
Abstract
Purpose
This study aims to identify predictors of postoperative pain and opioid consumption after shoulder surgery to help optimize postoperative pain protocols.
Study Design
Observational cohort study.
Methods
One thirty-four patients undergoing arthroscopic shoulder repair were included. Variables related to the patient, surgery and anesthesia were collected and correlated with postoperative pain intensity, analgesic consumption, and functionality up to 1-month post-surgery. We used mixed-effect linear models to estimate the association of gender, interscalene block (ISB), preoperative shoulder pain, non-steroidal anti-inflammatory drugs (NSAIDs) consumption before surgery, and type of surgery with each of the following outcomes: postoperative pain scores, opioid consumption, and functionality. We further analyzed the data for pain scores and opioid consumption per body weight using the multiple linear regression analysis to demonstrate the aforementioned associations specifically at 1 h, 6 h, 12 h, 24 h, 72 h, 1 week and 1 month after surgery.
Results
Omitting the ISB was associated with higher postoperative pain and cumulative opioid consumption over the first 24 h after surgery. Rotator cuff repair and stabilization surgeries were found to be predictive of higher postoperative pain at 24 h, 72 h, and 1 week and lower functionality at 1 week after surgery. Preoperative shoulder pain and NSAIDs consumption were also predictive of postoperative pain and cumulative opioid consumption.
Conclusion
Omitting a single shot ISB is a strong predictor of postoperative pain and opioid consumption in the early postoperative phase, beyond which the type of surgery, particularly rotator cuff repair and stabilization surgery, emerges as the most important predictor of postoperative pain and functionality.
Introduction
Initial analgesic requirements after minimally invasive shoulder surgery are often similar to those following open surgery, with a third of patients reporting severe pain on the first postoperative day. 1 Suboptimal treatment of pain after shoulder surgery may negatively impact patient outcomes due to delayed post-surgical rehabilitation, 2 risk of transition to chronic pain 3 and increased use or abuse of opioids. 4 Pain intensity may however differ according to the surgical approach, the type of surgery, the anesthetic technique used, as well as the initial shoulder injury and the severity of preoperative pain. Patient factors such as gender, age and level of anxiety may also impact the severity of post-surgical pain.5–7
In this observational cohort study, we hypothesized that the patient’s baseline characteristics, type of surgery, and omission of regional anesthesia may be associated with postoperative pain intensity, opioid consumption, and functionality in patients undergoing arthroscopic shoulder surgery in the immediate postoperative period and up to 1 month following surgery. The identification of these predictors would help guide the clinician in choosing the optimal pain control strategy following shoulder surgery.
Materials and methods
This prospective observational study was approved by the Institutional Review Board and adheres to the applicable STROBE guidelines. After obtaining written informed consent, 146 adult patients were included in the study from August 2018 through March 2020. Inclusion criteria were all adult patients aged greater than 18 years and scheduled for elective arthroscopic shoulder surgery of all types (rotator cuff repair, subacromial decompression/partial distal claviculectomy, stabilization/labral repair, and biceps tenodesis). Patients with a previous or current history of opioid addiction or drug abuse were excluded from the study.
Patient-related factors
Patient-related factors collected included the following: gender, age, body mass index (BMI), American Society of Anesthesiology (ASA) score, active or sedentary lifestyle, smoking status, medical comorbidities, preoperative anxiety on a numerical rating scale (NRS) from 0 to 10, where 0 is absence of anxiety and 10 is being extremely anxious. 8
Anesthesia-related factors
All patients received general anesthesia (GA) with propofol, fentanyl, rocuronium, nitrous oxide, and sevoflurane. The performance of an ultrasound-guided single shot interscalene block (ISB) with 20 mL of a 1:1 mixture of 10 mL bupivacaine 0.5% and 10 mL of lidocaine 2% with 5 µg/mL of epinephrine was left at the discretion of the surgeon and the anesthesiologist. Reasons for not performing ISB were patient’s refusal, surgeon’s refusal (i.e., time constraints), decreased respiratory reserve because of potential phrenic nerve block, and coagulopathy. Patients' pain was managed according to a multi-modal postoperative pain management protocol.
Surgery-related factors
Shoulder surgery type was classified into the following 4 categories: rotator cuff repair, subacromial decompression/partial distal claviculectomy, stabilization/labral repair, and biceps tenodesis. Patients were further classified as having traumatic versus non-traumatic shoulder injury. Presence or absence of preoperative shoulder pain and its intensity was recorded, as well as preoperative use of pain medications, such as non-steroidal anti-inflammatory drugs (NSAIDs).
