
Abstract
Introduction
Hallux valgus is a common forefoot deformity characterized by lateral deviation of the great toe and medial deviation of the 1st metatarsal bone, with prevalence of 3.5% among adolescent population. 1 The deformity is associated with functional impairment such as foot pain, abnormal gait pattern, or even risk of falling in elderly people.2–4 Radiographs are required for pre-operative assessment, surgical planning and post-operative evaluation.5,6 In addition, the recurrent rate after surgical correction can be predicted from post-operative radiographic parameters.7,8
Basically, angular deformity of medial column is the main part to be evaluated in clinical practice. The commonly used parameters comprise of 1,2 intermetatarsal angle(IMA), hallux valgus angle(HVA), hallux valgus interphalangeal angle(HVIA), and distal metatarsal articular angle(DMAA). However, deformity of 1st metatarsal bone consist not only angular deformity in transverse plane but also deformity in coronal plane which is 1st metatarsal pronation. Radiographic assessment with only degree of valgus or varus angulation is evidently not comprehensive enough for hallux valgus. The rotational deformity of 1st metatarsal bone becomes more remarkable in terms of their association with recurrent rate following surgery.7,8 The tibial sesamoid position in anteroposterior view of radiographs and 1st metatarsal head shape are important parameters for assessing the 1st metatarsal pronation and sesamoid subluxation.9,10 These radiographic parameters should be used to assess hallux valgus and they should be accurate, reliable and reproducible.
At present, weight-bearing CT scan or cone-beam CT scan has increasing role in evaluation of various foot and ankle conditions including hallux valgus. Several literatures investigated methods of assessment in hallux valgus especially for 1st metatarsal rotation.11–16 In addition, the role of CT scan for hallux valgus evaluation is still questioned whether it is crucial to be used in every patient or plain radiographs are already adequate for evaluation. In addition, there is still limitation in evidence representing reliability in parameter assessment of both plain radiograph and weight-bearing CT scan especially in post-operative period of hallux valgus which bony anatomy was distorted and obscured with implants. This study aimed to comprehensively assess the reliability of parameter measurement in hallux valgus from both plain radiographs and weight-bearing CT scan. Our primary hypothesis was weight-bearing CT scan could provide better reliability compared to plain radiographs, especially for assessment of coronal plane deformity.
Methods
The ethical consideration was approved from the Committee on Human Rights Related to Research involving Human Subjects in Faculty of Medicine Ramathibodi Hospital, Mahidol University (MURA2020/268). A total of 40 pre-operative plain radiographs, 40 post-operative plain radiographs, and 37 weight-bearing CT scan were retrospectively recruited in this study. Post-operative radiographs consisted of various hallux valgus procedures without other foot operation. Three orthopaedic surgeons individually assessed all the radiographic pictures. Prior to the process, bony landmarks and methods of each parameter measurement and digitally technique using PACS (Picture Archiving and Communication System) for assessment were trained and agreement was made for all assessors. Each assessor measured all radiographs 2 times with at least 6-week apart and in the different order of radiographs. Assessors evaluated the radiographs separately and were blinded about patients’ identification.
Parameters assessment
The dorsoplantar view of weight-bearing foot plain radiograph was used for evaluation. All of the 6 parameters were defined with the detail of landmark measurements according to standard measurement methods which were 1. 1, 2 intermetatarsal angle (IMA): the centers of proximal and distal metaphyso-diaphyseal area of 1st and 2nd metatarsal bone were marked as the axis of each bone. The intersection of 1st and 2nd metatarsal axes was defined as 1,2 intermetatarsal angle. (Figures 1A and 2A). 2. Hallux valgus angle (HVA): The centers of proximal and distal metaphyso-diaphyseal area of proximal phalanx of great toe were marked as the axis of the bone. The intersection of 1st metatarsal and great toe proximal phalanx axes was defined as hallux valgus angle. (Figures 1B and 2B). 3. Hallux valgus interphalangeus angle (HVIA): the midway of proximal articular surface of distal phalanx of great toe and the distal tip of the phalanx were marked. The line connecting between these 2 points was defined as the axis of great toe distal phalanx. The intersection of proximal and distal phalanx axes was defined as hallux valgus interphalangeus angle. (Figures 1C and 2C). 4. Distal metatarsal articular angle (DMAA): A line was marked between the most medial and lateral points of distal articular surface of 1st metatarsal bone. The intersection of 1st metatarsal axis and a line perpendicular to the line connecting distal articular surface was defined as distal metatarsal articular angle. (Figures 1D and 2D). 5. Tibial sesamoid position (TSP): the position of medial sesamoid bone was graded relative to the 1st metatarsal longitudinal axis, classifying as grade I to VII according to Hardy and Clapham,
17
which grade I-IV were considered as normal position while the others were displacement or outliers classified as subluxation.(Figures 1E and 2E). 6. First metatarsal head shape (head shape): the shape of lateral edge of the first metatarsal head was evaluated according to Okuda et al.
