
Abstract
Background
To evaluate the safety and effectiveness of posterior closed-open wedge osteotomy for treatment of congenital kyphosis in children.
Methods
Imaging and clinical data from January 2010 to December 2019 of posterior closed-open wedge osteotomy of congenital kyphosis with at least 2-year follow up was analyzed retrospectively. Perioperative indicators such as operation time, osteotomy site, osteotomy method and occurrence of complications, and imaging indicators were observed. The 3D printed models were used to measure the expanded distance of anterior edge vertebra and closed length of spinal canal line. The clinical effect was evaluated through SRS-22 questionnaires.
Results
There were 15 CK patients in this study. The osteotomy segments and details are as follows: 1 case each for T6-9 and L2, 2 cases at T11, 3 cases at T12, and 6 cases at L1. The average operation time was 314 min, the average blood loss was 970 mL, the average fusion range was 6.3 segments, and the average time of follow up was 70.5 months. The Cobb angle of local kyphosis was corrected from 65.6 ± 18.8° to 11.3 ± 7.1°(p < .001). The range of kyphosis correction was 40–90°, and average correction rate was 83.2% (67.7–95.7%). The correction was stable in follow-up, and the kyphotic angle was 11.0 ± 7.6 (p = .68). The preoperative SVA was 31.5 ± 21.8 mm, and the postoperative recovery was 18.0 ± 15.5, while the last follow-up was 9.1 ± 7.9. The p values were 0.02 and 0.07 respectively. By using 3D printed models, the expanded distance of anterior edge vertebra and closed length of spinal canal line were 14.5 ± 7.5 mm and 24.5 ± 8.0 mm respectively. Self-image and satisfaction in SRS-22 improved significantly. There was no recurrence of deformity and junctional kyphosis.
Conclusions
The posterior closing-opening wedge osteotom for treatment of congenital kyphosis in children is satisfactory, if selected appropriately. During the longitudinal follow-up, the patients could achieve solid fusion and the correction could be well maintained.
Keywords
Introduction
Congenital kyphosis (CK) is a relatively rare congenital spinal deformity characterized by the partial backward angle. 1 The exact incidence of CK is not really known, but the rates may be around three to four per 10,000 newborn babies. 2 The CK tends to aggravate with age and leads to an imbalance in the sagittal plane of the spine, and about 25% of patients suffer from neurological loss.1,3–5 Because conservative treatments are usually ineffective 1 surgical treatments are commonly selected.
The early operations are usually divided into one-stage or two-stage surgical treatments with a combined anterior and posterior approach.6,7 Recently, single posterior osteotomy has become popular. The osteotomy techniques include transpedicular osteotomy (PSO), closed wedge osteotomy (CWO), and total vertebral resection (VCR). The first two osteotomy procedures are less traumatic with minimal complications, but the correction is often minimal. The third osteotomy procedure can achieve a greater correction, but the surgical trauma is the major concern.
Closed wedge osteotomy is the most commonly used surgical technique, which also includeds transpedicular osteotomy and hemivertebra resection. Compared to the VCR, it is less traumatic with minimal complications.8–11 However, the technique cannot be used for severe CK because the single-segment transpedicular osteotomy for the lumbar spine is less than 30° and for the thoracic spine is less than 25°.12,13
The purpose of this retrospective study was to evaluate the safety and effectiveness of
Materials and methods
This retrospective study was approved by the institutional review boards of the hospitals involved in accordance with international agreements (World Medical Association Declaration of Helsinki “Ethical Principles for Medical Research Involving Human Subjects,” amended in October 2013. Informed consent and Health Insurance Portability and Accountability Act consent were obtained from each patient.
From January 2010 to December 2019, 21 children with CK underwent a single-stage posterior spinal osteotomy and fusion in our hospital. Preoperatively, full length anteroposterior and lateral X-rays of the spine were taken with the patient in the standing position. Three-dimensional reconstruction of the whole spine was produced from CT scan. Magnetic resonance imaging of the whole spine was taken to obtain the detailed images of the spinal column and para-vertebral structures. The inclusion criteria were as follows: (1) kyphosis angle≥ 45°; (2) patients undergoing COWO; (3) patients with at least 2-year postoperative follow-up; (4) complete perioperative data, imaging data, and follow-up data. The following exclusion criteria were applied: (1) patients with scoliosis more than 10°; (2) patients with any previous history of spinal surgery. (3) severe malformation of other organs. Finally, a total of 15 patients were enrolled in this study. All operations were performed by the same senior surgeons. Preoperatively, three-dimensional printed spine models were made for facilitating osteotomy based on the angle of spinal deformity.