Postoperative outcomes
The in-patient postoperative pain management protocol included intravenous paracetamol 1g every 6 h as a standing order, NSAIDs, codeine and tramadol 50 mg every 8 h as needed and increments of intravenous morphine for severe pain. Postoperative pain scores were measured using the NRS with scores ranging from 0 to 10 were 0 is no pain and 10 is the worst imaginable pain. NRS was also used to measure satisfaction with pain control, where 0 is not satisfied and 10 is extremely satisfied. Assessments were conducted at regular intervals; in the post-anesthesia care unit (PACU), at 1, 6, 12, 24, and 72 h and 1 week post-surgery by personal interview for in-patients and phone calls post discharge. Time to first analgesic request after surgery and analgesic consumption up to 1 week after surgery were also documented. Patients were discharged home on paracetamol, NSAIDs, codeine or tramadol PRN. The total amount of opioids consumed was calculated as morphine equivalents using the following formula: for codeine, each 1 mg is equivalent to 0.15 mg of morphine; for tramadol, each 1 mg is equivalent to 0.1 mg of morphine.
The shortened disabilities of the arm, shoulder and hand questionnaire (QuickDASH) was used to evaluate functionality of patients postoperatively at 1 week and 1 month after surgery, knowing that the higher the QuickDASH score, the poorer the functionality. 9 Although both the QuickDASH and the American Shoulder and Elbow Surgeons Standardized Shoulder Assessment (ASES) tools have been validated in Arabic, 10 we chose to use the QuickDASH tool as there has been more experience using it in Arabic in our institution and in the region.
Statistical analysis
Descriptive statistics were calculated for all variables, where means and standard deviations (SD) were reported for continuous variables and numbers and percentages for categorical ones. Associations between each of the different predictors and outcome variables were carried out by univariate linear regressions. The choice to investigate these variables was based on prior knowledge and the predictors that showed associations in the sample were then further investigated in adjusted analyses and yielded a model with 5 predictors.
Mixed model analysis was used to examine the relationship between predictive factors − where variables controlled for were those found to be statistically significant or of clinical significance − and outcome variables. These models allowed to investigate overall associations with the outcomes over time, accounting for the repeated measures of the outcome. Multivariable linear regression was further used in order to assess the association of surgery types with each of the outcomes at specific time points.
The time to first analgesic request in those who received ISB versus those who did not was analyzed as a secondary outcome using the log-rank test. Other secondary outcomes such as functionality scores, as well as incidence of severe pain and opioid use at 1 month between patients who received ISB and those who did not were also compared using t-test for means ± SD and chi square for numbers and percentages. Loss to follow-up were excluded from the analysis of the secondary outcomes. Data were analyzed using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) software (version 26). The clinical significance threshold was set at 0.05.
Sample size calculation
With an observed regression coefficient (R2) of 0.12 for multiple regression model including five independent predictors at alpha level of 0.05 and a statistical power of 0.8, a sample size of 100 patients was calculated. 11 To account for a 20% drop out, and to secure enough cases in the different surgical subgroups, it was decided to enroll 150 patients.
Results
Out of 152 patients assessed for eligibility, 6 patients declined to participate. Therefore, a total of 146 patients were included in the study. Of these, 8 patients were excluded because they underwent open shoulder surgeries, and 4 were removed from the analysis due to loss to follow-up (Figure 1). The remaining 134 patients were included and analyzed. Baseline characteristics of all patients are reported in Table 1. All patients underwent one of the 4 surgical categories using an arthroscopic approach by HB and MAT. Of the 134 patients, 27.6% presented with traumatic tears. Overall, 52% of the patients received ISB in addition to GA, while 48% received GA only (Table 1). Outcome variables are presented in Table 2. Univariate analysis, performed to identify most relevant predictors, is depicted in the supplementary file (supplementary tables 1 and 2). Flowchart indicating patients' enrollment in the study. Patient, surgery, and anesthesia-related variables. Data are presented as n (%) or means ± SD. BMI=body mass index, ASA=American Society of Anesthesiology, NRS=numerical rating scale, NSAIDs: non-steroidal anti-inflammatory drugs, GA=general anesthesia, ISB=interscalene block. Outcome variables. Data are presented as means ± SD. NRS=numerical rating scale, PACU=post-anesthesia care unit, QuickDASH=shortened disabilities of the arm, shoulder, and hand questionnaire.


