
Abstract
Purpose
To determine whether the addition of lateral extra-articular tenodesis (LET) to anterior cruciate ligament reconstruction (ACLR) reduces rotational laxity of the knee, and to compare the clinical results of this treatment with those of ACLR alone.
Methods
PubMed, Embase, and Cochrane Library were searched by two researchers for clinical studies comparing ACLR with and without LET. Studies with only evidence levels I and II and studies in which anterior lateral ligament reconstruction was performed with grafts were excluded. The risk of bias of the studies was assessed using the Cochrane risk-of-bias and modified Downs & Black tools. The outcomes included (1) functional outcomes; (2) knee laxity measures; (3) knee injury osteoarthritis and outcome score; and (4) complications. The outcomes of the two groups were extracted, summarized and compared.
Results
A total of 234 studies were retrieved and 223 were excluded. Eleven clinical studies with 1745 patients were included in our meta-analysis. Compared to the patients who underwent ACLR alone, the patients who underwent ACLR with LET had reduced pivot-shift (odds ratio [OR] 0.48, 95% confidence interval [CI] 0.31 to 0.74, p = 0.0009), and lower graft failure rate (OR 0.34, 95% CI 0.20 to 0.55, p < 0.0001).
Conclusion
Compared with ACLR only, ACLR combined with LET can effectively reduce rotation laxity of the knee joint, and reduce the graft failure rate in high-risk patients. However, the effects on the function and activity level of patients cannot be confirmed.
Keywords
Introduction
Anterior cruciate ligament (ACL) tears are one of the most common knee injuries accounting for more than 50% of knee injuries and affecting more than 200,000 people in the USA each year. 1 ACL reconstruction (ACLR) is the gold standard treatment for ACL tears according to almost all clinicians. Although surgical techniques for ACLR have constantly been developed and improved over the past few decades, residual rotatory laxity is still a major problem. It can cause knee instability, delay patients’ time to return to sports, and lead to graft failure, and dissatisfaction patients.2–7
Surgeons have long recognized that lateral extra-articular tenodesis (LET) can effectively control knee rotation, 8 so the idea of combining LET and ACLR for the treatment of ACL injury has been proposed to reduce the failure rate of either technique when used alone.9,10 This method began to be performed more often in the 1980s and has been used by many surgeons in various extra-articular reinforcement surgeries such as anterior lateral ligament reconstruction (ALLR).11,12 Compared to ALLR, which requires a graft, LET is more convenient because it usually performed with the iliotibial band to reinforce anterolateral complex and reduce rotational laxity.13–15 Biomechanical and clinical studies have suggested that the addition of LET to ACLR can improve rotational relaxation without increasing the incidence of complications such as osteoarthritis (OA).16,17 However, other studies have shown that the addition of LET to ACLR overly constrains tibial movement, resulting in reduced tibia internal rotation.15,18 In 2017, Devitt et al. 13 reported the results of a meta-analysis involving LET, but in addition to retrospective studies with low levels of evidence, studies on ALLR were also included in the final analysis. Thus, we selected high-level (evidence levels I and II) studies involving LET, to draw a more accurate conclusion on the clinical outcomes of ACLR with the addition of LET.
This study aimed to determine whether the addition of LET to ACLR reduces rotational laxity of the knee and compare the clinical results of this treatment with those of ACLR alone.
Materials and methods
Study selection
The PubMed, Cochrane Library, and EMBASE databases were searched comprehensively according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 19 on 15 December 2020. References from primary and review articles were screened to identify those that met the inclusion criteria. The following search terms were used: (“lateral extra-articular tenodesis” OR “lateral-external joint tenodesis”) AND (“anterior cruciate ligament reconstruction” OR “ACL reconstruction”).
Inclusion and exclusion criteria
This study included all published randomized controlled trials (RCTs) or prospective cohort studies (PCSs) (with evidence levels I and II), on ACLR that included two patient groups: (1) those treated with ACLR alone; and (2) those treated with ACLR combined with LET. All procedures were ligament reconstructions performed for symptomatic acute or chronic ACL injuries, with or without meniscal injuries. Irrelevant articles and studies that failed to meet inclusion criteria, such as reviews, articles on ACLR alone, cadaveric studies, and studies on ACLR combined with ALLR, were excluded. We first reviewed the title and abstract of each article to exclude those that did not meet the requirements. Then the full texts of the rest of the articles were reviewed. Two examiners (JF, JH) conducted an independent review, and any conflicts on article inclusion were resolved by a senior doctor (SW).
