
Abstract
Purpose
The purpose of this study was to evaluate sequential patellar height changes as well as the factors leading to these changes after medial open-wedge high tibial osteotomy (MOWHTO).
Methods
The study cohort constituted 37 knees from 36 patients who underwent MOWHTO for varus knee. The Caton–Deschamps index (CDI) for patellar height was measured preoperatively and at 2 weeks and 3, 6, and 12 months postoperatively. The factors related to sequential changes in patellar height were evaluated.
Results
Significant differences were observed between preoperative CDI and postoperative CDI at all time points (p < .05). Two-week postoperative CDI and postoperative CDI at 3,6,12-months was also significantly different (p < .05). The only significant factor for the change in patellar height between preoperative CDI and postoperative CDI at 2-weeks and 12-months was the change in the Δ medial proximal tibial angle (ΔMPTA) (postoperative MPTA–preoperative MPTA). We could not identify the factor that affected the change in patellar height change from 2-weeks postoperatively.
Conclusion
The change in patellar height continued sequentially until at least 3 months postoperatively. ΔMPTA was associated with the change in patellar height at 2 weeks postoperatively compared with preoperatively; however, no factors associated with the change in patellar height from 2 weeks postoperatively to 3, 6, and 12-months postoperatively were identified.
Keywords
Introduction
Medial open-wedge high tibial osteotomy (MOWHTO) is a widely performed surgical procedure for patients with varus malalignment and medial compartment knee osteoarthritis (OA). Good long-term clinical results have been reported (10-years survival rate of 90%). 1 The reported complications of MOWHTO include patella baja, hinge fracture, non-union, infection, and hardware-related irritation.2–4 Many studies have reported patella baja after MOWHTO as a major complication of the procedure (incidence rate: 80%–100%).5,6 Patellar height is reduced during MOWHTO because of distalization of the tuberosity. 7 In general, the change in patellar height had finished at direct postoperatively. However, El-Azab et al. reported a significant decrease in patellar height at direct postoperatively compared with before surgery, and the number of patellar infera cases increased before removal of the hardware compared with direct postoperatively. 8 Moreover, some scholars have reported that patellar tendon contracture may reduce patellar height after OWHTO.9–11 Therefore, in this study, we measured patellar height sequentially after MOWHTO to determine when patellar height change occur. We hypothesized that the patellar height changes sequentially after MOWHTO. The purpose of this study was to evaluate the sequential changes in patellar height and the factors that contribute to these changes after MOWHTO.
Materials and methods
Patients
This study was approved by the Institutional Review Board of Fukuoka University Hospital (U21-01-014), and informed consent was obtained from all patients. This study was a retrospective, nonrandomized, and sequential study. The study cohort constituted 37 knees from 36 consecutive patients (male/female, n = 13/24) who underwent MOWHTO. All surgical procedures were performed by one senior surgeon to treat medial OA of the knee at our institution from April 2017 to August 2020. The mean age of the patients was 64.3 ± 6.9 years (range, 52–77 years), and the mean body mass index (BMI) was 26.3 ± 3.8 kg/m2 (range, 19.6–32.7 kg/m2). 14 patients had Kellgren–Lawrence grade II disease, 18 patients had grade III, and five patients had grade IV. Clinical function was evaluated using the Knee Injury and Osteoarthritis Outcome Score (KOOS).
Surgical technique and postoperative rehabilitation
A longitudinal skin incision was made over the pes anserinus insertion at the anteromedial aspect of the tibia. The medial proximal tibia was exposed by releasing the pes anserinus and the medial collateral ligament. First, osteotomy was performed at the medial cortical margin of the proximal tibia, along the osteotomy guide, and stopped approximately 5 mm from the lateral cortical margin, targeting the proximal tibiofibular joint. Second, osteotomy was performed in the frontal plane while protecting the patellar tendon and maintaining a tibial tubercle thickness of approximately 10 mm. The osteotomy site was opened using an opener until the preoperatively planned medial proximal tibial angle (MPTA) was reached. β-Tricalcium phosphate and two β-tricalcium phosphate wedges were inserted into the osteotomy gap. The medial osteotomy site was fixed using a locking compression plate after the pes anserinus was repaired.