Predictors of pain, opioid consumption, and functionality after surgery
Mixed model analysis identified GA without ISB, preoperative shoulder pain, and preoperative NSAIDs consumption as significant independent predictors of overall pain after surgery. Pain scores increased with time as depicted in Figure 2; the significant results of our mixed model analysis confirm this pain increasing pattern after surgery. The mixed model’s results for pain scores are presented in Table 3. Pain scores after surgery over time. Pain was significantly higher after 24 h (p < 0.05), 72 h (p < 0.001), and 1 week (p < 0.001) compared to 1 h after surgery. Mixed model analysis for pain scores after surgery. PACU=post-anesthesia care unit, ISB=interscalene block, NSAIDs=non-steroidal anti-inflammatory drugs.

Mixed model analysis showed that stabilization surgery as compared to decompressive surgery was a statistically significant predictor of pain. Rotator cuff repair and tenodesis, showed a trend toward significance as predictors of pain after shoulder arthroscopy. To identify the type of surgeries predicting the outcome at specific time points, we performed a subsequent multiple linear regression that is depicted in the supplementary file (supplementary table 3). It indicated that omitting ISB was a strong predictor of pain during the first 24 h, beyond which rotator cuff repair and stabilization emerged as significant predictors of pain at 24 and 72 h after surgery.
Mixed model analysis for cumulative opioid consumption per body weight after surgery.
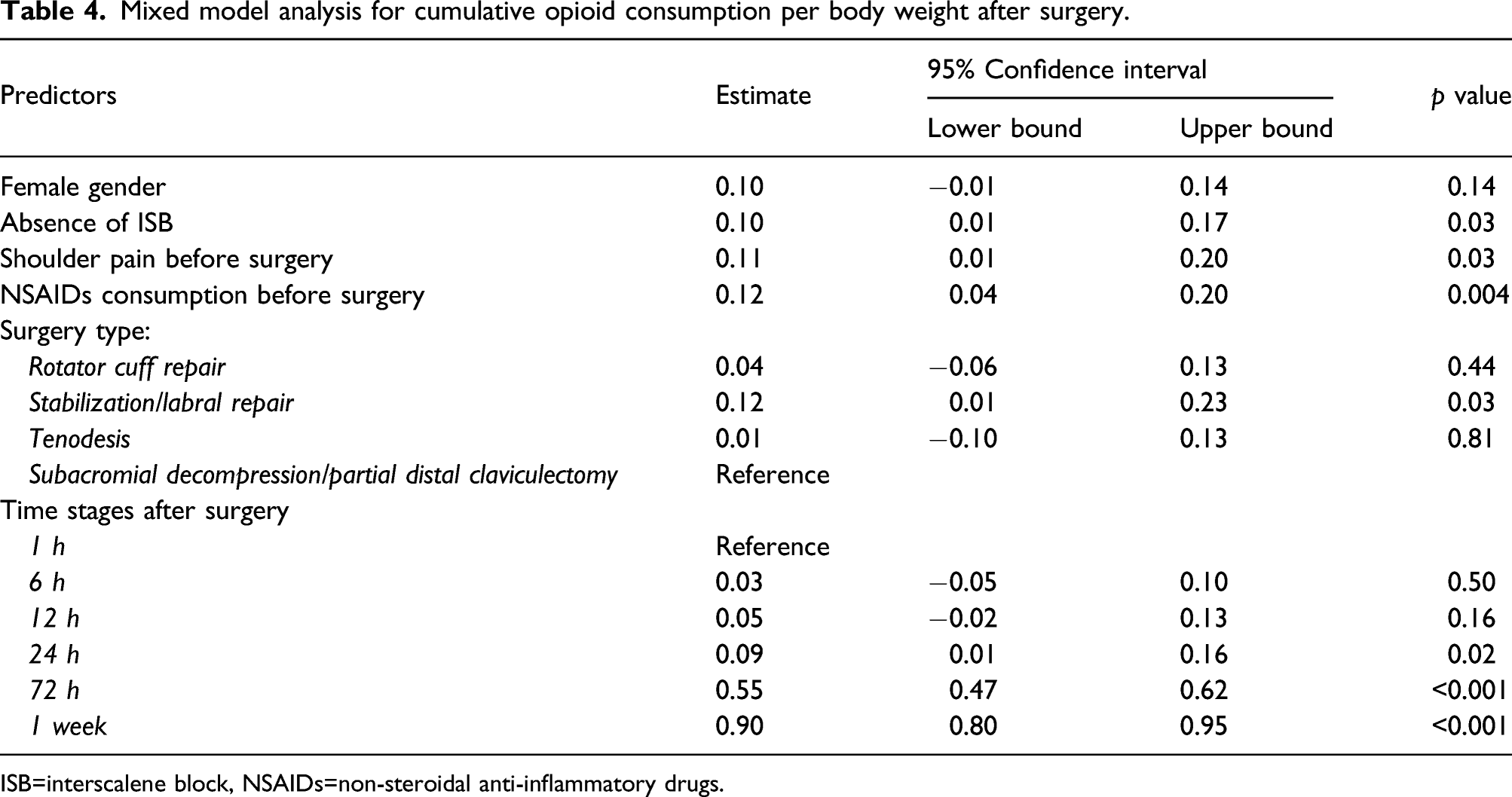
ISB=interscalene block, NSAIDs=non-steroidal anti-inflammatory drugs.
