors underwent an osteotomy in the medial or lateral malleolus according to the tumor’s location. However, AVN was operated on with an anterior approach without osteotomy.
A window was created in the body of the talus. All visible tumor was removed by meticulous curettage by confirming with a C-arm image, and inviable bone was removed by curettage until the healthy bone was exposed in AVN, resulting in a large volume of bone loss. Autologous bone grafts were applied in the subchondral area, and all remaining defects were filled with cement (Figure 1). If the cartilage was intact, an autologous bone graft was not required. Given the risk of cement leakage, particularly in patients with AVN owing to the lack of enclosing cortical bone, meticulous attention was required by the operating surgeon. Chondroblastoma at the talus (Left), It was removed and bone cementing was performed (Right).
After confirming that the talus was sufficiently filled, the window was closed, and the osteotomy site was fixed using a screw and plate.
Post-operative care
Patients were allowed to start ankle motion immediately and walk with tolerable weight-bearing in a short leg splint or cast. A cast or splint was worn for 4 weeks, after which patients returned to regular footwear.
Functional evaluation
The American Orthopedic Foot & Ankle Society (AOFAS) score, Visual Analogue Scale (VAS) pain score, and ankle range of motion (ROM, sum of ankle extension, and flexion) were measured before surgery and at the final follow-up.
Radiographic evaluation
Radiography such as X-ray, CT, or MRI was used to record the collapse of the talus, the condition of the talus cartilage before and after surgery, and changes in osteoarthritis (OA) (using the Kellgren and Lawrence grading system), cement leakage, and the occurrence of osteolysis around the cement and bone (cement gap). The volume of the tumor and recurrence were recorded.