8
A circle was marked fit to the 1st metatarsal head articular surface. The shape of the lateral edge was classified into 3 types depending on the maximal distance between the lateral cortical edge of metatarsal head and the circle: angular (distance ≥2 mm), intermediate (distance between 1-2 mm), and rounded (distance <1 mm). The round type was meant as increased pronation of 1st metatarsal bone. (Figures 1F and 2F) Measurement of pre-operative radiographs: (A) 1, 2 intermetatarsal angle (IMA); (B) Hallux valgus angle (HVA); (C) Hallux valgus interphalangeus angle (HVIA); (D) Distal metatarsal articular angle (DMAA); (E) Tibial sesamoid position (TSP); (F) First metatarsal head shape (head shape). Measurement of post-operative radiographs: (A) 1, 2 intermetatarsal angle (IMA); (B) Hallux valgus angle (HVA); (C) Hallux valgus interphalangeus angle (HVIA); (D) Distal metatarsal articular angle (DMAA); (E) Tibial sesamoid position (TSP); (F) First metatarsal head shape (head shape).


Intermetatarsal angle, hallux valgus angle, hallux valgus interphalangeal angle and distal metatarsal articular angle were assessed in weight-bearing CT scan using the same methods as measured in plain radiographs. Additionally, rotation of 1st metatarsal bone was assessed by using α angle. The method of measurement started with drawing an inferior line between lateral edge of lateral sulcus and medial edge of medial sulcus. A superior line was defined between medial and lateral corners of 1st metatarsal head. Another straight line was drawn connected at the midpoint of inferior and superior lines then the angle was measured between this straight line and the vertical line perpendicular to horizontal ground axis.
11
(Figure 3) Measurement of α angle in axial cut of weight-bearing CT scan.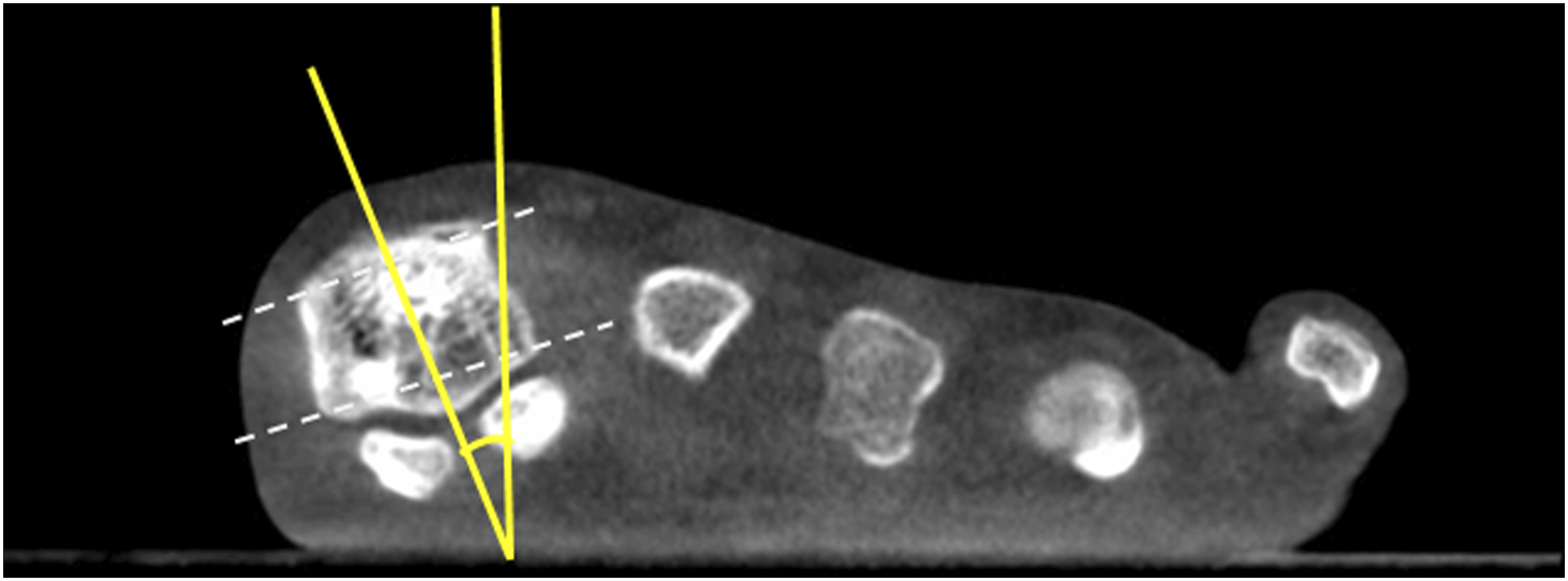
Statistical analysis