Quality assessment
The risk-of-bias of the included studies was independently assessed by 2 examiners. The level of evidence of the included studies was assessed using the Cochrane risk-of-bias and modified Downs & Black tools. 20 In the modified Downs & Black tool, the maximum score is 16. A score ≥12 was defined as indicating high quality; a score 10-11 was defined as indicating moderate quality; and a score ≤9 was defined as indicating low quality.21,22 If there was a disagreement, the two examiners came to a decision by discussion.
Data extraction
The data were extracted by two independent examiners. The outcomes included (1) functional outcomes such as the International Knee Documentation Committee (IKDC) score, Lysholm score, and Tegner activity score; (2) knee laxity measures such as the pivot-shift test, KT-1000, and Lachman test results; (3) knee osteoarthritis and outcome score (KOOS); and (4) complications such as graft failures and pain measured by the visual analog scale (VAS). Data extraction was performed independently, and any conflicts were resolved before final analysis by a professor (SW).
Data synthesis and analysis
A meta-analysis was performed when two or more sets of the same data were reported in the outcomes. We compared the outcomes between the two groups by RevMan v5.4, and p value of less than 0.05 were considered statistically significant. The continuous variables such as the Lysholm score are presented as the mean and standard deviation together with the total number of patients in the ACLR+LET and ACLR-only groups. The results, such as the pivot-shift test results, are presented as a proportion of the number of events to the total number of patients in the ACLR+LET and ACLR-only groups. For the description of the results, the frequency of events or the weighted mean (of continuous endpoint) together with the 95% confidence interval (CI) was calculated. The risk ratio of events for the ACLR+LET and ACLR-only groups and the 95% CI were also calculated according to the Mantel–Haenszel approach. Data heterogeneity was evaluated by using forest plots as well as the Cochran heterogeneity statistic and Higgins I2 coefficient. 23 A Higgins I2 value greater than 50% was considered suggestive of statistical heterogeneity, prompting random effects modeling. Otherwise, a fixed effect model was applied.
Results
Search results