The tumor height (a, the largest length in the coronal or sagittal plane), width (b, the largest medial to lateral length in the axial plane), and length (c, the largest anterior to posterior length in the axial plane) were measured under the assumption of an ellipsoid. The volume of the tumor (V) was calculated as follows:
Statistical analyses
Statistical analyses were performed using SPSS software. VAS pain score, AOFAS score, and ROM before surgery and at final follow-up were compared through the Wilcoxon sign test, and p-values of <0.05 were considered statistically significant.
Results
Functional, radiologic outcomes & cement related complications.
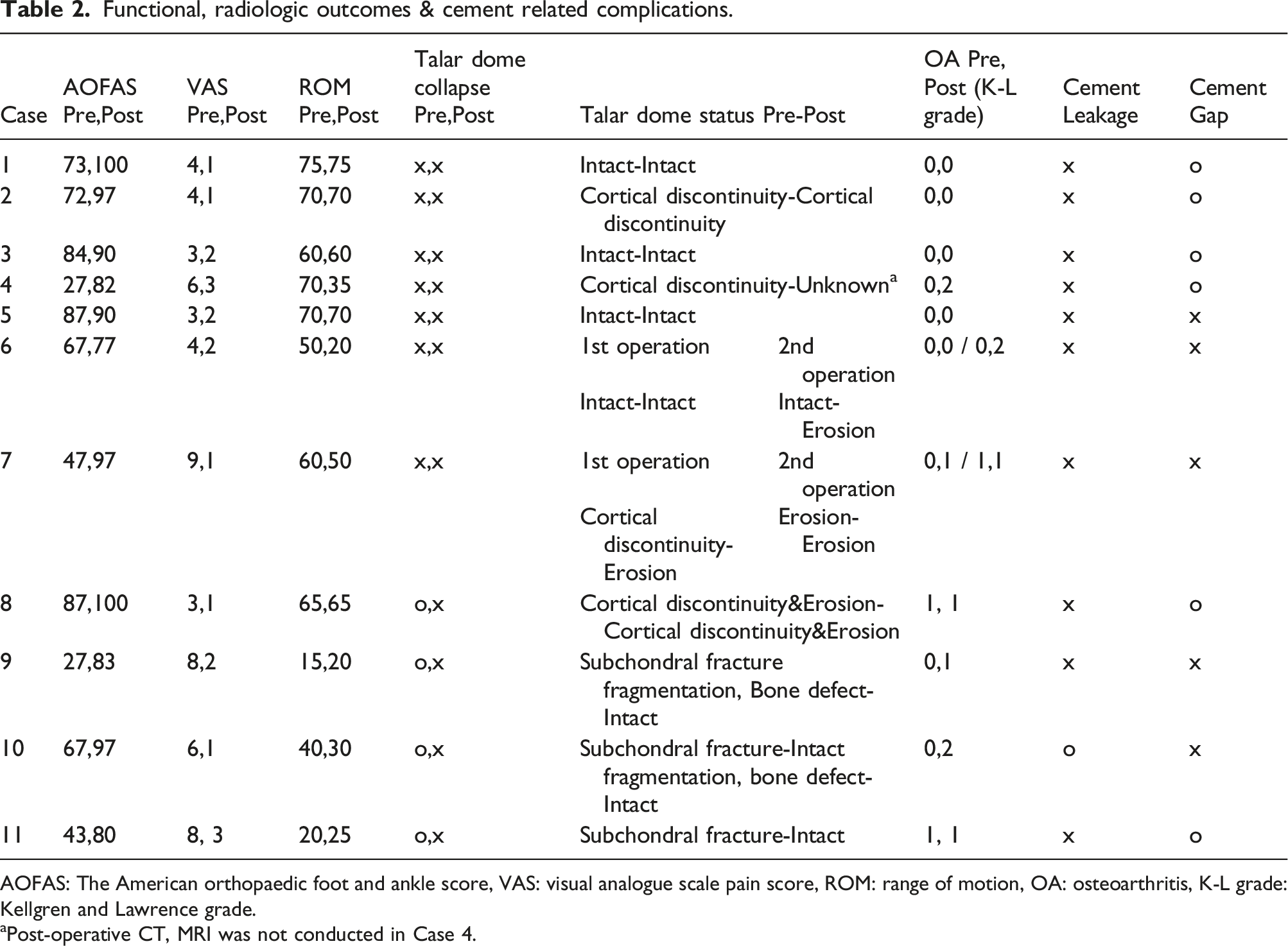
AOFAS: The American orthopaedic foot and ankle score, VAS: visual analogue scale pain score, ROM: range of motion, OA: osteoarthritis, K-L grade: Kellgren and Lawrence grade.
aPost-operative CT, MRI was not conducted in Case 4.
Additionally, no talus collapse of the ankle joint occurred. Conversely, four patients (Cases 8, 9, 10, 11) with talus collapse recovered to near normal height after cement insertion. Talus cartilage condition did not diminish before or after surgery except in one patient (Case 6). Six patients (Cases 1, 2, 3, 5, 8, 11) had no radiographic OA exacerbation before or after surgery, but five patients (Cases 4, 6, 7, 9, 10) had osteoarthritic change within Kellgren and Lawrence grade 1 or 2 (Table 2 and Figure 2). Chondroblastoma at talus was seen in pre-operative X-ray (Left). Talus collapse, osteoarthritic change, or cement leakage was not observed up to 58 months follow-up (Right).
The average size of the bone tumors was 6.99 cm³ across all patients.