The inter-observer and intra-observer reliability for the measurement of each hallux valgus parameters were evaluated. The intraclass correlation coefficient (ICC) was calculated for continuous data (IMA, HVA, HVIA, DMAA, and α angle) as absolute agreement using a 2-way random effects model to investigate the intra-observer variability (single measurement) and inter-observer variability (average measurement). Reliability was classified as follows: poor, ICC ≤0.20; fair, ICC = 0.21 to 0.40; moderate, ICC = 0.41 to 0.60; good, ICC = 0.61 to 0.80; and very good, ICC = 0.81 to 1.00. A weighted kappa coefficient (κ) was used to determine consistency among observers for categorical data (TSP and head shape). The strength of examiner agreement was defined as follows: poor, κ ≤ 0.20; fair, κ = 0.21 to 0.40; moderate, κ = 0.41 to 0.60; good, κ = 0.61 to 0.80; and very good, κ = 0.81 to 1.00.18,19 Statistical analysis was performed with SPSS, version 20.0.0 (IBM Corp).
Results
Demographic data
A total of 34 patients, all female, were included. There were 6 patients (17.65%) included with bilateral feet. A total of 40 pre-operative plain radiographs, 40 post-operative plain radiographs, and 37 weight-bearing CT scan were evaluated. Mean age was 47.85 years (standard deviation 17.66, range 18–73 years). Both right and left feet were available 20 in each side for radiological appraisal. From 40 post-operative radiographs, Scarf osteotomy was done for 24 feet (60%), Chevron osteotomy was done for 5 feet (12.5%), Lapidus fusion was done for 5 feet (12.5%), first metatarsophalangeal fusion was done for 6 feet (15%), and medial eminence resection was done for 10 feet (25%). In order to correct the residual valgus deformity or the presence of hallux valgus interphalangeus, Akin osteotomy was done for 22 feet (55%).
Angle measurements
Inter-observer reliability of parameters in pre-operative and post-operative plain radiographs.

ICC: intraclass correlation coefficient; κ: weighted Kappa coefficient; CI: confidence interval.
Intra-observer reliability of parameters in pre-operative and post-operative plain radiographs.

ICC: intraclass correlation coefficient; κ: weighted Kappa coefficient; CI: confidence interval.
Inter-observer and intra-observer reliability of parameters in post-operative weight-bearing CT scan.
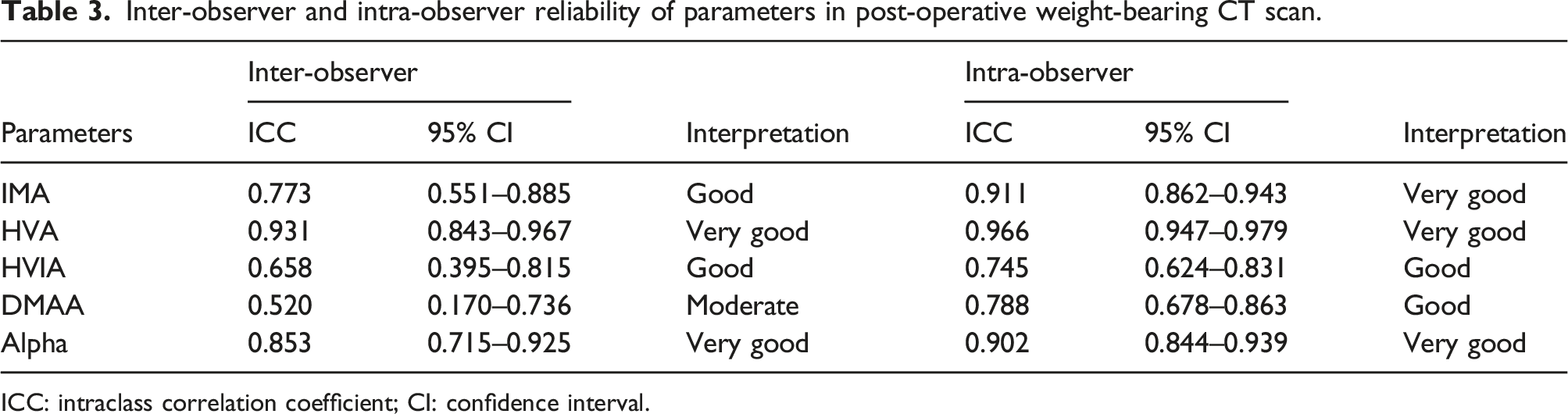
ICC: intraclass correlation coefficient; CI: confidence interval.
