
Abstract
The concept of antibiotic-coated implants, mainly coated intramedullary nails, has become increasingly used for the treatment of fracture related infections. After a long period of hand-made implants, commercially fabricated implants combine several benefits. Antibiotic-coated nails constitute a solid treatment option for unstable diaphyseal infections with fractures or non-unions. They release high concentrations of antibiotics locally, while retaining reduction and providing axial stability. This review aims to provide an overview about the background, the development, the indications, the treatment strategies and the outcomes of antibiotic-coated intramedullary nails.
The concept of antibiotic-coated implants, mainly coated intramedullary nails, has become increasingly used for the treatment of fracture related infections. After a long period of hand-made implants, commercially fabricated implants combine several benefits. Antibiotic-coated nails constitute a solid treatment option for unstable diaphyseal infections with fractures or non-unions. They release high concentrations of antibiotics locally, while retaining reduction and providing axial stability.
This review aims to provide an overview about the background, the development, the indications, the treatment strategies and the outcomes of antibiotic-coated intramedullary nails.
Background
Despite remarkable advances in the field of orthopedic surgery, fracture related infection (FRI) remains a common and potentially devastating complication after osteosynthesis. 1
A recent epidemiological study from Germany even shows a slight increase in the prevalence of FRI to 10.7 cases per 100,000 inhabitants, resulting in a 1.23% risk for FRI per fracture. 2
Among other initiatives, this has led to a consensus meeting of an international expert group with support from the AO Foundation. This group proposed a new definition for FRI in 2018, which is comprised of suggestive and confirmatory criteria that are based on clinical, radiological and laboratory parameters. 1
This risk for FRI is remarkably higher in open long bone fractures with significant soft tissue damage. This applies especially to fractures of the tibia, due its sparse soft tissue coverage. Tibia fractures are by far the most common open fractures 3 and infection rates may reach up to 43%, depending on the literature. 4
The initial treatment of such fractures aims to prevent infection, preserve soft tissues and establishing stability. While some advocate a staged approach with initial external fixation and temporary coverage by negative pressure wound therapy (NPWT), 5 others promote primary musculocutaneous coverage with internal fixation. 6 A recently published Cochrane review about the treatment of open long bone extremity fractures shows, that there is limited scientific evidence for universally applicable treatment recommendations. 7
Especially grade 3 open fractures often develop acute or chronic infections, which interfere with bone healing and cause non-union or osteomyelitis. 2 Such complications represent a tremendous challenge to treat and require a precise and multifactorial approach, consisting of thorough surgical debridement, restoration of viable soft-tissue coverage, microbiological sampling and targeted local and systemic antibiotic treatments. These measures alone, however, may remain inadequate to eliminate bacterial biofilms and implant removal often becomes inevitable. In such situations, antibiotic coated nails can retain stability and enable the local release of high antibiotic concentrations.
Development
The aim of inserting an antibiotic coated implant has been twofold: On one hand, it is paramount to achieve infection control and to prevent the formation of a new bacterial biofilm. On the other hand, fracture reduction should be retained and axial stability should be provided:
One of the first mentions of a coated intramedullary nail in the literature was in 1998. The authors described a significantly lower risk of osteomyelitis when intramedullary tibia nails were covered in antiseptic solution in a rabbit model. 8
In view of the availability of isolated case reports on antibiotic-loaded cement spacers for the treatment of infected arthroplasties, 9 from the early 2000s there was also an increasing emergence of case reports and animal experiments using antibiotic-loaded cement rods to treat infected long bone fractures. 10 These rods were mostly custom made, as commercially produced implants were not available yet.
One common technique, which is still in use today, is to mix conventional bone cement with antibiotic agents to create custom cylindrical implants within different sized silicone tubes (ie. chest tubes). 11 Other authors report shaping custom implants through a rolling motion or by using custom made molds.
