
Abstract
Objective
To examine the incidence and risk factors of any-cause reoperation after primary ACLR in children and adolescents.
Design
Retrospective Cohort
Setting
Electronic medical records from a large tertiary care, single institution integrated healthcare delivery system.
Patients
Patients were under the age of 18 years and had anterior cruciate ligament reconstruction. They were excluded if they had a multi-ligamentous knee injury or <1 year follow-up.
Interventions
Patients were further identified to have undergone a subsequent knee operation ipsilaterally or contralateral ACLR.
Main outcome measures
The rate of any-cause reoperation was our primary outcome measure.
Results
The median age was 16. There were 208 females (53.9%) and 178 males (46.1%) included. The median follow-up was 25 months with a minimum of 12 months (interquartile range: 16.0, 46.0). The rate of any-cause reoperation was 34.7%. There was no statistically significant difference between those who underwent reoperation versus those who did not undergo reoperation relative to age, sex, BMI, graft type, or the presence of concomitant meniscal injury. The rates of ipsilateral ACLR and contralateral ACLR at any time during the study period was 8.0% and 10.9% respectively. There was no statistically significant difference for rate of reoperation between graft types, between various concomitant injuries, between those who underwent meniscus repair or no repair.
Conclusions
This study reflects a 34.7% rate of a subsequent knee operation after ACLR in patients younger than 18 years. These findings can be used to inform pediatric patients undergoing primary ACLR on their risk of returning to the operating room.
Introduction
The rates of anterior cruciate ligament (ACL) injury and ACL reconstruction (ACLR) in children and adolescents have increased significantly in recent years.1–4 This increase may be explained by an increase in the number of children/adolescents participating in organized sporting activities, increased sport specialization, and/or advancing medical diagnostics/imaging identifying ACL injuries that may have previously gone undiagnosed.4,5 Also, it has been demonstrated that a delay in treatment of ACL tears in younger patients whether it be as little as 150 days 6 or more than a year 7 is associated with increased risk of meniscal and chondral injuries, with the most common being medial meniscus tears.6–10 Many studies have demonstrated an increased risk of re-injury following primary ACLR in younger patients.11–13 Risk factors for ipsilateral or contralateral ACL re-injury following primary ACLR include younger age, sex, increased activity level, use of allograft, and earlier return to sport.11,12,14,15 There remains a gap in the literature for large, population-based studies that examine the risk of all-cause reoperation after primary ACLR specifically in children and adolescents. The purpose of this study was to examine the incidence and risk factors of repeat surgery after primary ACLR in pediatric and adolescent patients within a single, closed healthcare system.
Materials and methods
We obtained approval from the Institutional Review Board for this single institution retrospective chart review. Patients were identified from 2006 – 2018 who underwent ACLR using the Current Procedural Terminology code (29888). All surgeries were performed by physicians within a large tertiary care, integrated healthcare delivery system. 16 These patients were then filtered to only include those patients who were younger than 18 years of age at the time of their primary ACLR. Patients were further identified to have undergone a subsequent knee operation ipsilaterally, or contralateral ACLR. Patients were further identified to have undergone a subsequent knee operation, either ipsilaterally or contralaterally. Identification of the subsequent procedure(s) was performed utilizing CPT codes (29888, 29870, 29871, 29873, 29874, 29875, 29876, 29877, 29879, 29880, 29881, 29882, 29883, 29884, 29889). Standard demographic variables and other patient level data (i.e. concomitant diagnoses, sex, age, race, BMI, graft type/size, associated pathology) were collected. All patients with a multi-ligamentous knee reconstruction at their index procedure or ACLR prior to the study period were excluded. Patients who were noted to have a concomitant collateral ligament injury not requiring repair or reconstruction at their index procedure were included. All patients who had less than 1 year of follow-up were also excluded. The electronic medical record was reviewed for each patient including preoperative and postoperative clinic notes, operative reports, and implant logs. For each of the three most commonly used techniques for ACLR (Bone-Tendon Bone autograft, 17 Hamstring autograft, 18 and Allograft 19 ), well described techniques were utilized. When a post and washer was used, a bicortical screw on the tibial side was utilized, with the distal traction sutures tied around the screw once appropriate tension was confirmed.