Discussion
In this study, the reliability of parameters from the plain radiograph and the weight-bearing CT scan was comprehensively evaluated. The inter-observer reliability of the transverse plane parameters in plain radiograph was better than the reliability of the coronal plane parameters. In weight-bearing CT scan, it was demonstrated that α angle which represents 1st metatarsal rotation or coronal plane deformity could improve the reliability in both inter-observer and intra-observer, while the reliability of transverse plane evaluation was showed to be comparable when measuring in plain radiograph.
Initially, evaluation of hallux valgus deformity has been focusing on angulation of hallux in transverse plane. Several literatures demonstrated reliability in radiographic measurement of hallux valgus since the process of parameters assessment has various roles in clinical practice from pre-operative planning to post-operative follow up period. Van der Woude et al. 20 studied on inter- and intra-observer reliability of radiographic HVA, IMA and DMAA in weightbearing and non-weightbearing conditions by 4 observers. The inter-observer reliability of all parameters was in very good level. The intra-observer reliability of HVA and IMA was very good while DMAA was variable by all observers from moderate to very good levels. Similarly, Lee et al. 21 evaluated radiographic correlation of various parameters of non-operated feet. The inter-observer reliability of HVA and IMA were very good [ICC (95% CI): HVA: 0.99(0.98–0.99), IMA: 0.90 (0.83–0.94)] but for DMAA was fair [ICC (95% CI): 0.38(0.15–0.59)]. Hence, the intra-observer reliability of HVA, IMA and DMAA were good to very good [ICC (95% CI): HVA: 0.99(0.98–0.99), IMA: 0.91(0.84–0.95), DMAA: 0.78(0.62–0.88)]. Scheele et al. 14 also evaluated various parameters of hallux valgus and calculated reliability of measurements from post-operative radiographs (modified Lapidus procedure). The radiographic parameters were evaluated by 3 observers. The inter-observer reliability of HVA was 0.77, 0.88 and 0.98; IMA was 0.89, 0.88 and 0.96; DMAA was 0.83, 0.77 and 0.96. The intra-observer reliability of HVA, IMA, and DMAA were assessed only by one observer which was 0.93, 0.83, and 0.96, respectively. The parameters represented interphalangeus deformity were specifically assessed by Hujazi et al. 22 and found inter-observer reliability of HVIA was very good in both pre-operative and post-operative radiographs [ICC: pre-operative = 0.83, post-operative = 0.86]. The intra-observer reliability was assessed in each observer which shown very good reliability for all [ICC: observer 1 = 0.81, observer 2 = 0.86, observer 3 = 0.91]. Most of inter-observer and intra-observer reliability of IMA, HVA, HVIA and DMAA from previous literature were good to very good which were similar to results in our study. Hence, plain film would already be proper investigation in assessment of hallux valgus angulation in transverse plane.
Coronal plane deformities of hallux valgus have been increasingly investigated as there were evidences suggested that remaining of rotational mal-alignment was associated with recurrence of deformity following operative correction.8,23 In order to assess the rotational deformity from the plain film, the 1st metatarsal head shape and tibial sesamoid position were parameters of choice. The 1st metatarsal head shape or lateral edge of 1st metatarsal head represented the degree of 1st metatarsal rotation. Okuda et al. 8 proposed the lateral edge of 1st metatarsal head and demonstrated the reliability of the measurement. The reliability of 1st metatarsal head shape was evaluated from 10 pre-operative and 10 post-operative radiographs (after proximal metatarsal osteotomy). The inter-observer reliability of 1st metatarsal head shape was 0.61 and 0.65 according to 2-round of assessment. Additionally, the intra-observer reliability was 0.64 of first observer and 0.65 of second observer. The tibial sesamoid position (TSP) in dorsoplantar view is the plain film parameter representing the rotational deformity of 1st metatarsal bone or sesamoid subluxation. When the TSP showed abnormal result, patient might have one of the two mentioned deformities or might have both. It was reported by Scheele et al. 14 about the inter-observer reliability of TSP from 3 observers were 0.98, 0.76 and 0.78. Additionally, the intra-observer of TSP was 0.83 which, overall, were good to very good reliability of inter-observer and intra-observer. In our study, we found the intra-observer reliability of TSP was good in both pre- and post-operative measurement but for head shape, the intra-observer reliability was moderate in both periods. The inter-observer reliability of pre-operative TSP and head shape was mostly moderate while in post-operative radiographs, the inter-observer reliability of TSP and head shape was mostly fair.