These implants, however, are for temporary use and local application of the medication only. As they are shaped around thin metal cores, such as guidewires, K-wires or Ilizarov-Pins, they come with the disadvantage of reduced stability and limited load bearing capacity. 12 This problem can be addressed by the installation of an additional external fixator or by strict partial load bearing of the affected extremity. Once infection control is achieved, removal of the implant and replacement with a conventional nail is needed. To avoid this, other authors describe coating conventional intramedullary nails with a 1.5–2.5 mm layer of an antibiotic-cement mixture. 13
Commercially fabricated implants
In 2005, De Puy Synthes licensed the first commercially available gentamicin-coated intramedullary tibial-nail, the UTN (Unreamed Tibial Nail) PROtect®. This product was coated with a biodegradable layer of gentamicin-laden polymer. It later evolved into the ETN (Expert Tibial Nail) PROtect®, which allows reamed insertion and more proximal and distal locking options. It offers improved biomechanical properties compared to the custom made options, allows full axial load bearing and does not require additional surgery to be replaced with a definitive implant. These advantages, however, come with a considerable financial costs and a limited global availability. 14
Other, less known providers of fabricated genta- or tobramycin covered intramedullary nails are the French company “Synimed”, the Argentinian company “Subiton” or the Indian Company named “Matrix Meditec”, which lack representation in the literature.
Scientific background
The use of antibiotic coated implants requires the consideration of multiple factors. These include the choice of cement, the choice of antibiotic agent and the mechanical properties of the implant.
In regards to the custom made implants, a consensus on standardized protocols has yet to be reached.
Choice of cement
Regarding the choice of bone cement, there seems to be strong agreement within the literature: A recent systematic review by Ismat et al. found that most authors use polymethylmethacrylate (PMMA) for the creation of antibiotic coated implants. 12 PMMA is a polymer, which is be created by combining two components (a liquid and a powder) in an exothermic reaction. As this reaction can reach up to 80°C, it is essential to combine it with an antibiotic agent with high heat stability. PMMA cement has good elution properties, can be mixed with a range of antibiotic agents and offers structural advantages, which allow good handling and shaping of the implants. One bag of cement powder is commonly mixed with 2–4 g of the antibiotic agent before adding the liquid monomer. The components are then mixed as usual. While a combination of more than one antibiotic agent can be used, it is important to note, that a higher ratio of antibiotics to cement reduces the structural stability of the implant.
Choice of antibiotic agent
The most commonly used antibiotic agent is vancomycin, which is often mixed with another agent like genta- or tobramycin. 12 The rationale behind these choices stems from their favorable coverage profiles (with a special focus on staphylococcus aureus) and good heat stability. 15
Besides the use of antibiotic agents, other experimental studies have investigated the efficacy of nails coated with human β-defensin-2, 16 antimicrobial peptides 17 growth factors 18 or vitamins. 19
Local and systemic antibiotic release
One major advantage of using antibiotic-coated implants is the local release of high doses of the antibiotic agent, without increasing the systemic concentration.
The first peak of local antibiotic release can be seen within the first 24 h after implantation and relevant local concentrations can be upheld for up to 6 weeks. 14 The release into the systemic circulation, however, usually does not exceed detectable levels. 20 These elution properties are even more favorably in commercially available products, which achieve high local release within hours and sustain relevant local levels for approximately 6 months. 21
Indications
The most common indications for antibiotic-coated nails are revision of infected long bone fractures after intramedullary nailing, 22 infected non-unions 23 and osteomyelitis. 11 Other potential uses described in the literature are the fusion of chronically infected ankle fractures 24 or arthrodesis after infected total knee arthroplasties. 25
Another important potential indication is primary fracture fixation in cases at high risk for infection, such as grade 3 open fractures or open fractures with severe contamination:
A recent multi-center cost-effectiveness analysis shows that primary usage of ETN PROtect® in grade 3 open tibia fractures is associated with a lower rate of infection and significant cost savings for all included centers. The higher implant costs were offset by fewer infections, inpatient days and re-operations. 26
Despite these promising outlooks, the use of antibiotic coated implants should not replace proper surgical technique. Therefore, it should always remain the highest priority to perform a thorough surgical debridement, flush sufficiently, perform adequate sampling and use targeted antibiotic therapy. 23
Treatment – strategies and timing
The presence of a fistula or sinus, wound breakdown with exposed bone/implant, purulent discharge, or the presence of pus constitute confirmatory criteria for FRI. If other suggestive signs (redness, fever, elevated inflammatory markers etc.) are present, surgical exploration and extensive deep tissue sampling should be considered.