Patients who underwent primary ACLR without a subsequent operation were compared to those who had primary ACLR with a subsequent operation. The specific causes of reoperation were identified and recorded. Only the cause for the first reoperation was included in the overall reoperation analysis. In cases of multiple reoperations, if the cause for any of the reoperations after the first was revision ACLR or Contralateral ACLR, this was recorded and analyzed separately. Patients in whom a meniscus tear was identified at the index ACLR surgery were compared in two groups: those who had meniscus repair and those who had only partial meniscectomy or no meniscal intervention during their primary ACL procedure.
Continuous variables were summarized using means and standard deviations for normally distributed data or median and interquartile range (IQR) for non-normally distributed data. Categorical variables were summarized using frequencies and percentages. Demographic and clinical characteristics were compared using chi-square tests for categorical data and the Kruskal-Wallis test for non-parametric continuous data. Incidence rates of reoperation following primary ACLR and other factors are reported. Descriptive statistics for follow up of the non-reoperation group patients were generated using the number of months between the primary surgery date and last follow-up date. Kaplan-Meier methods were used to calculate median time to reoperation for all patients and by BMI class. All analyses were performed using SAS v9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Demographic information for all ACL reconstruction by reoperation status.

Clinical characteristics information by reoperation status.

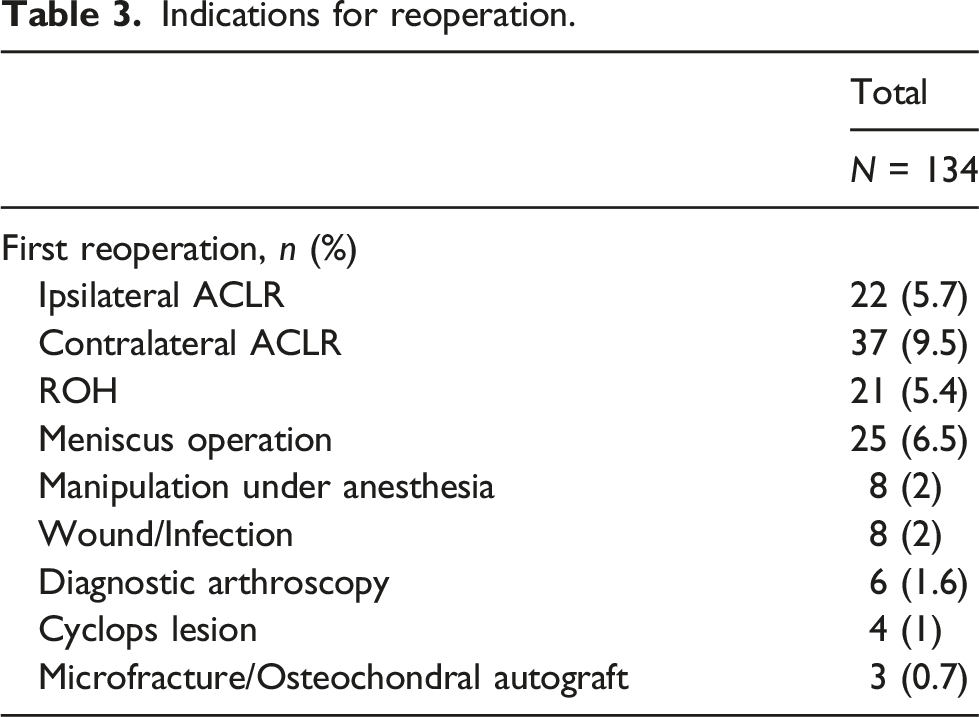
Indications for reoperation.

Reoperation separated by year.
