
Abstract
Background:
Ligament reconstruction and tendon interposition (LRTI) is currently the most performed procedure for osteoarthritis (OA) of the thumb carpometacarpal (CMC) joint. In general, satisfactory outcomes are expected, although some patients complain of residual pain after LRTI. The objective of this study is to determine the factors associated with residual pain.
Method:
All patients with OA of the thumb CMC joint who underwent LRTI at our hospital between October 2013 and October 2018 and were regularly observed for at least 1 year were included. The following variables were extracted and included in the univariate analysis: sex, age, dominant hand, pain visual analog scale (VAS) score, Eaton classification, grip strength, pulp pinch strength, and metacarpophalangeal joint hyperextension angle were recorded as variables. Mann-Whitney U test or Fisher exact test was used for univariate analysis of the above factors, and then multivariate logistic regression analysis was performed to find out the factors associated with residual pain.
Results:
The study included 60 thumbs of 53 patients. Eleven thumbs had postoperative residual pain. The surgery on the dominant hand was significantly associated with the presence of postoperative residual pain, especially in males.
Conclusions:
Dominant hand was associated with residual pain after LRTI for OA of the thumb CMC joint, although residual pain was minimal. Our findings will help in preoperative and postoperative counseling of patients. In the future, our results may also help select surgical procedures according to the patient’s characteristics.
Keywords
Introduction
Surgical treatment is commonly performed for osteoarthritis (OA) of the thumb carpometacarpal (CMC) joint that has not responded to conservative treatment. As there are various surgical procedures such as extension osteotomy, trapeziectomy with ligament reconstruction and tendon interposition (LRTI), arthrodesis, and joint replacement, no procedure has been proven to have better results. 1
Among all procedures, LRTI is currently the most performed procedure, as it shows good outcomes in terms of pain and physical function. 2 We also use LRTI as the mainstay of surgical treatment, and as in previous reports, there is generally a significant improvement in postoperative outcomes, although some patients complain of residual pain after LRTI.
Nishimura et al. cited the preoperative pain VAS score at rest as a factor leading to surgery in OA of the thumb CMC joint. 3 It is thought that resting pain is serious enough for patients to choose to undergo surgery.
Although factors associated with postoperative residual pain may be important in counseling patients who choose to undergo surgery in the expectation of improving their intolerable pain, there have been no studies reporting the relationship between postoperative residual pain after LRTI and the patient’s character or preoperative physical and radiographic findings.
In this study, we focused on the group with residual resting pain at 1 year postoperatively after LRTI for OA. The reason for focusing on resting pain is that the group with resting pain is treated as the most severe pain group in previous studies.4,5 Our aim is to determine which patient characters and factors measured preoperatively were associated with the presence of residual pain.
Materials and methods
Our institutional review board approved the study. We performed a single-center, retrospective study in the university hospital located in the city center; all patients with OA who underwent LRTI at our hospital between October 2013 and October 2018 and were regularly observed for at least 1 year were included. All cases were diagnosed as primary non-traumatic OA of the thumb CMC by hand surgeons. Posttraumatic, rheumatic, and severely neuropathic thumbs were excluded from the study. A total of 60 thumbs of 53 patients (17 males [18 thumbs] and 36 females [42 thumbs]) were included in this study.
For all patients, variables were extracted by hand surgeons at the first visit; sex, age, dominant hand, occupation, pain visual analog scale (VAS) score (0 mm = no pain, and 100 mm = worst imaginable pain) at rest, Eaton classification (comparison among stages), grip strength, pulp pinch strength, and metacarpophalangeal (MCP) joint hyperextension angle.
At 1 year postoperatively, patients were assigned into two groups by whether they had residual pain or not.
In terms of radiographic assessment, we also assessed the effect of subsidence of the first metacarpal. We measured the distance between the first metacarpal and the scaphoid and determined the ratio of the distance at 1 year compared to 3 months post-operation.
Statistical methods
Continuous parameters were compared using the Mann-Whitney U test, and categorical variables were compared using the Fisher exact test.
First, the association between the presence of postoperative residual pain and the candidate predictors was evaluated by univariate analysis.
Variables that showed statistical relevance (p < 0.10) were then selected as candidates for independent variables in multiple logistic linear regression analysis.