In case of FRI after intramedullary nailing, reaming and debridement of the intramedullary canal is advisable. In case of infected unstable fractures or non-unions, custom-made antibiotic coated nails or external fixation offer an interim solution to retaining stability.
Recently, a second generation reamer has been developed, which allows for reaming of smaller size canals, provides easier handling and other improvements – it has been named RIA 2. The combination of irrigated reaming with antibiotic coated nails is a promising approach for the prevention and treatment of complicated long bone infections. A recent study from Italy describes successful treatment of 17 non-unions after tibia shaft fractures by combining the RIA system with the ETN- PROtect®. 29
Outcomes
While the literature on antibiotic-coated nails is limited, there have been some studies and case series with overall positive results.21–23,32–40
One of the first published case-series from 2007 showed control of infection in 95% of patients with infected non-unions and segmental bone-defects by using custom made antibiotic rods. 23 Since then, a number of important publications have been released, which cover both commercially available and custom-made antibiotic nails/rods. Interestingly, some authors cover mostly commercially available implants, others appear to exclusively describe the use of custom-made implants. This might be due to the limited availability of the fabricated products on certain markets.
Synopsis of studies on antibiotic coated tibia nails, sorted by year.
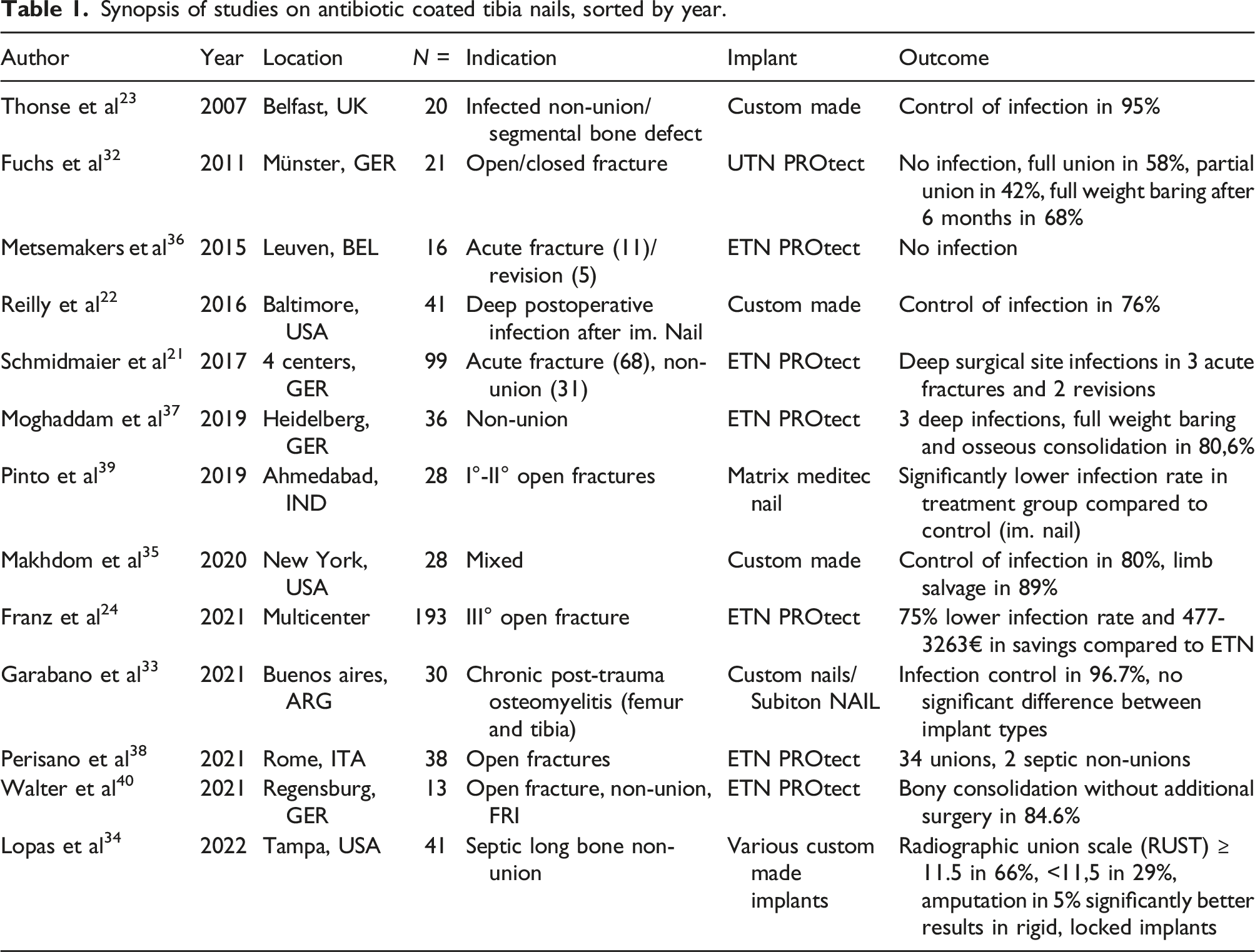
It becomes apparent, that the use of antibiotic coated intramedullary (tibia) nails achieves high rates of infection control and overall good clinical outcomes in complicated cases. These results, however, need to be interpreted in view of their purely retrospective character, and possible publication bias.