As the agreements of TSP and head shape measurements in plain radiographs which represent rotational deformity from this study were relatively lower compared with other parameters, especially in post-operative radiographs. We believe that the post-operative radiographs might provide unclear anatomical landmark for grading determination for TSP due to metal works, distorted bony landmarks and the position of sesamoid related to longitudinal axis is quite subjective in both pre- and post-operative radiographs. 21 In case of head shape evaluation, initially the articular margin which needed to be identified was probably not clearly shown on radiographs. In addition, the circular drawing according to articular margin in the process of measurement might be inconsistent enough for determination in various assessors. Therefore, the methods of rotational parameter measurements might not be reproducible in different conditions. The assessment of sesamoid position or 1st metatarsal rotation would need other investigation such as weight-bearing CT scan for improvement of reliability of rotational parameters.
Weight-bearing CT or cone-beamed CT scan is an evolved technology using in assessment various foot and ankle diseases under weight-bearing condition. This technology could provide radiographic picture more in details of bony structure and generate different plane of picture to be assessed. For hallux valgus, the utility and consistent in using weight-bearing CT scan for deformity evaluation were still unclear. Najefi et al. 24 assessed hallux valgus parameters from weight-bearing CT scan and presented that the inter-observer reliability of IMA, HVA and α angle was all very good [ICC: IMA = 0.90, HVA = 0.96, α angle = 0.83]. The intra-observer reliability of HVA was 0.91 and α angle was 0.95, while IMA showed only 0.54 for intra-observer reliability. We investigated the reliability of all transverse plane evaluation used in plain radiographs included α angle representing degree of 1st metatarsal rotation. This study focused on weight-bearing CT in post-operative radiographs as the landmarks for measurement possibly distorted from operative correction. The results showed very good inter-observer and intra-observer reliability only for α angle and HVA. Though the inter-observer and intra-observer reliability of IMA and HVIA were good to very good, the level of agreement was comparatively lower than results from plain radiographic assessment. Lastly, inter-observer and intra-observer reliability of DMAA were moderate and good, respectively, while evaluation in plain radiographs showed good reliability. According to the reliability results, assessment of 1st metatarsal rotation with weight-bearing CT scan is more preferable than plain radiographs.
This study had several strengths. First, the study was comprehensively assessed the reliability of all common radiographic parameters in both plain radiographs and weight-bearing CT scan. Second, the reliability specifically based on both pre-operative and post-operative conditions were evaluated which found less post-operative data in previous literatures. Third, the operated feet were chosen in various procedures which representing in various conditions of the patients. Fourth, the second-round measurement took place at least 6 weeks after the first one in random order to reduce possibility of recall bias.
Some limitations in this study were acknowledged. First, the normal feet were not included for the evaluation. However, the parameters would be easier to assess and might be more realistic in normal anatomic feet. Second, weight-bearing CT scan was provided only in post-operative period because the technology is quite new so that we were unable to gather the radiographs from pre-operative period. Third, the 3 dimensional picture of weight-bearing CT scan was not performed in this study due to the fact that additional advanced software was needed in order to measure parameters in 3D radiographs and to create 3D pictures, extra price must be included which might not be proper in every patient care.
Conclusion
Radiographic evaluation has an important role in patient care and management plan in hallux valgus. Apart from plain films, weight-bearing CT scan is increasingly used in assessment. From this study, assessment of rotational alignment of 1st metatarsal bone by α angle provided high reliability. However, in order to assess transverse plane deformity by various angular parameters from weight-bearing CT scan must be used with caution as the reliability was shown to be less compared with measuring in plain radiographs. Therefore, weight-bearing CT scan would provide better assessment in coronal plane deformity of hallux valgus but might unable to replace the role of plain radiographs.
Footnotes
Authorship
The conception and design of the study: S.P., S.L., T.T; - Acquisition of data: S.P., P.P., S.B.; - Analysis and interpretation of data: T.T.; - Drafting the article or revising critically: S.P., J.O.; - Final approval of the version to be submitted: T.T., S.L, S.P.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.