We searched 227 records in the database, and an additional 7 articles were found after we checked the references. A total of 158 articles remained after the duplicates were excluded. After screening of the articles by the titles and abstracts, 63 articles remained, and the full texts were assessed for eligibility. A total of 11 articles2,16,24–32 met all eligibility criteria: randomized controlled trials or prospective cohort studies (evidence levels of I and II), that included studies on ACLR (single-bundle or double-bundle) and two groups: (1) an ACLR-only group; and (2) an ACLR combined with LET group.
A flowchart of the literature search process is provided in Figure 1. There was substantial agreement between the reviewers at the title and abstract screening step (κ = 0.81), and perfect agreement between the reviewers at full-text screening step (κ = 1.00) screening stages. PRISMA (preferred reporting items for systematic reviews and meta-analyses) flow diagram. ACLR, anterior cruciate ligament reconstruction.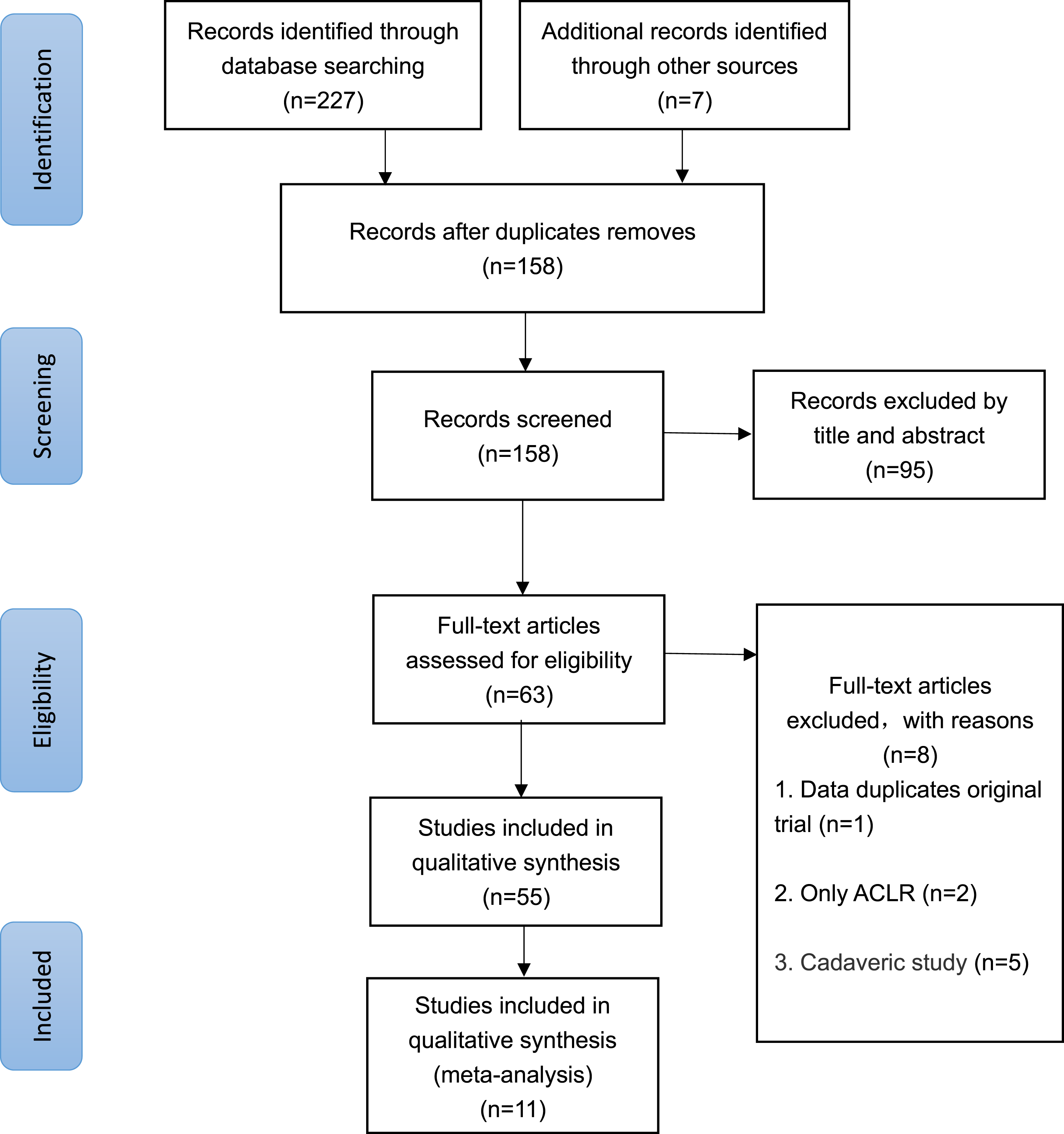
Study characteristics
Study characteristics.

Data for age and follow-up time were presented as mean ± standard deviation or mean or mean (range) unless otherwise indicated. Studies characteristics (LOE, level of evidence; RCT, Randomized controlled trial; ACLR, anterior cruciate ligament reconstruction; LET, lateral extra-articular tenodesis; HA, hamstring autograft; BTB, bone–patellar tendon–bone graft; ITB, iliotibial band; NR, not report).
Methodological quality
Quality assessment tool: Modified downs & black.

Aim, aim of study; Patient, patient characteristics; Sample, sample is representative; Bias, selection bias present; Comparison, comparison group identified; Outcomes, clearly described outcomes; Valid, measures are valid and reliable; Blinding, attempt to blind measurers; Findings, main findings of study; Random, estimates of random variability; Statistics, statistical tests used; Confounders, clearly described distributions of principle cofounders; Adjustment, adequate adjustment for cofounding; Sample calc., reported sample size calculation; Power, sufficient power in study; Quality, ≥12=high quality,10-11=moderate quality,≤9=low quality.
Extracted data.

IKDC, International Knee Documentation Committee; KOOS, Knee injury Osteoarthritis and Outcome Score.
KOOS QOL, KOOS Quality of Life; VAS, visual Analogue Scale; ACLR, anterior cruciate ligament reconstruction; LET, lateral extra-articular tenodesis.