Surgical techniques
The operation was performed under general anesthesia. The patient was placed in the prone position with padding of all bony prominences. We made a midline skin incision centered over the involved segment located using fluoroscopy. Subperiosteal dissection was performed to expose the spinous process, lamina, facet joint process, and the transverse process of the involved levels. Spine pedicle screws (Titanium 3.5-, 4.5-, and 5.5-mm, Shang Hai San You MEDICAL CO) were inserted with the freehand technique. Screw positioning was guided using a guide plate and C-arm fluoroscopy. Guided pins were placed to confirm the correct level. Hemivertebra osteotomies were performed using three different techniques (i.e., single-level, double-level, and multilevel vertebral osteotomies) (Figures 1, 2, and 3) according to the deformities of kyphosis, which were planned based on the preoperative spine models. We removed the spinous processes. We performed piezosurgery osteotomy to remove the bilateral lamina of the affected vertebrae and a portion of the lamina and articular processes of the adjacent vertebra. When performing a thoracic osteotomy, a 2–3 cm long segment of the corresponding rib was removed to facilitate deformity correction. The spinal canal and spinal cord were exposed, and the fat and other soft tissues surrounding the spinal cord were removed to visualize the spinal dura mater. We used a temporary short rod to connect the pedicle screws on the ipsilateral side, and a similar procedure was repeated on the contralateral side. The spinal cord was gently dissected away from the pedicle to expose the posterior longitudinal ligament. The ligament was incised to expose the vertebral body. A wedge osteotomy was performed using an osteotome or piezosurgery. If the remaining anterior portion of the vertebral body was intact, it was completely osteotomized using a piezosurgery. Two short rods were secured on the pedicle screws above and below the osteotomy level. The kyphosis deformity was corrected by closing the osteotomy with sequential rod contouring. During the procedure, normal motor- and sensory-evoked potential of the spinal cord was confirmed using spinal cord monitoring. The final fixation was completed with longer rods. The voids at the osteotomy sites were filled with allogenic bone grafts. The wound was closed in layers. (Figures 4 and 5) (a) This deformity is mainly due to wedge-shaped changes of a single vertebral body, which was defined as a monopteral shape, (b) The red line is the osteotomy design. (c) The area of osteotomy shown after osteotomy. The arrow indicates the expected distance of lamina closure, and (d) After correction of the kyphosis, the central column of the spine is closed and the anterior margin of the vertebra is opened. The arrow indicates the distance of opening. (a) This deformity is mainly due to wedge-shaped changes in the two vertebral bodies and is defined as a bivertebra, (b) The red line is an osteotomy design where the pedicle is preserved as much as possible, (c) The area of bone resection shown after osteotomy. The arrow indicates the expected distance of lamina closure, and (d) After correction of the kyphosis, the central column of the spine is closed and the anterior margin of the vertebra is opened. The arrow indicates the distance of opening. (a) This deformity is caused by four vertebral body deformities, which are defined as multivertebral body type (vertebral body≥3), (b) The red line is the osteotomy design, (c) The area of bone resection shown after osteotomy, the arrow points to the expected lamina closure distance, and (d) After correction of the kyphosis, the central column of the spine is closed and the anterior margin of the vertebra is