Case presentation
The treatment of chronic fracture related infection often requires an individually tailored treatment approach. To exemplify the use of an antibiotic coated nail and the RIA system, we present the case of a 29-year-old male patient with chronic osteomyelitis after open reduction and internal fixation of a comminuted 42B3 tibia fracture.
The patient was hit by a car as a pedestrian in January 2016 and polytraumatized with an ISS of 29. He suffered a blunt chest trauma with a lung laceration and a pneumothorax, a grade 1 (AAST) liver laceration, a grade 3 open C-Type pelvic ring injury, a grade 2 open right femur fracture, and bilateral open lower leg fractures (right side: grade 3; left side: grade 1) (Figure 1(a)). Prior medical history included chronic alcohol and drug abuse. The patient was taken to the OR immediately for damage control orthopedics (Figure 1(b)). The left tibia was openly reduced and internally stabilized on the fourth day using two cerclage wires and a T2 intramedullary nail (Figure 1(c)). Early fracture related infection presented after 2 weeks and was successfully treated with repeated debridement, negative pressure wound therapy and targeted systemic antibiotics. The patient remained asymptomatic and mobile for 2 years but bony union of the left tibia was not achieved. Dynamization was performed in February 2018. In August 2019 (3½ years after trauma), the patient presented with purulent secretion from a fistula above the anterior shinbone and persistent non-union (Figure 1(d)). SPECT confirmed chronic osteomyelitis. Images from a case of non-union and chronic osteomyelitis after a 42B3 fracture of the left tibia treated with the RIA system and an