One patient (Case 6) who initially had three different lesions underwent surgery three times. The first was performed at another hospital, during which the anterior and superior tumors were missed (Figure 3). Anterior talofibular ligament was cut off for visualization without osteotomy at the second operation, and the superior tumor was missed. Finally, an osteotomy was performed, and the superior tumor was removed. Therefore, we regard this as a case in which three tumors were missed rather than recurrence Missed anterior and superior lesions observed on MRI taken before the second surgery (White arrows).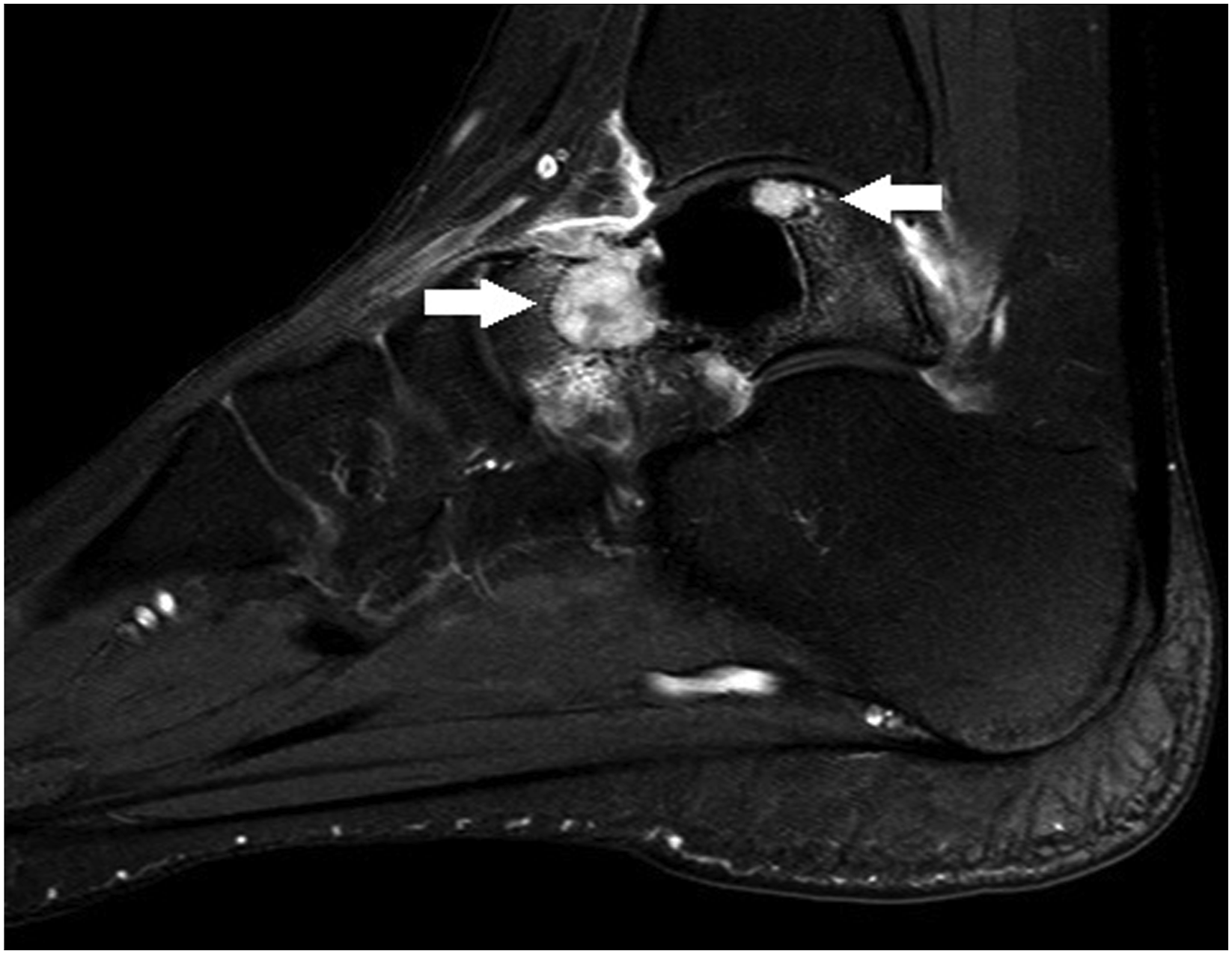
Recurrence occurred in one patient with a bone tumor (Case 7); however, undergoing the same operative procedure prevented further recurrence (Table 2).
Cement-related complications occurred. For example, cement leakage was observed in one patient with avascular bone necrosis (Case 10), and a gap between the cement and bone (Cases 1, 2, 3, 4, 8, 11) occurred in six patients (Figure 4, Table 2). Talar collapse was observed in pre-operative X-ray of avascular necrosis patient (Left). After performing bone cement augmentation, talar dome collapse was recovered to near normal height (Middle). Posterior cement leakage occurred during follow-up (Right).
Discussion
Many studies have confirmed good results from autologous bone grafts in small bone tumors,9–11 and bone cement if the lesion is large. 2 Our study differed from previous studies in that we performed cement augmentation with autologous bone graft when subchondral defects occurred. We used bone cement and autologous bone graft for the central and subchondral portions of the talus, respectively. We intended to replace the function of the rigid subchondral bone using a bone graft to act as the “wall” and cement as a “buttress”. This technique proved particularly useful when subchondral collapse or cartilage defects occurred in AVN and bone tumors.