opened. The arrow indicates the distance of opening. A 6-year-old female patient (height, 112 cm; weight, 21 kg) suffers congenital kyphosis. (a) A photo taken on the back view, (b) Lateral view, (c). Preoperative standing anteroposterior X-ray of full-length spine, (d) Lateral X-ray (SK: 94°, TK: -39°, LL:58°, PI:30°, SVA: 3 mm), (e) Preoperative three-dimensional CT reconstruction shows local kyphosis in the thoracic and lumbar spine, and no evidence of scoliosis, (f) A section view shows the abnormalities of the spine at L1 and 2 with vertebral dysplasia and at T12, L1, 2, 3 with anterior fusion of the four vertebral bodies, (g) Postoperative standing anteroposterior X-ray of full-length spine shows the shoulders are of equal height, no evidence of scoliosis, and nor pelvic tilt, (h) Full-length lateral X-ray (SK, 4°; TK, 0°; LL, -20°; PI, 11°; SVA, 5 mm), (i) Anteroposterior X-ray after 2 years, (j) Lateral X-ray (SK, 7°; TK, 13°; LL, -21°; PI, 16°; SVA, 15 mm), and (k). A photo taken on the back view 2 years after surgery. B. Lateral view photo. According to preoperative, postoperative and reexamination CT scan data, 3D printing rapid prototyping technology was used to visually display the situation of deformity correction and bone healing. (a) L1, 2 vertebral body dysplasia, T12, L1,2,3 anterior edges of the four vertebral bodies fused, (b). After L1 osteotomy via pedicle, bone-to-bone convolution was reached between T12 and L2, (c) The spinal canal was completely closed to ensure the integrity of the spinal canal and provide a strong guarantee for the fusion of the posterior spine, and (d–f) One year after the operation, the bone growth at the opening of the anterior osteotomy of the vertebral body was rechecked for good bone growth. The osteotomy site between T12 and L2 achieved bone healing, and the bone behind the spinal canal also achieved bone healing.




Patients ambulated 5–6 days later and used custom-made thoracolumbar orthoses for 3 months after surgery.
Outcome evaluation
Operative time, blood loss, osteotomy site, fusion segment, osteotomy techniques, and complications were recorded. Radiographic evaluation was performed on standard full-length lateral standing spine radiographs. 19 The parameters included SVA (distance between plumb line C7 and posteriosuperior corner of S1), local kyphosis angle, PI index (infiltration rate). The distance between the anterior margin of the vertebra and the length of the midline closure of the spinal canal was measured using the three-dimensional models. Quality of life was assessed using the Scoliosis Research Society (Scoliosis Research Society) SRS-22 score. SRS-22 questionnaire survey was conducted (some children were completed with the assistance of their parents).
Statistical analysis
SPSS software version 19.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. Data were shown as mean ± standard deviation. The comparison between preoperation and postoperation was performed by paired samples t test. Statistical significance was set at p-value < .05.
Results
There were nine male and six female patients. The average age at surgery was 10 years (range, 3–15 years). In this series, we used single-level (n = 4), double-level (n = 3), and multilevel vertebral (n = 8) osteotomy techniques. The osteotomy segments included T6, T8, T9, and L2 (n = 1); T11 (n = 2); T12 (n = 3); and L1 (n = 6). The average range of fusion was 6.3 segments, including 1 case of four segments, 4 cases of 5 segments, 6 cases of six segments, 2 cases of 7 segments, 1 case of 10 segments, and 1 case of 11 segments.
Clinical demographic and characteristics for 25 patients.

Comparison the radiographic parameters.
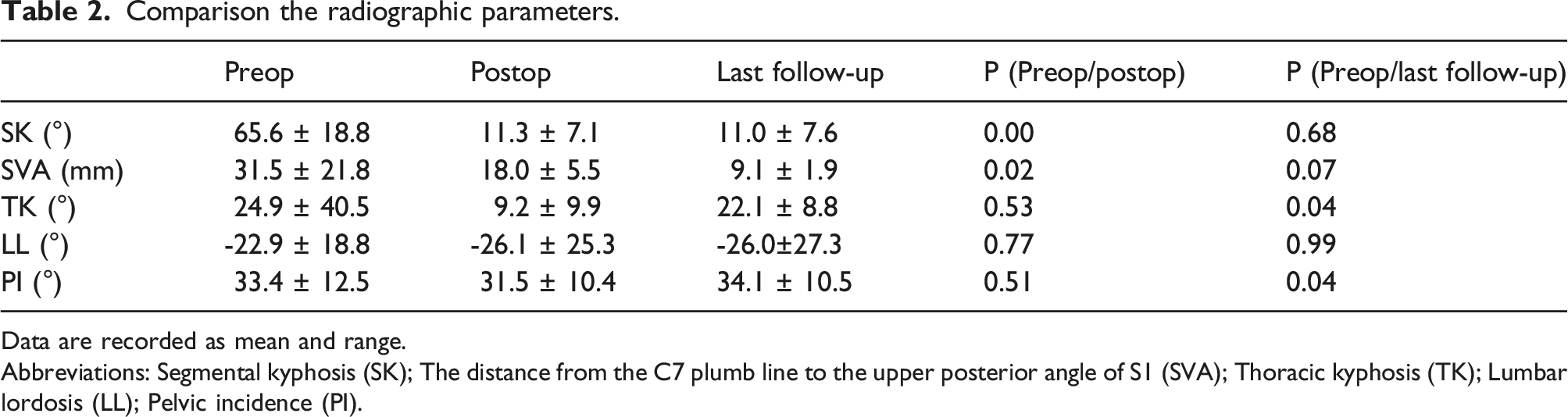
Data are recorded as mean and range.