Isometric quadriceps exercises, active ankle exercises, straight leg raises, and continuous passive motion with no limitation were started on postoperative day 3. Patients were allowed to begin half partial weight-bearing exercises 2 weeks after surgery and were allowed to begin full weight-bearing exercises 4 weeks after surgery. Patients with microfractures were allowed to begin half partial weight-bearing exercises 3 weeks postoperatively and were allowed to begin full weight-bearing exercises 5 weeks postoperatively.
Radiographic evaluation
The % mechanical axis (%MA) and the MPTA were measured using standing anteroposterior full-length radiographs of the lower limb (Figure 1). The MA represents the point at which the Mikulicz line (the line connecting the center of the femoral head to the center of the talus) passes from the most medial side of the tibial plateau. The %MA is calculated as the ratio of the horizontal distance from the medial edge of the tibial plateau to the intersection of the MA. The MPTA is defined as the medial angle between the tibial anatomic axis and the joint line of the proximal tibia. The posterior tibial slope (PTS) was measured on the lateral diagram of the knee according to the method of Brazier et al.
12
(Figure 2). The Caton-Deschamps index (CDI) was used to measure the patellar height preoperatively (preCDI) and at 2 weeks (post2WCDI) and 3, 6, and 12 months postoperatively (post3MCDI, post6MCDI, and post12MCDI, respectively)
13
(Figure 3). Many reports have shown that the CDI is a reliable and reproducible method, and it is also a more direct method to measure patellar height compared with the Insall-Salvati index (ISI), which measures the patellar tendon length.5,14 Furthermore, the CDI is poorly influenced by the quadriceps muscle.
15
The ISI has demonstrated poor reproducibility and repeatability because of the difficulty in identify the location of the patellar tendon and the anterior tibial tubercle on postoperative X-ray.5,16 The Blackburne-Peel index (BPI) may not be an accurate method to assess patellar height after high tibial osteotomy (HTO), because BPI depends on the change in the posterior tibial slope, which frequently occurs in HTO.
17
Therefore, we believe that the CDI is the most suitable method to assess patellar height after HTO. Radiographic measurements for evaluating coronal alignment on standing full-length anterior-posterior radiographs. (a) Mechanical axis (MA); (b) %MA; %MA (a/b) is calculated as the ratio of the horizontal distance from the medial edge of the tibial plateau to the intersection of the MA (a) and the proximal tibial plateau line to the entire length of the proximal tibial plateau line (b). (c) Mechanical Medial proximal tibial angle (MPTA). Lateral radiograph of the knee. The tibial slope was measured according to Brazier et al.‘s method. The inclination angle between the tangent to the medial tibial plateau and the line perpendicular to the tangent of the posterior tibial cortex was measured. Lateral radiograph of the knee. Caton–deschamps index = a/b.


Statistical analysis
Paired t-tests were used to evaluate pre- and postoperative differences in alignment parameters and KOOS. The CDI was measured to evaluate sequential changes in patellar height after MOWHTO. The repeated-measures analysis of variance (ANOVA) with Tukey’s post-hoc test was used to compare the CDI at different time points. Significant differences identified with Tukey’s test were defined as ΔCDI. Multiple regression was used to predict changes in ΔCDI based on preoperative % MA and PTS, ΔMPTA (postoperative MPTA – preoperative MPTA), age, sex, BMI, and OA grade.
Correlations between ΔKOOS (post12MKOOS − preKOOS) and ΔCDI (preCDI – post12MCDI) were assessed using Spearman’s rank correlation coefficient analysis to determine whether patellar baja negatively impacted the clinical outcome.
A p value of <0.05 was considered statically significant. The post-hoc analyses showed that a sample size of 24 achieved a power of 80% and a significance level of 5%, which verified the adequacy of the present sample size. All statistical analyses were performed using SPSS software (version 23.0, IBM Corp. Armonk, NY, USA).
Results
The patients’ demographic characteristics (n = 30).