Mixed model analysis for functionality scores after surgery.

ISB=interscalene block, NSAIDs=non-steroidal anti-inflammatory drugs.
Secondary outcomes
Throughout the study follow-up period, severe pain (described as at least one reported pain score greater or equal to 7) was reported by 59% of all patients. However, it was shown to be reported significantly more frequently in patients who did not receive ISB versus those who did (83% vs. 37%, respectively, p<0.001). A survival function (Kaplan Meier curve) was plotted (Figure 3) and showed that patients who underwent GA with ISB had a median time to first analgesic request of 24 h (95% CI, 7.15 to 40.85 h) after surgery. This was longer than the group who did not receive ISB, which had a median time to first analgesic request of 0.16 h (95% CI, 0.15 to 0.17 h) after surgery. The survival distributions for the two groups were significantly different (p < 0.001, log-rank test). Time to first analgesic request after shoulder arthroscopic surgery. Patients who underwent GA with ISB had a longer time to first analgesic request (median=24 h, 95% CI, 7.15 to 40.85 h) than the group who did not receive ISB, (median=0.16 h, 95% CI, 0.15 to 0.17 h) after surgery. The survival distributions for the two groups were significantly different (p < 0.001, log-rank test). GA, general anesthesia; ISB, interscalene block.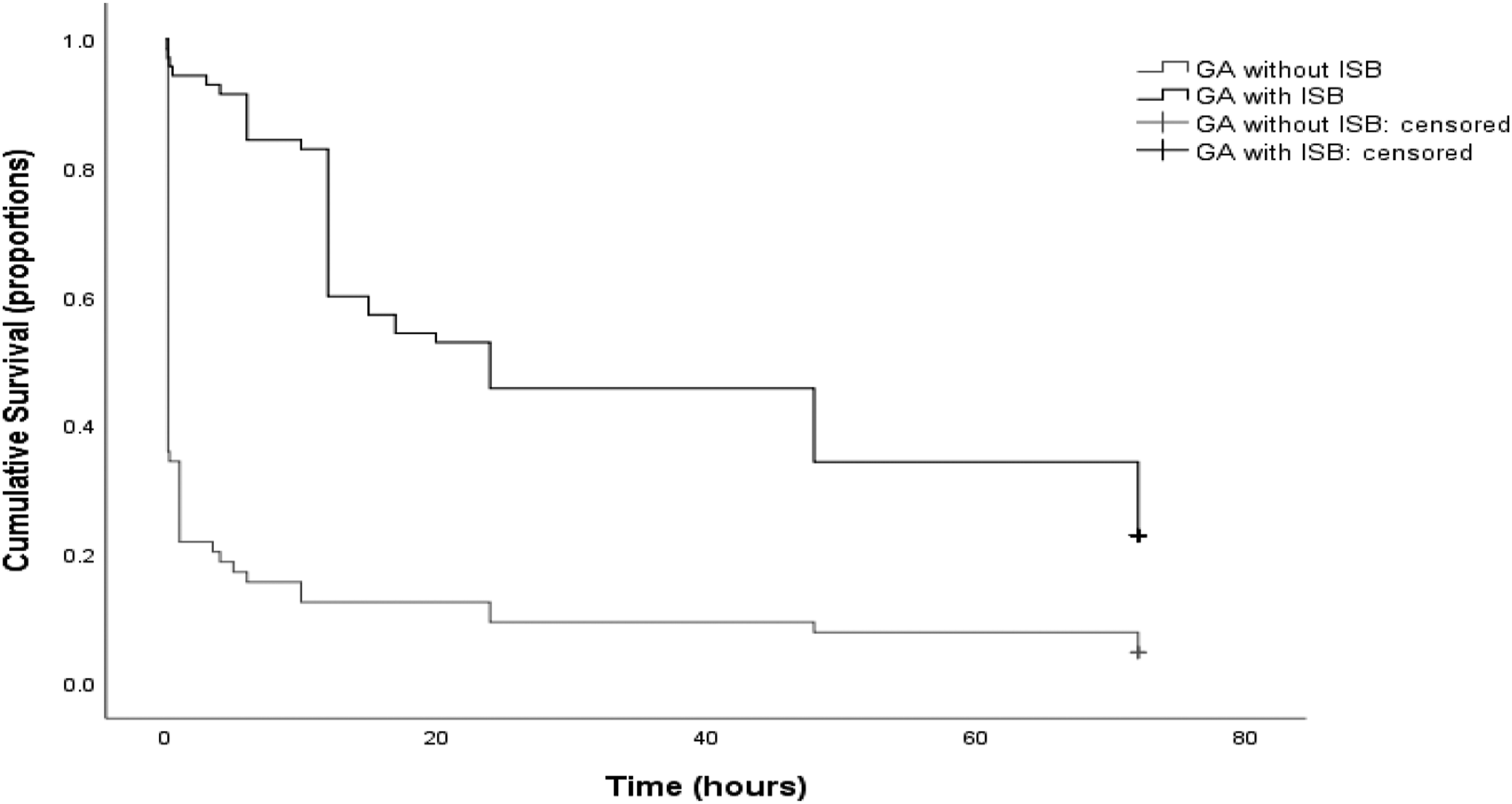
At one-month follow-up, 99 patients completed the follow-up measurements. Average NRS pain score was 2.45±2.7. However, the number of patients who continued to use opioids was significantly higher in the group who did not receive ISB versus the group that did (23.4% vs. 8.6%, respectively, p=0.013). The functionality mean QuickDASH scores were 63.9 ± 17.2 at 1 week and 36.4 ± 19.8 at 1 month. It was significantly better at 1 week (59.6 ± 18.56 vs 68.8 ± 14.16, respectively, p=0.02), but also at 1 month (32.8 ± 19.81 vs 40.6 ± 19.04, respectively, p=0.049) in patients who received ISB versus those who did not. However, mixed model analysis failed to identify ISB as a predictor of better functionality.