Demographic and clinical characteristics were analyzed for all ACL reconstructions and compared by 3 BMI categories. Sex distribution was not equally distributed (p = .0067) throughout BMI classes with more females being underweight or normal weight (60.0%), while males were more representative in the overweight and obese groups (58.2% and 55.0%, respectively). There was no difference found in reoperation status when patients were stratified across 3 BMI subgroups.
Reoperation rates, including ipsilateral reoperation and contralateral ACLR, for each of the graft types including BTB autograft (30.2%), hamstring autograft (39.8%), other graft types (41.2%) are shown in Figure 2. There was no statistically significant difference for rate of reoperation amongst graft types (ipsilateral ACLR). There was also no significant difference for rate of graft failure when comparing allograft versus autograft. Rates of reoperation in patients with specified graft types and various concomitant injuries are shown in Figure 2 and Table 4 respectively. No statistically significant difference was seen between the groups with reoperation and those with either: no concomitant injuries (35.1%), meniscus tear (34.3%), multiple injuries (31.6%), or Collateral ligament tear not requiring reconstruction (60.0%). As shown in Table 5, there was no difference in the rate of reoperation for patients with a meniscus tear who underwent meniscus repair versus those with a meniscus tear who had partial meniscectomy or no intervention for the meniscus tear (34.5% vs. 33.3%, respectively, p = .8630). The median time to ipsilateral ACLR as the first cause for reoperation was 18 months (IQR: 10–30), compared to all other causes for first reoperation which was 15 months (IQR: 9–27). This difference was no statistically significant (p = .8455). The median time to second ACLR for ipsilateral ACL tear at any time during the study period was 16.6 months (IQR: 9.711, 28.3) compared to contralateral ACL tear which was 22.1 months (IQR: 13.8, 33.1). This difference was not statistically significant (p = .1647). Reoperation separated by graft. Distribution of concomitant injuries by reoperation. Comparing Rate of Reoperation for Meniscus Repaired or Not Repaired Among Patients with Meniscus Tear Identified at time of Index ACLR.


Discussion
We found that 34.7% of patients required another operation on their ipsilateral or contralateral knee following an index ACLR. This demonstrates that there are relatively high rates of re-operation following index ACLR in children and adolescents. The reasons for re-operation were not limited to ipsilateral graft failure—other reasons included contralateral ACL rupture, new meniscal pathology, and hardware removal. Contralateral ACL rupture was the most common reason for re-operation in this series. In a recent study by Defrancesco et al. looking at 419 pediatric patients who underwent primary ACLR, the most likely reason for reoperation at 3 years was ACL graft rupture followed by contralateral ACL rupture. 20 Their reported rate of reoperation at 3 years was 16.5%. Another study showed a 13.2% reoperation rate with the most likely reason being graft rupture, but they did not include contralateral ACLR in their rate for return to OR. 21 Both of these studies demonstrate a lower reoperation rate than the current study. Compared to the latter study, our rate of return to the OR was 25.1% if we exclude contralateral ACLR. The rate of 34.7% seen in our study was achieved by calculating the sum of each cause for first time reoperation. This is different than the Kaplan-Meier method that the Defrancesco study used to estimate all-cause return to OR, which is fundamentally less because competing risks blocked the others’ effects.