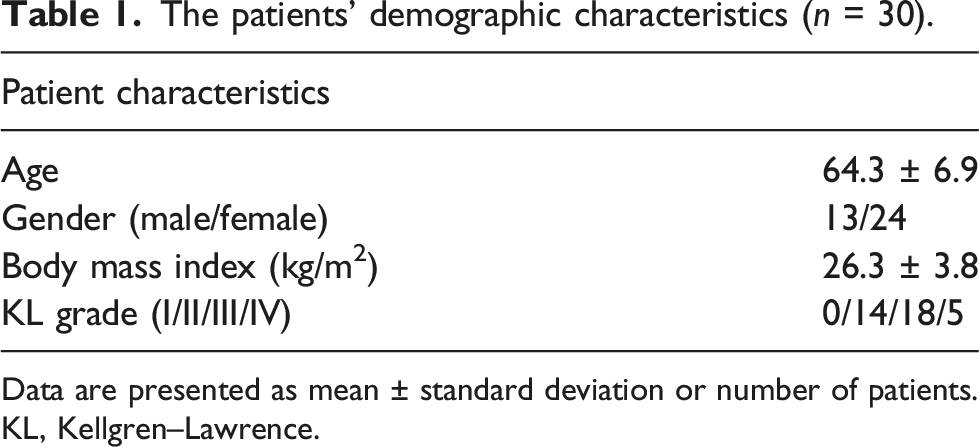
Data are presented as mean ± standard deviation or number of patients. KL, Kellgren–Lawrence.
Preoperative and postoperative radiographic measurements.
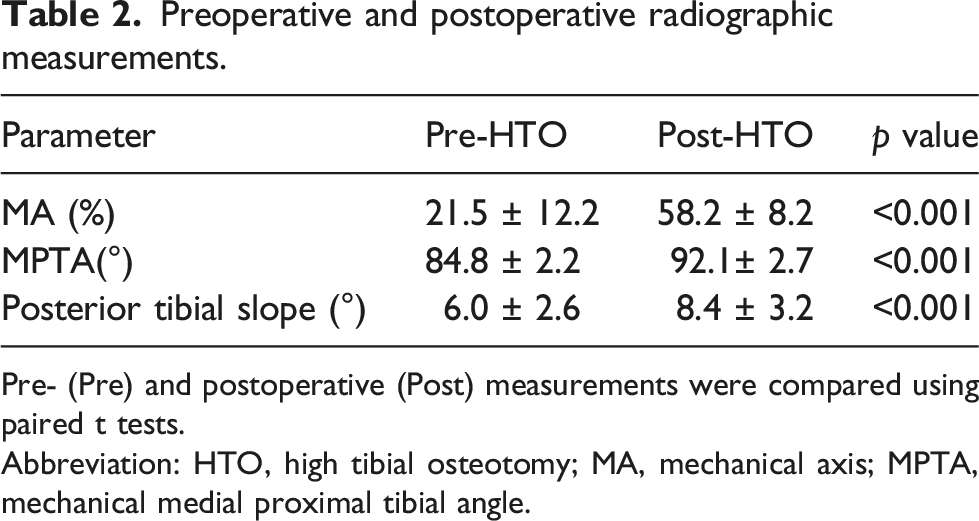
Pre- (Pre) and postoperative (Post) measurements were compared using paired t tests.
Abbreviation: HTO, high tibial osteotomy; MA, mechanical axis; MPTA, mechanical medial proximal tibial angle.
Preoperative and postoperative KOOS.
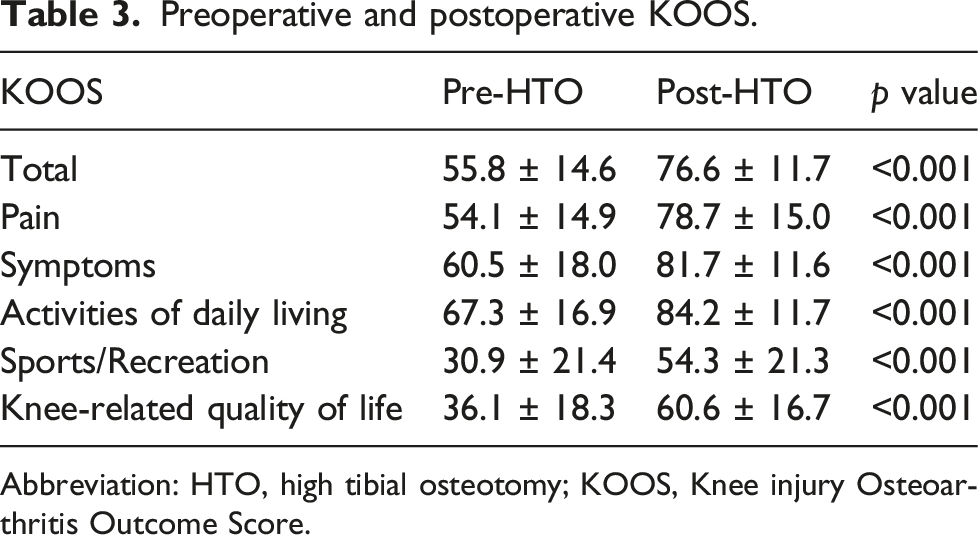
Abbreviation: HTO, high tibial osteotomy; KOOS, Knee injury Osteoarthritis Outcome Score.