Functional outcomes
Four studies evaluated the Lysholm score in 103 patients treated with ACLR+LET and 201 patients treated with ACLR only. A significant difference was found in the mean Lysholm score in favor of ACLR+LET (mean difference between the ACLR+LET and ACLR-only groups, 3.46; 95% CI 2.39–4.53; p < 0.00001) (Figure 2). Meta-analysis using fixed-effects model to compare the Lysholm score of anterior cruciate ligament reconstruction (ACLR) with lateral extra-articular tenodesis (LET) versus ACLR only for all studies.
Three studies evaluated the Tegner activity score in 95 patients treated with ACLR+LET and 193 patients treated with ACLR only. A significant difference was found in the mean Tegner activity score in favor of ACLR+LET (mean difference between ACLR+LET and ACLR-only groups, 0.80; 95% CI 0.59–1.01; p < 0.00001) (Figure 3). Four studies evaluated the IKDC subjective score in 381 patients treated with ACLR+LET and 407 patients treated with ACLR only. No significant difference was found between the two groups (mean difference between ACLR+LET and ACLR-only groups, 1.90; 95% CI -0.17 to 3.97; n.s.) (Appendix Figure 2). Meta-analysis using fixed-effects model to compare the Tegner activity score of anterior cruciate ligament reconstruction (ACLR) with lateral extra-articular tenodesis (LET) versus ACLR only for all studies.
Knee laxity
Six studies evaluated the pivot-shift test results in 204 patients treated with ACLR+LET and 279 patients treated with ACLR only. A significant difference was found in the rate of positive pivot shift test results in favor of ACLR+LET (risk ratio for ACLR+LET vs ACLR-only group, 0.48; 95% CI 0.31–0.74; p = 0.0009) (Figure 4). Meta-analysis using fixed-effects model to compare the pivot-shift test of anterior cruciate ligament reconstruction (ACLR) with lateral extra-articular tenodesis (LET) versus ACLR only for all studies.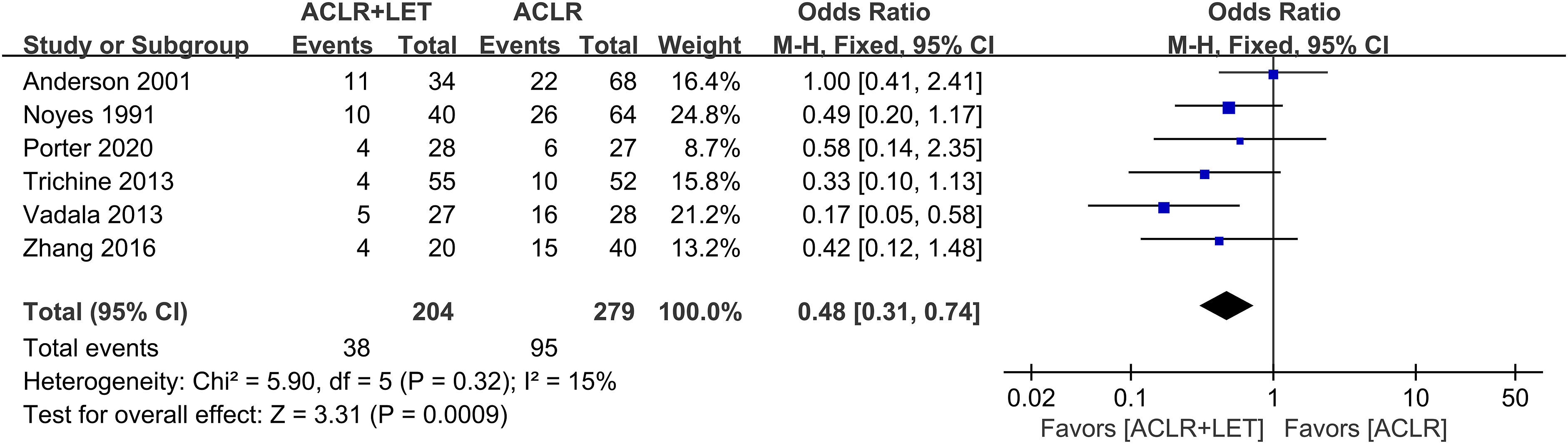
Three studies evaluated side-to-side KT-1000 in 106 patients treated with ACLR+LET and 184 patients treated with ACLR only. No significant difference was demonstrated in the rate of side-to-side KT-1000 values >3 mm (risk ratio for ACLR+LET vs ACLR-only group, 0.70; 95% CI 0.43–1.14; n.s.) (Appendix Figure 3)
Two studies evaluated the Lachman test results in 47 patients treated with ACLR+LET and 68 patients treated with ACLR only. No significant difference was demonstrated in the rate of positive Lachman soft point test results (risk ratio for ACLR+LET vs ACLR-only group, 1.06; 95% CI 0.48–2.35; n.s.) (Appendix Figure 4)
Knee osteoarthritis and outcome score
Three studies provided the KOOS recreation subscore in 342 patients treated with ACLR+LET and 347 patients treated with ACLR only. No significant difference was found between the two groups in this score (mean difference between ACLR+LET and ACLR-only groups, 1.39; 95% CI -1.99 to 4.77; n.s.) (Appendix Figure 5).