It has been demonstrated that nearly 25% of young athletic patients who sustain an ACL injury and return to sport will go on to sustain a second ACL injury in their career, frequently soon after they return to sport. 22 Many factors can influence the success of ACLR including surgical technique, graft type or fixation, concomitant injury, postoperative rehabilitation, patient education, timing of return to play, and young age.11,23 Younger age, and early return to play have been identified as two independent risk factors for re-injury after ACLR, with young patients being at a significant risk for both graft rupture and contralateral ACL injury.11,22 In a cohort of patients described by Wiggins et al., the rate of a second ACL injury in patients younger than 25 years old who return to sport was 23% (contralateral + ipsilateral). Our study found a graft rupture rate of 8.0% and a contralateral ACLR rate of 10.9%. This contrasts with the Heath et al. study which demonstrated a revision rate nearly double the contralateral rupture rate, when living donor hamstring tendon grafts were used (20.6%, and 11.3%, respectively). 24 When looking at incidence of a second surgery, Cordasco et al. showed that adolescents with 2–3 years of growth remaining were at a significantly higher risk for reinjury (20% revision ACLR) than those with 3–6 years of growth remaining (6% revision ACLR) and those who were skeletally mature (6% revision ACLR). 25 This stands in contrast to a study done using the Swedish registry data which found an overall revision rate after ACLR of 1.1% and 2.6% at 2 years and 5 years respectively. 26 The authors note that patients may have been exposed to less sporting activity which may help explain their low revision rate compared to others noted in the pediatric and adolescent literature. The median age of our patients in this study was 16 years with an average time to reoperation for revision ACLR of 16.6 months and contralateral ACLR of 22.1 months. Given our median age of 16 years and revision ACLR for graft rupture rate of 8.0%, our study seems to have similar results to the Cordasco study group of skeletally mature adolescents. Our rate being 2.0% higher with respect to revision ACLR may be attributed to the inclusion of patients of all ages in our reported rate. Our study demonstrates a rate of second ACL injury that is 4.1% less than the study performed by Wiggins et al. We did not track return to sport, so it may be that some of our patients did not return to sport and therefore our rate was lower than previously cited.
Because the literature shows that younger age is a risk factor for re-injury after ACLR,11,22 we expected this age group would have a relatively higher overall reoperation rate as well. The adult literature has wide ranging rates reported for return to the operating room after isolated ACLR. One study in patients who had ACLR, found a rate of 10.3% when looking at subsequent surgery in a patient population with an average age of 29.6 years. 27 Hettrich et al. report a rate of 18.9% for return to operating room after ACLR when looking specifically at the ipsilateral knee in their adult population after 6 years. 28 This is less than our current study which showed a 25.2% rate of reoperation when examining only the ipsilateral knee. Lyman et al. found a rate of 6.5% when examining subsequent reoperation within 1 year; this study included patients of all ages. 29 In a study looking prospectively at patients after ACLR, Shelbourne et al. found 17% subsequent injury rate in the <18 years old group, 7% in the 18–25 years old group, and 4% in patients >25 years. 30 The rate of a subsequent reoperation for meniscal pathology after acute primary ACLR is not well known. Prior studies have shown that pediatric and adolescent patients with ACL deficient knees have poor outcomes with respect to subsequent instability, inability to return to sport, joint arthrosis, and other knee symptoms.14,31 More than just the ACL injury, there are a significant number of associated knee injuries which can necessitate operative intervention. 32 Despite the advancements in diagnosis and treatment of ACL injuries, Whittaker et al. found that young adults with a history of a sport-related knee injury demonstrate greater clinical symptomatology consistent with the development of post traumatic osteoarthritis and an increased likelihood of developing obesity 3–10 years post injury. 33 Previous studies corroborate the greater post-injury symptomatology and discuss treatment and rehabilitation strategies for minimizing it.34–37 Millet et al. showed that there was a higher incidence of medial meniscus tears requiring operative treatment (repair vs. partial meniscectomy) in chronically ACL-deficient knees or delayed ACLR when compared to lateral meniscal injury in the acute setting, similar to the adult population. Many authors now advocate for early surgical stabilization of the ACL-deficient knee in children and adolescents to potentially help prevent further intra-articular knee injury.6–10,14,32,37,38 In the current study the rate of reoperation for treatment of isolated meniscal pathology was almost 7%, including those who had meniscus repair, partial meniscectomy, or no intervention regarding their meniscus at the time of index ACLR.