Preoperative Caton–Deschamps index (CDI) (preCDI) and postoperative CDI at 2 weeks (W) and at 3, 6, and 12 months (M) (post2WCDI, post3MCDI, post6MCDI, and post12MCDI) after medial open-wedge high tibial osteotomy. PreCDI versus post2WCDI, preCDI versus post12MCDI, and post2WCDI versus post3MCDI were significantly different. *p < .05.
Multiple comparison procedure using Tukey’s post-hoc test.

Abbreviation: CDI, Caton–Deschamps index; post2W, 2 weeks postoperatively; post3M, 3 months postoperatively; post6M; 6 months postoperatively; post12
The time points at which a significant difference was detected were defined as Δpre-post2WCDI (preCDI − post2WCDI), Δpre-post12MCDI (preCDI − post12MCDI), Δpost2W-post3MCDI (post2WCDI − post3MCDI), Δpost2W-post6MCDI (post2WCDI – post6MCDI), and Δpost2W-post12MCDI (post2WCDI – post12MCDI).
Multiple regression to predict Δpre-post2WCDI based on preoperative radiographic parameters.

Abbreviation: Δ, change; BMI, body mass index; CDI, Caton–Deschamps index; KL, Kellgren–Lawrence; MA, mechanical axis; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; post2W, 2 weeks postoperatively.
Multiple regression to predict Δpre-post12MCDI based on preoperative radiographic parameters.

Abbreviation: Δ, change; BMI, body mass index; CDI, Caton–Deschamps index; CI, confidence interval; KL, Kellgren–Lawrence; MA, mechanical axis; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; post12
Multiple regression to predict Δpost2W-post3MCDI based on preoperative radiographic parameters.