Multivariate logistic regression analysis was performed with the presence or absence of residual pain as the dependent variable. The respective odds ratios (ORs) were also analyzed; p < 0.05 was considered to indicate statistical significance.
Surgical technique
The surgery performed was the modified LRTI technique using free palmaris longus tendon graft reported by Miura. 6
The first step of the surgery was to resect the trapezium, fix the free palmaris longus tendon to the flexor carpi radialis tendon, and then pass one end of the tendon through the bony hole drilled at base of metacarpal bone and stabilize the first metacarpal by interlacing it with the other end of the tendon. The remainder of the tendon was inserted into the gap. Postoperatively, the first and second metacarpals were temporarily fixed with K-wire for 3.5 weeks.
A short arm thumb spica splint is applied for 3.5 weeks. Active range of motion exercise is encouraged after splint removal. Strengthening exercises including pinch are encouraged after 8 weeks.
Result
Fifty-three patients (60 thumbs) were included in this study. They were all Japanese, and the overall median age was 66 years (range, 43–83 years).
Of those 60 thumbs, 11 thumbs had postoperative residual pain.
The distribution of the pain VAS score at rest is shown in Figure 1. The median preoperative pain VAS score was 23.0 (range, 0.0–90.0; interquartile range, 7.5–56.5), and the median postoperative pain VAS score was 0.0 (range, 0.0–0.0; interquartile range, 0.0–18.0). Preoperative and postoperative distribution of pain visual analog scale (VAS) scores at rest. The box plot shows the minimum, first quartile, median, third quartile, and maximum values.
Results of univariate analysis (residual resting pain).
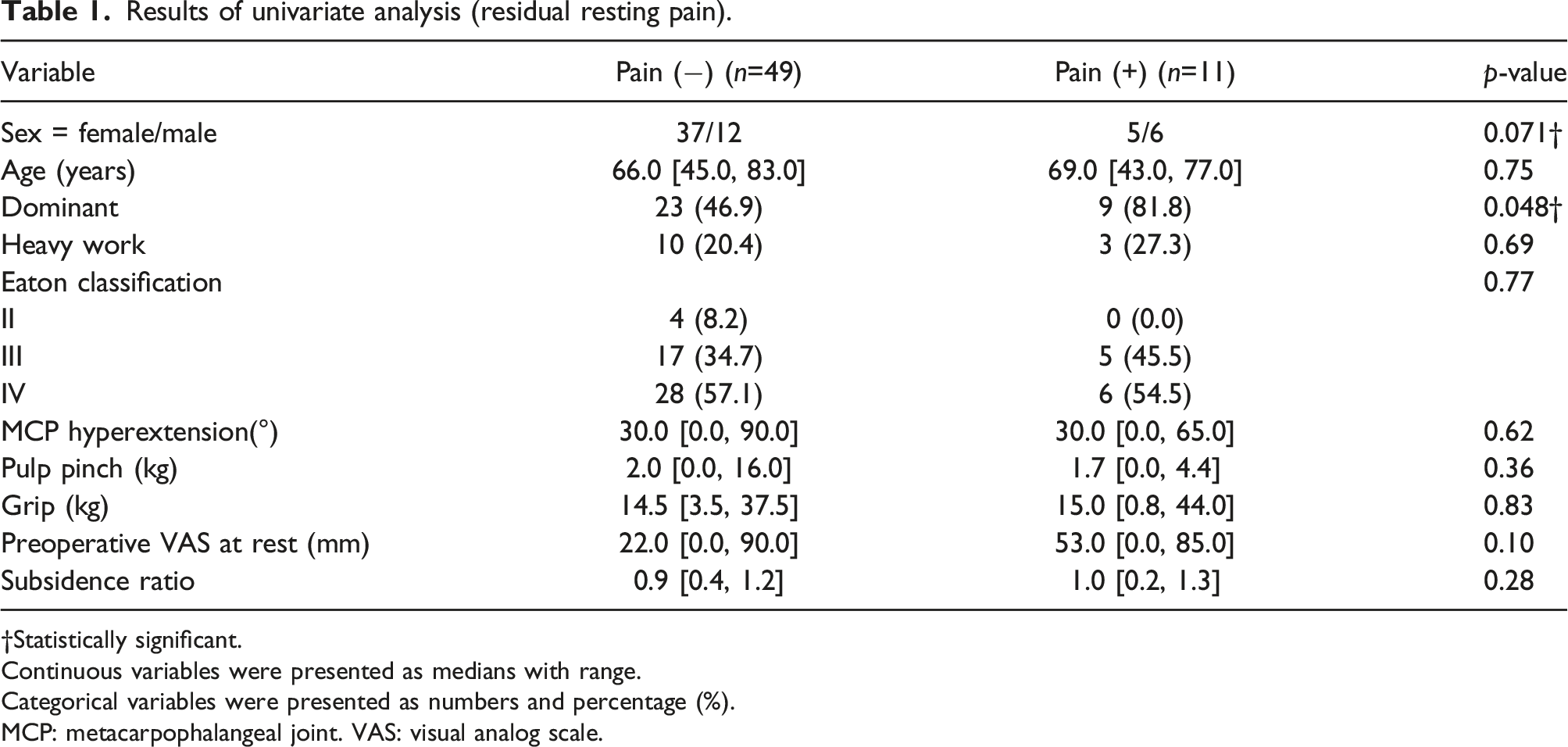
†Statistically significant.
Continuous variables were presented as medians with range.
Categorical variables were presented as numbers and percentage (%).
MCP: metacarpophalangeal joint. VAS: visual analog scale.
Results of univariate analysis in males.
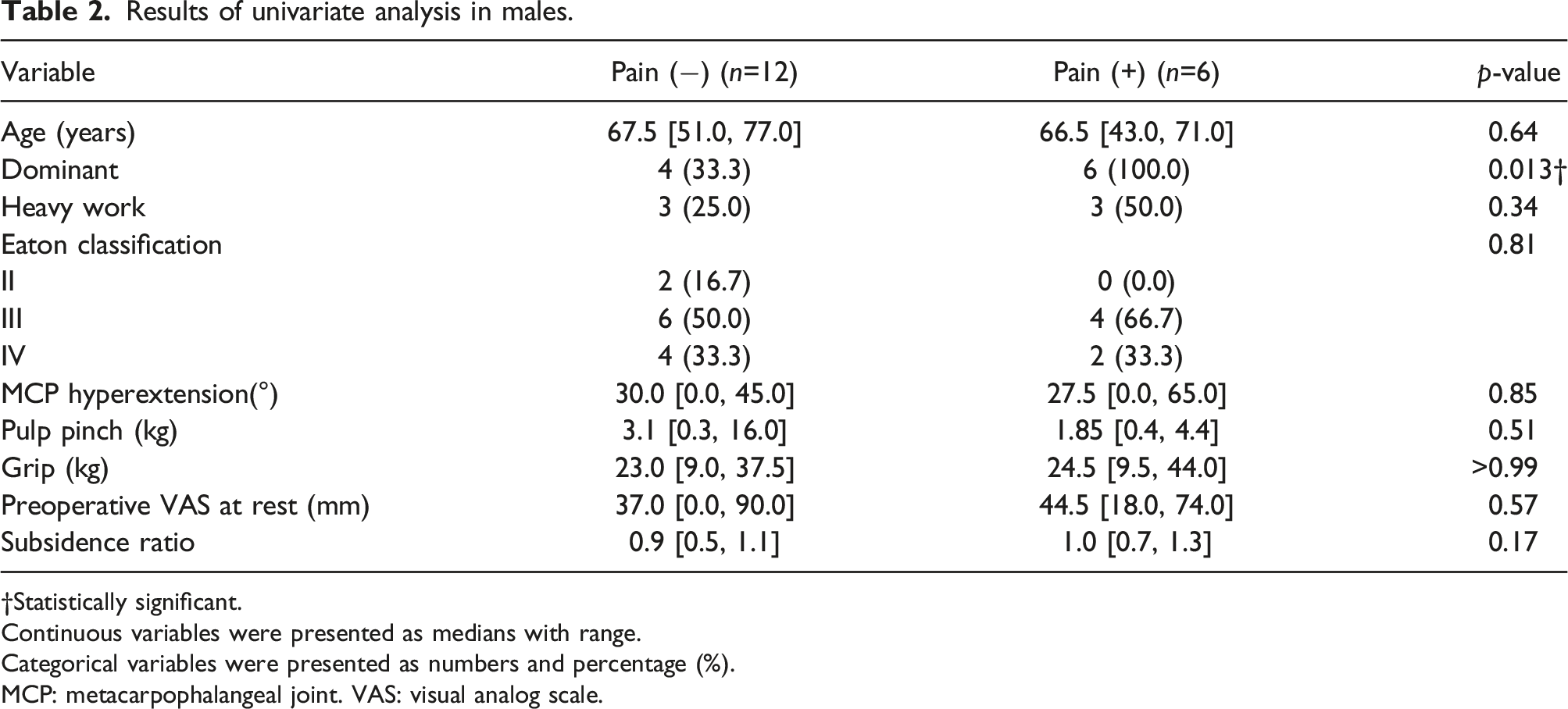
†Statistically significant.