Two studies evaluated quality of life with the KOOS (KOOS QOL score) in 334 patients treated with ACLR+LET and 339 patients treated with ACLR only. No significant difference was found between the two groups (mean difference between ACLR+LET and ACLR-only groups, 1.51; 95% CI -0.97 to 4.00; n.s.) (Appendix Figure 6).
Complications of graft failure
Five studies evaluated graft failures in 583 patients treated with ACLR+LET and 695 patients treated with ACLR only. A significant difference was found in the rate of graft failure in favor of ACLR+LET (risk ratio for ACLR+LET vs ACLR-only group, 0.34; 95% CI 0.20–0.55; p < 0.0001) (Figure 5). Meta-analysis using fixed-effects model to showing risk ratio of graft failures for anterior cruciate ligament reconstruction (ACLR) with lateral extra-articular tenodesis (LET) versus ACLR only for all studies.
Visual analog scale
Two studies evaluated the VAS score in 35 patients treated with ACLR+LET and 36 patients treated with ACLR only. No significant difference was demonstrated in the rate of high VAS scores (risk ratio for ACLR+LET vs ACLR-only group, 0.05; 95% CI -0.36–0.47; n.s.) (Appendix Figure 7)
Discussion
The most important finding of the high-evidence-level study was that ACLR combined with LET could reduce the rate of positive pivot-shift test results. The analysis of comparable clinical studies demonstrates that the patients treated with ACLR+LET have fewer positive pivot-shift test results and graft failures. The results showed better patient-reported functional outcomes (the Lysholm score, Tegner activity score) with the ACLR+LET treatment than with ACLR only.
Whether ACLR should be performed with or without LET surgery has been debated for years. Six studies were conducted in the US in the 1980s and early 1990s, but none have been published since then and have only been reviewed in recent years. The termination of LET may have been prompted by an article published by a leading US institution claiming that the procedure was unnecessary, particularly in acute settings. It could be potentially harmful,27,33,34 but recently, biomechanical and clinical studies have suggested that the addition of LET to ACLR can improve rotational stability. 35 The meta-analysis showed that additional LET effectively reduced rotational laxity of the knee, which is consistent with the results of two previous systematic reviews.13,36 Both studies concluded that the addition of LET in ACLR was effective in reducing the rate of positive pivot-shift test results, especially severe preoperative pivot-shift test results. However, there are still problems to consider. Katakura et al. 37 reported in their study that injury to the lateral meniscus leads to increased rotational relaxation of the knee joint and Hoshino et al. 38 also reported the same result. Moreover, Sekiguchi et al. 39 showed that enlargement of the posterior slope can increase the degrees of internal and external rotation of the tibia. All of the above factors may result in a positive pivot-shift test result.
Among the 11 articles included in the meta-analysis, four articles included preoperative data of meniscal injury.2,25,26,30 The meta-analysis revealed the lack of a significant difference in the integrity of the menisci between the ACLR group and the ACLR+LET group (Appendix Figures 8-10). In addition, two other articles28,32 have excluded meniscus injury in their selection of articles. And five articles2,28,30–32 have excluded multiple ligament injuries such as medial collateral ligament (MCL) and lateral collateral ligament (LCL) in their subject selection. Moreover, Gibbs et al. 26 explicitly mentioned the lack of a significant difference in MCL and LCL injuries among all groups. Porter et al. 28 did not find a significant difference in the posterior tibial slope (PTS) data between the two groups. However, Noyes et al. 27 reported four patients in the ACLR group who underwent proximal tibial osteotomy, but none in the ACLR+LET group, which may lead to differences in the PTS between the two groups and affect rotation. However, only a few articles mentioned preoperative data on meniscal and ligament injuries. Meanwhile, posterior lateral complex and other factors that may affect the rotation were not mentioned in any article.