antibiotic coated nail (ETN PROtect®). (a) Initial CT-Scan; (b) External Fixation; (c) Open Reduction Internal Fixation; (d) Non-union and purulent fistula; (e) Nail removal and external fixation; (f) Using the Reamer-Irrigator-Aspirator system; (g) RIA and insertion of ETN PROtect®; (h) X-Ray follow up; J: Nail removal.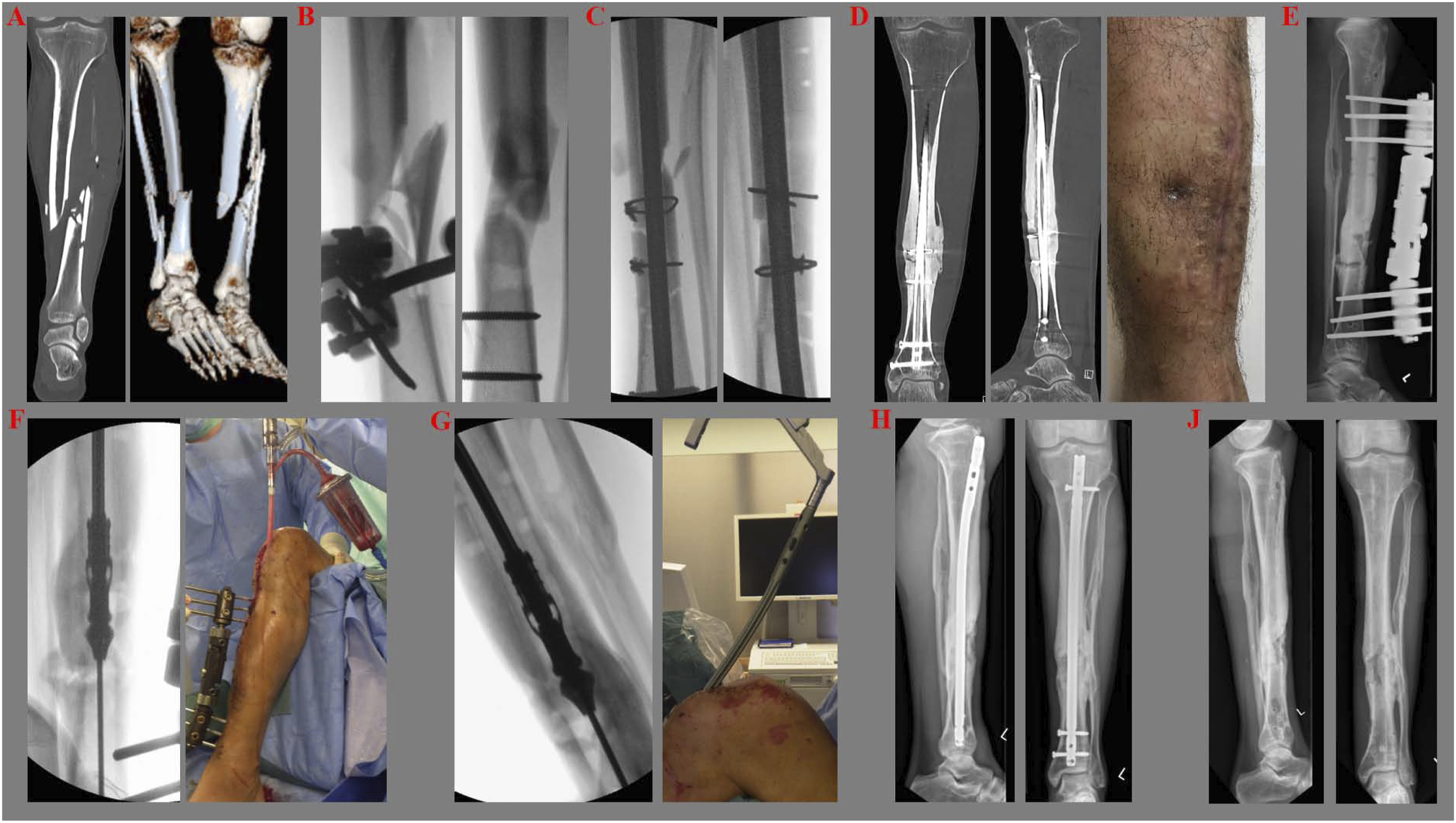
Removal of the nail, thorough debridement and sampling was performed, an external fixator was attached and targeted systemic antibiotic therapy was started (Figure 1(e)). After 1 week, the intramedullary canal was debrided using the RIA system (Figure 1(f)). The external fixator was reattached and systemic antibiotic therapy was continued. After three more weeks the external fixator was removed, reaming with the RIA system was repeated and an ETN PROtect® was inserted (Figure 1(g) and (h)). Infection control was achieved and the patient remained asymptomatic and mobile. The nail was removed in February 2022 Figure 1(j).
Conclusion
Antibiotic coated nails are a valuable adjunct in the treatment of infected fractures and non-unions and might be worth considering in the initial treatment of open fractures with a high risk of infection. High local antibiotic concentrations can be achieved without increasing the systemic levels and adverse effects are seldom. Custom-made and commercially available implants both show a good efficacy, however, custom made implants have lower axial stability and require additional operations. One may find out whether the additional cost of implants and longer time in the operating theaters are compensated by lower rates of infections and whether overall complication rates can be improved.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors received no pharmaceutical or industrial support for this study.