If the tumor and AVN are small, performing a bone graft only after curettage can be considered. However, the average tumor size was 6.99 cm³ in this study. Filling a this large defect with allograft bone only can potentially lead to bone resorption and infection.12–14 However, obtaining an appropriate quantity of bone tissue from the patient can cause pain and comorbidities, and in some cases is simply not possible.15,16 However, bone cement does not appear to cause harm to the patient and can be supported sufficiently with the amount needed.
We obtained satisfactory outcomes with bone cement and bone graft. The height of the talus body was restored to close to normal ranges, indicating minor bone resorption. The osteoarthritic change in five patients was grade 1 or 2. Considering that OA change was not severe, subchondral collapse and cartilage defects were restored and solved to some extent with this technique. Even patients in whom cement gap or post-operative OA findings were observed by radiographic imaging showed no symptoms (pain, swelling, gait disorder) or impact on daily life, thus were observed without any treatment.
If worsening in osteoarthritis causes the patient to require ankle fusion, the operation does not differ from general ankle fusion. Though the defect will be large, it can be filled up with an autograft or allograft, or bone substitute in the same way. Also, the size of the defect will increase in the revision ankle fusion, but the differences will not be significant. At last, fixation with an implant will be performed.
Although talar AVN has several treatment options, the most realistic alternative is arthrodesis with bone graft. 5 Even if arthrodesis is performed, achieving bone union is challenging, and functional disorders remain inevitably.17,18 Unlike joint-sacrificing surgery, using a simple technique to ensure joint preservation is expected to yield better functional treatment results.
Unlike tumor cases, AVN lesions have subchondral fractures preventing the containment of bone cement in the surrounding cortex. To prevent cement leakage, the ankle joint was distracted directly to face the joint surface, confirmed with the naked eye and C-arm X-ray. Although leaked bone cement was removed to prevent joint irritation, cement leakage occurred (Case 10). There was some limitation to the ankle joint ROM, but it was not significant enough to cause pain or walking difficulties.
Treating talus lesions with bone cement is quick, easy, and simple. Functional advantages include patients walking and starting ankle motion immediately after surgery. Fortunately, there were no cases of cement breakage, loosening, foreign body reaction, or talar dome collapse during the 16-year follow-up in our study. Although the technique is not permanent, as demonstrated in OA progression or osteolysis cases, which may require additional surgery such as ankle fusion, the effects are long-term with no to minimal side effects. Additionally, bone cement insertion acts as a joint-preserving surgery, unlike ankle fusion, which typically sacrifices the ankle.
Our study was underpowered owing to the small sample size. We aimed to address the management of talar body bone lesions specifically; therefore, we could only include 11 cases, eight of which were bone tumors and three were AVN, given their rarity.
Although bone tumors and AVN are different disease entities, we have discussed them collectively, given the application of the same operative technique. Bone tumors typically occur in young patients with intact subchondral bone 19 ; thus, these patients rarely experience talar dome collapse. Therefore, bone cement and autologous bone grafts are well confined and could be used over a long period. However, AVN usually occurs in older patients who often present with talar dome collapse. Outcomes are usually satisfactory in patients with a low physical demand after restoring the talar dome collapse using filling cement with autologous bone graft.
However, it should not be misinterpreted that this surgical technique can be applied to all bone tumors and lesions. The technique was applied on talar body bone lesions, which are not malignant diseases, and do not invade the subtalar joint. In the case of bone tumors, treating a large or aggressive tumor by only curettage is insufficient; resection or adjuvant treatment would be required in these cases. In the case of AVN, treating a large whole talus lesion including the body, neck, and head with only curettage will be insufficient; joint arthrodesis with sufficient bone graft is needed in these cases. The shorter follow-up term also prevented the evaluation of long-term cement-related complications. A follow-up study of 20–30 years would be required to assess the possibility of long-term adverse events. However, the long-term operative use of total knee replacement arthroplasty suggests that significant cement-related complications are unlikely to occur.
Conclusion
Cement implantation with autologous bone graft for bone lesions of the talus (benign bone tumors with joint cartilage damage and AVN) is simple with good outcomes and may be a satisfactory alternative to various more invasive surgeries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The protocol of this study was reviewed and approved by the Asan Medical Center Institutional Review Board (IRB No. 20211454).