Continuous variables were presented as medians with range.
Categorical variables were presented as numbers and percentage (%).
MCP: metacarpophalangeal joint. VAS: visual analog scale.
Results of univariate analysis in females.
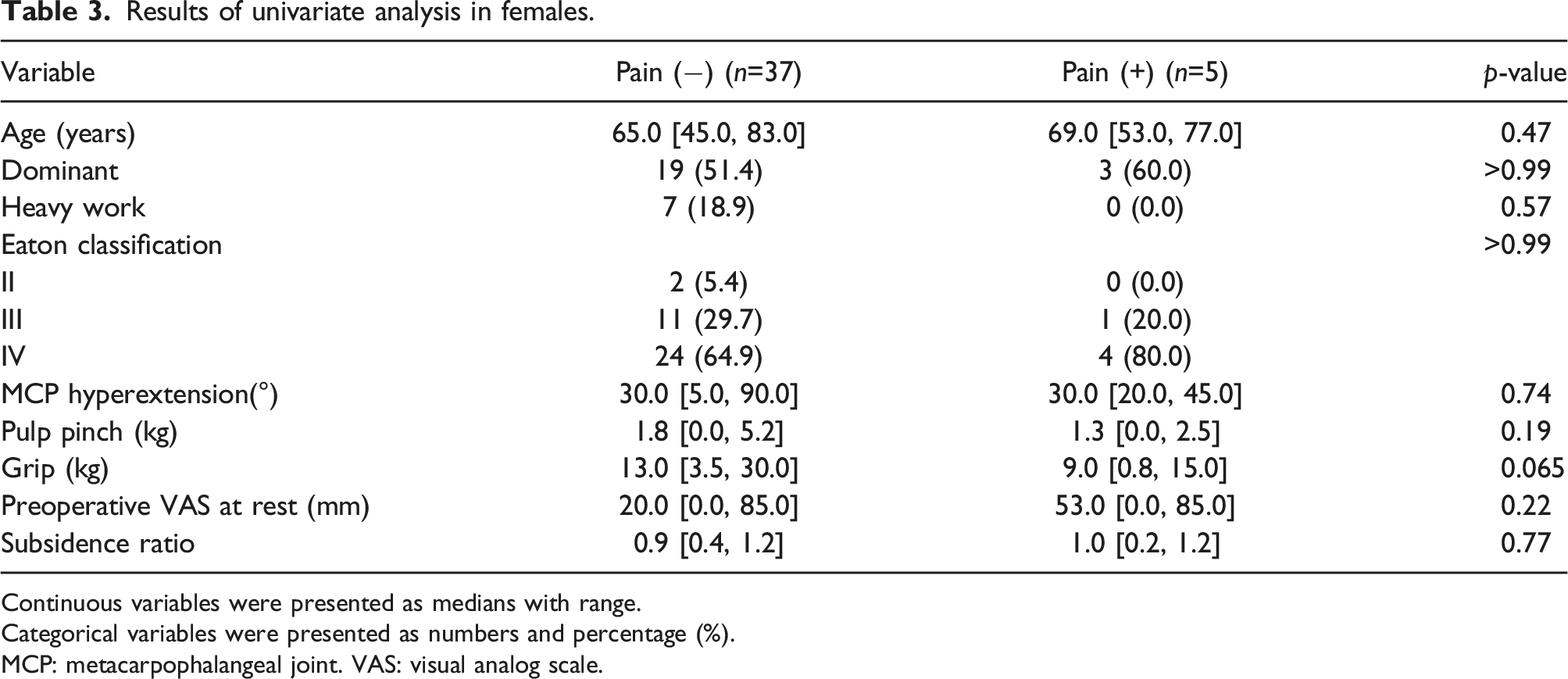
Continuous variables were presented as medians with range.