Abbreviation: BMI, body mass index; CDI, Caton–Deschamps index; KL, Kellgren–Lawrence; MA, mechanical axis; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; post2W, 2 weeks postoperatively; post3M, 3 months postoperatively.
Multiple regression to predict Δpost2W-post6MCDI based on preoperative radiographic parameters.

Abbreviation: BMI, body mass index; CDI, Caton–Deschamps index; KL, Kellgren–Lawrence; MA, mechanical axis; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; post2W, postoperative 2 weeks postoperatively; post6M, 6 months postoperatively.
Multiple regression to predict Δpost2W-post12MCDI based on preoperative radiographic parameters.
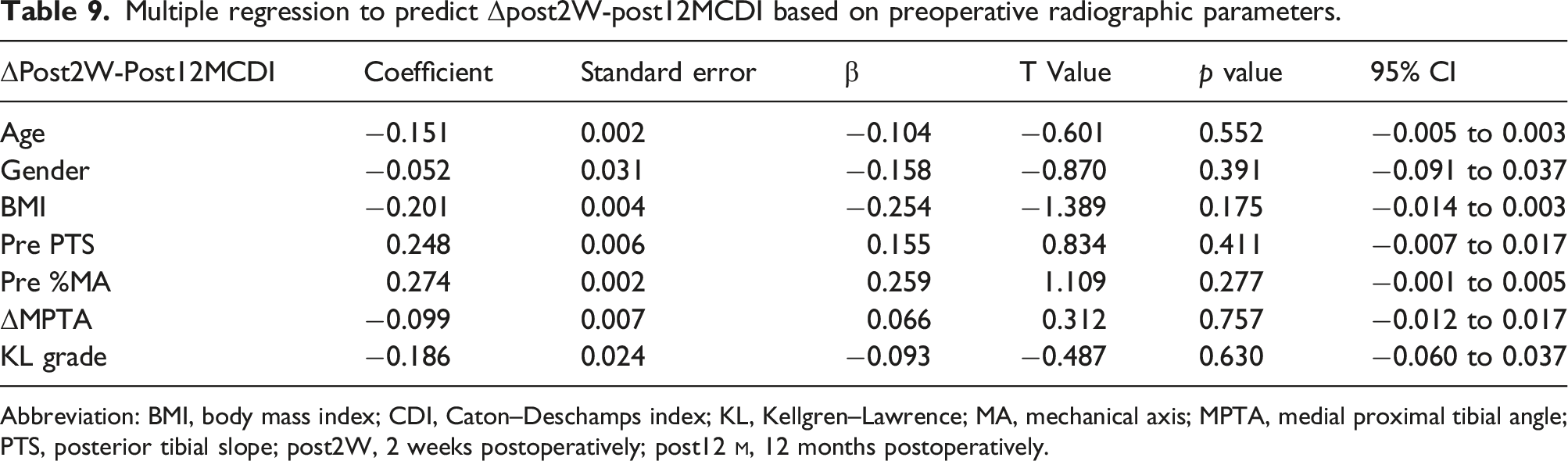
Abbreviation: BMI, body mass index; CDI, Caton–Deschamps index; KL, Kellgren–Lawrence; MA, mechanical axis; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; post2W, 2 weeks postoperatively; post12
Spearman’s rank correlation coefficient analysis between ΔCDI and ΔKOOS (pre-post12
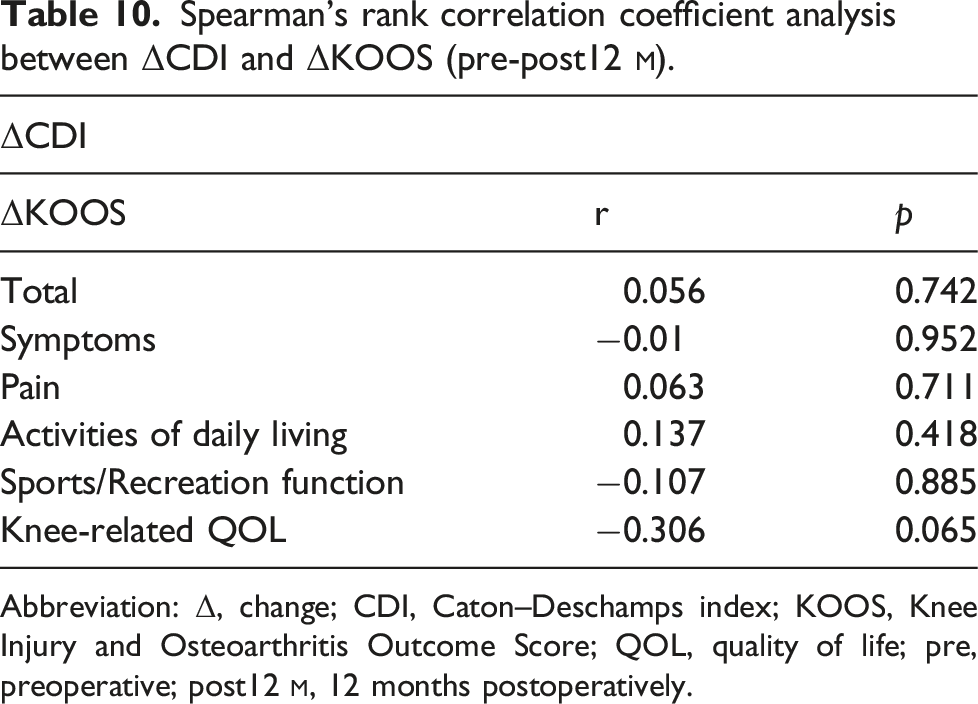
Abbreviation: Δ, change; CDI, Caton–Deschamps index; KOOS, Knee Injury and Osteoarthritis Outcome Score; QOL, quality of life; pre, preoperative; post12
The reliability of the measurements was assessed by estimating the intra-observer and inter-observer reliability using the intraclass correction coefficient (ICC). The ICCs were 0.81–1.00 (intra-observer variance) and 0.81 to 1.00 (inter-observer variance).