Abbreviations: Segmental kyphosis (SK); The distance from the C7 plumb line to the upper posterior angle of S1 (SVA); Thoracic kyphosis (TK); Lumbar lordosis (LL); Pelvic incidence (PI).
Different types of anterior vertebral body extension length and lamina closed length after osteotomy.

Quality of life
A total of 12 patients responded to SRS-22 questionnaire at both preoperation and the last follow-up. At preoperation, the mean scores of pain, mental health, selfimage, and function were 3.86 ± 0.60, 3.02 ± 0.61, 2.98 ± 0.44, and 3.58 ± 0.68, respectively. At the last follow-up, the mean scores of pain, mental health, self-image, function, and satisfaction were 4.54 ± 0.62, 3.82 ± 0.46, 3.96 ± 0.52, and 4.17 ± 0.66, 4.8 ± 0.98 m respectively, showing improvements at different levels.
Complications
In this group of cases, postoperative abdominal pain and discomfort occurred in 11 cases, accounting for 73.3% of all cases. B ultrasound examination of the abdomen showed no obvious abnormalities in the abdominal organs and no special treatment was done. The pain was relieved 3–7 days after the operation. It was considered to be caused by postoperative intestinal and abdominal vascular traction.
In one case, the spinal cord monitoring MEP disappeared during the operation, which occurred during the closure of the osteotomy. While the lamina was not completely closed, so we explored the spinal canal through the unclosed lamina space and found the accumulation of adipose tissue in the vertebral joints, compressing the spinal cord. We promptly cleaned up the fat and ligament tissue in the spinal canal, relieved spinal cord compression, and intravenously injected methylprednisolone 80 mg. About half an hour later, the MEP recovered. We continued to correct the lamina and completely closed the lamina. The MEP did not decrease. After the operation, the patient had no symptoms of nerve damage after waking up.
Cerebrospinal fluid leakage occurred in 1 case, which was caused by the traction of the nerve root during the osteotomy process, resulting in tearing of the dural sac and the exit of the nerve root. No repair was done during the operation, the postoperative drainage volume was slightly larger, and the color of the drainage fluid was light red. The drainage tube was pulled out 3 days after the operation, and the wound healed naturally without special treatment.
Discussion
Closing-opening wedge osteotomy to correct angular kyphosis is a surgical technique improved by Norio Kawahara 15 combining the techniques of Smith-Petersen, Heinig and Tomita et al. The characteristics are that firstly, the anterior longitudinal ligament is used as the orthopedic center point to correct the kyphotic deformity to 30–35° using a closed osteotomy, and then an open osteotomy is used to correct the remaining kyphotic deformity with the spinal cord as the orthopedic center point. The open vertebral space is supported by autologous iliac bone or titanium mesh bone graft. Later, this technique is further improved by using PSO osteotomy taking vertebral column as orthopedic center to properly open the anterior edge, and this is called fish-mouth PSO because the opening of the anterior edge of the spine is similar to a fish mouth. Some scholars 17 consider the fish-mouth PSO to be COWO. While, the author of this paper believes that this is not accurate, because only the first type of the classification introduced in this paper can be called fish-mouth PSO, and the second and third types cannot be called PSO osteotomy. To the best of the author’s knowledge, there is no literature report on the use of COWO in the treatment of congenital kyphosis. For the first time, this paper summarizes the different osteotomy positions and methods according to its different types, and the closed length of lamina and the safe opening length of the anterior edge of the vertebral body are accurately measured.