Although the pivot-shift test is considered to be one of the most sensitive methods for diagnosing ACL damage, it is still subjective and variability between examiners has been found in previous studies. 40 Although attempts to use such measurements with mechanical and optical tracking devices hold great promise, the pivot-shift test remains the most widely used method for evaluating rotational stability.41,42 Overall, all studies included in this study used the pivot-shift test to compare ACLR with or without LET. The fixed angle of the iliotibial band may affect the pivot-shift level, but some of the 11 studies included did not list these details, so further analysis of this variable was not performed.
Another issue associated with LET is the possibility of excessive restriction of tibial movement, which can result in reduced knee activity and poorer subjective functional outcomes.15,18 No evidence of statistical significance was found in the results of this study suggesting this complication of LET occurs, in contrast, the addition of LET to ACLR may improve patients’ subjective functional outcomes (the Lysholm score, Tegner activity score). The difference in the Lysholm score in this study was 3.46 (mean difference between ACLR+LET and ACLR-only groups, 95% CI 2.39–4.53; p < 0.00001), but Nwachukw et al. noted in their clinical study that a difference of more than 10 ± 4.3 in the Lysholm score is clinically significant, 43 so the difference is statistically significant but not clinically significant. Moreover, Natalie et al. 44 mentioned in their review that the Tegner activity scale may be more suitable for the comparison of patients at different periods but not suitable for comparison between groups. Therefore, the effect of LET on patients’ subjective functional outcomes is still unclear.
Overall, ACLR+LET significantly reduced the percentage of patients with ACL graft rupture, according to five studies. High-risk populations have been considered to have high graft failure rates in previous clinical studies, 6 which is reflected in this study. Alan et al.24,25 selected patients with high pivot-shift values or high exercise requirements, as did Rowan et al. 29 The inclusion criteria of the studies that reported graft failure events are shown in appendix Table 1. These patients have a higher risk of graft rupture than does the general population, so the graft failure results obtained in this study can only reflect the situation of high-risk populations (who have severe pivot-shift results, a desire to return to high-risk/pivoting sports, and generalized ligamentous laxity), and are not generalizable to all populations.
This study has some limitations. First, it should be noted that only 4 of the 11 included studies in this meta-analysis were RCTs. Therefore, additional high-level studies are needed to obtain a more accurate conclusion and clinical plan for additional LET surgery. Differences in the ACLR surgical method, implant selected, outcomes measured, and follow-up time may also contribute to biases. Second, there was heterogeneity in characteristics of the patient population included in the study, such as their exercise ability and presence of acute or chronic injuries, which may have affected the results of our analysis, as patients with different preinjury activity levels and time to surgery from injury exhibit different postoperative clinical outcomes. Third, because the presence of concomitant cartilage injuries and differences in the surgical methods were not adequately accounted for in each of the included studies, these potential confounding factors may have influenced on the final results. Fourth, some of our data, such as the Lachman test and VAS scores, had a small sample size for meta-analysis, which may have certain limitations. In addition, this meta-analysis only included English articles published electronically, which can lead to publication bias.
Conclusion
ACLR combined with LET can effectively reduce rotation laxity of the knee joint and reduce the graft failure rate in high-risk patients. However, the effects on the function and activity level of patients cannot be confirmed.
Supplemental Material
Supplemental Material - Anterior cruciate ligament reconstruction with lateral extra-articular tenodesis reduces knee rotation laxity and graft failure rate: A systematic review and meta-analysis
Supplemental Material for Anterior cruciate ligament reconstruction with lateral extra-articular tenodesis reduces knee rotation laxity and graft failure rate: A systematic review and meta-analysis by Jing Feng, Yangbo Cao, Lingjie Tan, Jiehui Liang, Chunrong He, Jinshen He and Song Wu in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
In this study, all data statistics analyses were performed under the guidance of biostatistician Prof. Dianzhong Zhang.
Author contributions
Conception or design of the work: JF, JSH, and SW. Analysis or interpretation of data: JF, JSH, YBC, LJT, JHL and CRH. Revised the manuscript critically for important intellectual content: JF, JSH, and SW.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported by National Science Foundation of China (81802208).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.