Categorical variables were presented as numbers and percentage (%).
MCP: metacarpophalangeal joint. VAS: visual analog scale.
Dominant hand was significantly associated with postoperative residual pain only in males, and no such trend was observed in females. In addition, the presence of heavy work was not significantly associated with residual pain in both male and female group.
Results of multivariate logistic regression analysis.

aCI: confidence interval.
†Statistically significant.
Discussion
In this study, we investigated factors associated with postoperative residual pain after LRTI. The surgery on the dominant hand was the factor that showed a significant association.
LRTI, which is now widely adopted for OA of the thumb CMC joint, shows satisfactory improvement in both function and pain, and many reports show continuous improvement up to 1 year postoperatively. 7
Though good long-term outcomes have been also reported, 8 it is important to note that a certain percentage of patients may have residual pain after surgery.
Gangopadhyay et al. reported that 13% of patients had residual pain at 6 years after LRTI, 4 and Salem et al. reported that 18% of patients had residual pain at 6 years after surgery. 5 In our study, 82% of patients had a resting VAS score of 0 mm, meaning the complete resolution of resting pain at 1 year postoperatively, but 18% of patients had residual resting pain. This is comparable to previous studies.4,5
In preoperative counseling, the probability of residual pain after surgery and the characteristics of patients who are prone to residual pain are important information. To date, there have been no studies on factors associated with residual pain. In the present study, the surgery on the dominant hand was significantly associated with the presence of postoperative residual pain. By sex, dominant hand was significantly associated with the presence of postoperative residual pain only in males.
Regarding the difference in sensitivity to pain between dominant and non-dominant hands, several reports have shown that the dominant hand is rather less sensitive to pain.9,10 In addition, Pud et al. performed a sex-specific analysis and found that the dominant hand was less sensitive only in the right-handed male. 11 Considering these reports, there must be a reason that explains our results, in which the dominant hand was more likely to have residual postoperative pain even though the dominant hand is less sensitive to pain. We speculate that the combination of frequency and intensity of use may explain our results. In males, who have stronger muscles than females, the frequency of overload on the dominant hand could increase, and such overload overwhelms the low pain sensitivity of the dominant hand.
There are several limitations to this study. The first is that the number of cases was relatively small, which may have reduced the statistical power of the study. Second, psychological factors such as the Pain Catastrophizing Scale (PCS) were not considered. Catastrophic thinking and depression may have affected the pain sensitivity. 12 Although there was no significant difference in this study, the group with residual pain tended to have a higher preoperative pain VAS score (median 53.0 VS 22.0), which may be influenced by pain perception. Third, we did not consider detailed hand usage. Although the analysis showed no significant association between heavy work and postoperative rest pain even in males, patients who engage in heavy work often complain of pain during use even after surgery, especially with pinching. Information on the actual intensity of use of the surgically operated hand may further clarify whether the intensity of postoperative use had a direct impact on residual pain. Fourth, the pain VAS score is a subjective outcome analysis and cannot be used alone to evaluate postoperative outcomes.
In this study, dominant hand was shown to be associated with the presence of residual pain after LRTI for OA. When analyzed separately by sex, the association was significant only in males. Our findings will help in preoperative and postoperative counseling of patients. In the future, our findings may also help in the selection of surgical procedures according to the patient’s characteristics, such as sex, occupation, and dominant hand.
Conclusion
We investigated the factors associated with residual pain after LRTI for OA of the thumb CMC joint. Dominant hand was associated with residual pain, especially in males. Our findings will help in preoperative and postoperative counseling of patients. In the future, our results may also help select surgical procedures according to the patient’s characteristics.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.