Spiro et al. 20 treated 10 patients (mean age 11 years) with simple kyphosis by posterior osteotomy. Among them, 7 patients with a kyphosis angle less than 60° underwent a standard PSO osteotomy, and three patients with a kyphosis angle greater than or equal to 60° underwent Vertebral Column Resection osteotomy. Zeng et al. 21 treated 23 patients (mean age 27 years) with kyphosis or lateral kyphosis by posterior osteotomy. Among them, nine patients with a kyphosis angle less than 70° underwent PSO osteotomy, and 14 patients with a convex angle greater than or equal to 70° underwent VCR osteotomy. Qiu et al. 22 performed SRS-Schwab4 23,24 closed osteotomy on 38 patients with an average kyphosis angle of 50°. In this group, 9 cases of kyphosis angle were greater than 60°, and 6 cases of kyphosis angle were greater than 70°. COWO may be suitable for the treatment of CK in children, especially moderate to severe congenital kyphosis, which may has significant advantages over the PSO and VCR osteotomy.25,26
If a simple closed osteotomy is used to achieve the same orthopedic effect, it will undoubtedly increase the scope and level of osteotomy (Figure 6). In order to prevent excessive shortening of the spinal cord, a titanium mesh must be implanted, which will increase the difficulty of the operation, surgical time, bleeding volume, postoperative bleeding of flow rate and the incidence of nerve damage that may occur, and may cause symptoms such as the sinking of the titanium mesh and recurrence of deformities. Schematic diagram of closed osteotomy. (a) If a simple closed osteotomy is used, an osteotomy should be performed along the red dotted line if the same osteotomy angle is to be achieved. This resulted in an increased grade of osteotomy and difficulty in placing the pedicle screw indicated by the arrow, (b) In order to achieve effective orthopedics and fixation, it is necessary to extend the range of surgical fusion, as shown by the green screws, and (c) To maintain the vertebrate height, a titanium mesh is placed in the anterior column, which adds more difficulty, risk of iatrogenic injuries, and nonunion by reducing the bone-to-bone contact.
Especially the expanded the range of osteotomy, which destroyed the pedicles at the upper and lower ends of the osteotomy, making the original pedicle screw unable to be inserted. This requires increasing the range of surgical fusion. If the osteotomy is in the lumbar spine, this is particularly unfavorable for the preservation of lumbar segments and the fixed segment even reaches the sacrum, which the lumbar spine cannot be moved at all. Owing to using the preoperative three-dimensional printing models, intraoperative planning can be avoided, which shortens the operative time and reduces blood loss.
Through this group of cases, we did find that SVA gradually decreased from preoperative to postoperative to the last follow-up, and similar situations were also reported in some kyphosis surgical correction literature.8,10 There are two main reasons for this.
The limitations of this study include a retrospective study, a small sample size, and no control group. However, an average of 5 years of follow-up showed encouraging results. As far as we know, this is the first systematic study of closed-open osteotomy to treat congenital kyphosis. However, further research on more patients should be performed to better ascertain the result of treatment.
Conclusion
The present study consisting of a minimum of 2-year postoperative follow-up suggested that the result of the posterior COWO for treatment of congenital kyphosis in children is satisfactory. During the longitudinal follow-up, the patients could achieve solid fusion and the correction could be well maintained.
Footnotes
Authors’ contribution
HLY, XHF, MZS, and LC contributed to the study design. XHF and LC contributed to the data analysis and drafted the manuscript. HLY directed data collection and provided administrative support for the project. All authors contributed to interpretation of the data, commented on the manuscript, revised the manuscript, revised the manuscript, and approved the final version for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project is supported in part by the National Natural Science Foundation of China (Grant number: 81171735), the Provincial Natural Science Foundation of Shaanxi (Grant number: 2017JC2-04) and Air Force Military Medical University.
Ethics approval
Approval was obtained from the Ethics Committee of the First Affiliated Hospital of the Air Force Medical University. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to participate
Informed consent was obtained from all individual participants and their legal guardians included in the study.
Data availability
The data are available from the corresponding author upon reasonable request and with permission from the Xijing Hospital, Air Force Military Medical University.