Discussion
The most important finding in the present study was that the change in patellar height decreased from 2 weeks to 3 months postoperatively after MOWHTO. This suggests that the change in patellar height had not finished immediately after surgery; rather, it continued to change sequentially. Several reports have described changes in patellar height between pre CDI and early post CDI, or between pre CDI and CDI measured 12 months after surgery 6,9,18–20; however, we evaluated sequential changes in patellar height and the factors causing sequential changes in patellar height after MOWHTO. Although the change in patellar height from 2 weeks to 3 months postoperatively was small, a previous cadaver study reported that patellar femoral (PF) contact force increased by 3% per 1-mm of change in patellar height. Therefore, this small change is suggested to be clinically significant. 21
Different methods are available to measure patellar height, such as the ISI, BPI, CDI, and the femoral patellar height Index (FPHI). BPI depends on the change in the PTS, which frequently occurs in HTO; thus, BPI should not be used in HTO. 17 Meanwhile, ISI shows poor reproducibility and repeatability because of the difficulty in locating the patellar tendon and the anterior tibial tubercle on postoperative X-ray.5,16
Although several reports have noted that patellar height decreases after MOWHTO, Ihle et al. reported that the FPHI indicates the change in patellar height change after MOWHTO. 22 However, the authors did not analyze the relationship between correction and patellar height. Although the FPHI showed good to excellent intra-observer and inter-observer reliability, which can be measured using standing long-leg radiographs, we consider that if patients have extension contracture, this measurement method is unsuitable. Many reports have shown that CDI is a reliable and reproducible method, and it is also a more direct method to measure patellar height than ISI, which measures the patellar tendon length.5,14
Distalization of the tubercle is the most likely factor causing patella baja. Closed-wedge HTO should mechanically raise the patella by lowering the joint line. During Distal-Tuberosity Osteotomy (DTO), the tibial tuberosity remains attached to the proximal tibia and may not change the patellar height. However, some cases of patellar height reductions have been reported after DTO; therefore, patellar tendon contracture may change patellar height. 23 Several reports have noted that any type of HTO may reduce the patellar height due to the patellar tendon contracture.9–11 Many reports have evaluated the patellar height after MOWHTO at two time points (preoperative and postoperative). These reports have suggested that patellar height is reduced postoperatively compared with preoperatively. However, the time point at which the change in patellar height ceases has not yet been reported. Some studies have reported that patellar tendon contracture may affect the change in patellar height after MOWHTO. Therefore, we hypothesized that patellar height changes sequentially after MOWHTO. This is the first report to show the sequential change in patellar height and the factors affecting the change in patellar height after MOWHTO in detail. It is not possible to prevent the reduction in patellar height caused by distalization of the tibial tuberosity direct after surgery, and it is also difficult to restore the original patellar height. However, it is possible to prevent the sequential change in patellar height directly after surgery by continuing rehabilitation to prevent patellar tendon contracture. Thus, surgeons should evaluate sequential changes in patellar height after MOWHTO.
Otsuki et al. reported that CDI decreased by 1.7% per 1° of correction angle. 24 In our study, ΔMPTA was associated with ΔCDI (pre-post2WCDI and pre-post12MCDI), indicating that correction angle is negatively associated with the change in patellar height change, as we expected. Although one of our objectives was to determine the factors affecting patellar height change from post2WCDI to post3MCDI, we identified no such factors. Δpost2W-post3MCDI may be affected by patellar tendon contracture, and because patellar tendon contracture may reduce patellar height without radiographic changes, sequential patellar height changes on radiography and sequential patellar tendon quality evaluation using magnetic resonance imaging (MRI) and elastography may clarify the details.
An increased in patellar femoral (PF) contact pressure owing to patella baja may be related to cartilage degeneration, anterior knee pain, and crepitus.25,26 Although this study showed a small change in patellar height from directly after surgery, it has been previously reported that even a 1 mm reduction in patellar tendon length causes a 1° loss of knee flexion and an increased risk of patellofemoral pain. 27 However, this study showed no correlation between ΔCDI and ΔKOOS. Previous reports have noted that PFOA progression and patellar baja do not affect clinical scores.20,28 However, clinical scores specific to the PF joint have not been obtained in the previous studies and this study. Therefore, measurements of functional outcomes specific to the PF joint are needed.
This study has several limitations that should be noted. First, this was a retrospective study. Second, the follow-up duration may have been too short to evaluate the clinical outcomes. It is possible that the clinical outcomes may have worsened with PF joint deterioration during the mid- or long-term follow-up. Third, the sample size was small. However, the number of patients exceeded the minimum number of patients required for the post-hoc analysis to achieve a power of 0.8. Fourth, we did not evaluate the patellar tendon directly using MRI or elastography; thus, further studies should make use of these approaches.
Conclusion
Patellar height was reduced immediately after MOWHTO and the change progressed until 3 months after MOWHTO. Although ΔMPTA was associated with the change in patellar height preoperatively compared with 2 weeks postoperatively, no factors associated with the change in patellar height from 2 weeks postoperatively to 3 months postoperatively were identified.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.