One cause for return to the OR that was higher than we expected was the removal of hardware. In the previously cited studies looking at reoperation after ACLR, the cited rate of hardware removal during the study period was less than 1%.20,21 Our rate of hardware removal was 5.3% and was most frequently a cortical screw and washer on the tibial side. In a study by Almeida et al. they demonstrated a 10.8% rate of hardware removal in patients who had a screw and washer construct on the tibial side for fixation. 39 Another study in which the surgeon used primarily interference screws for fixation on the tibial side, demonstrated the rate of hardware removal at about 5%. 40 Our findings were more like these two studies as compared to the previously cited reoperation studies. Given our surgeons’ use of post and washer construct preferentially, we feel this rate is comparable to prior studies. Utilizing a suture anchor or a different, lower profile device, may be beneficial if the treating surgeon feels a post-washer construct is an important aspect of their treatment.
Although the surgeons in the current study used mostly autografts at the time of index ACLR, there were still a relatively large number of patients who had allograft ACL reconstruction. The majority of included patients in whom allograft was utilized, were from a single surgeon who treats adults in addition to pediatric patients and exclusively utilizes allograft for all ACLR. Allograft should be considered carefully in pediatric and adolescent patients. It has been shown in the literature that allograft reconstruction and higher activity level are both risk factors for increased odds of graft failure in the young, active population.41,42 In patients between ages 11–18 years, Engelman et al. calculated the hazard ratio of graft failure to be 4.4 when comparing the use of allograft to autograft. 43 Further, when specifically studying patients <18 years old, Ellis et al. found a 15 times higher rate of graft failure when comparing Bone-Patellar Tendon-Bone allograft versus Bone-Patellar Tendon-Bone autograft. 44 In contrast, Shah et al. found no difference in failure rates between age groups using freeze-dried achilles tendon allograft in primary ACLR. 45 Although the current study is one of the largest to look at reoperation rates in pediatric and adolescent patients after ACLR, and we had 59 patients in whom allografts were used, it was still underpowered to detect a difference in terms of graft failure when comparing allograft and autograft (p = .0901), as revealed by post hoc power analyses of subgroup comparisons. Additionally, patients in our study were followed for a minimum of 12 months which is less than the previous studies looking at allograft ACLR which only included patients with at least 24 months follow-up.
There are a few limitations of this study. This study was by design a retrospective cohort, without the intention to investigate causes for ACL re-tear, return to sport, or specific technical considerations of ACL reconstructive surgery. Given its retrospective nature, this study was not designed with power or sample size considerations for subgroup analyses. Therefore, the reported subgroup results should be considered with this limitation in mind. Also, the median age of our patients was 16 years which may limit the generalizability among pediatric patients to those with closed physes. The status of physeal closure was not recorded. While angular deformity from transphyseal technique is certainly a consideration, it has been previously noted that there is minimal growth around the knee after age 13 years in girls and 14 years in boys.35,46 In our study all patients who received BTB autograft were girls older than 13 years and boys older than 14 years. The inclusion of patients with a minimum of 1 year follow-up is less than the ideal 2 year follow-up seen in similar studies. This may lead to a decreased rate of reoperation in our study compared to what the actual rate may be due to not including some patients who may have had a reoperation at another institution after 1 year. Further, despite our large catchment area and integrated healthcare delivery system, there may be several patients who decided to have their second surgery elsewhere which would increase the rate of reoperation from what is reported. Further, given that our rate of reoperation is increased compared to the literature, we think it unlikely that our population is leaving the system in a such a volume that a difference would be detected. Despite these limitations, we were able to address the specific aims of the study, namely, evaluating the overall rate that children and adolescents return to the operating room for any reason after ACLR.
Conclusions
This study focused on the all-cause rate of return to the OR in pediatric and adolescent patients <18 years old within a closed health care system and found a 34.7% rate of a subsequent knee operation after index ACLR. There were no identifiable independent risk factors for reoperation within the study population. The findings of the current study can be used to inform pediatric patients undergoing primary ACLR on their risk of returning to the operating room for any reason and future work should attempt to study modifiable factors that can reduce this risk.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.