NRS satisfaction with pain management scores were consistently high at all-time points: at 24 h (9.3±0.4), 1 week (9.3 ± 1.2) and 1 month (9.1 ± 1.7).
Discussion
Our study showed that omitting a single shot ISB is a strong predictor of postoperative pain and opioid consumption in the early postoperative phase, beyond which the type of surgery, particularly rotator cuff repair and stabilization surgery, emerges as the most important predictor of postoperative pain and functionality.
We are living through the era of opioid crisis where the use of perioperative opioids should be closely scrutinized. More than a quarter of patients on chronic opioid therapy had their opioid treatment started after surgery. 12 Furthermore, new persistent opioid use might occur not only after major surgeries but also after supposedly less painful minor procedures in more than 6% of the cases. 13 A recent preclinical study in rats suggests that repeated postoperative morphine doses prolong postoperative pain, perhaps leading to the persistence of post-surgical pain. 14 Opioids have long been considered as the cornerstone of postoperative pain management. However, recent data showed that neuroadaptation prevents opioids' ability to provide long-term analgesia and may produce opposite effects, such as enhancement of existent pain and facilitation of chronic pain development, through two interrelated phenomena: tolerance and opioid-induced hyperalgesia. 15 Therefore, a paradigm shift has occurred favoring the use of opioid-free or opioid-reduced anesthesia and analgesia protocols. Our findings shed additional light on the predictors of increased pain and opioid consumption following minimally invasive shoulder surgery and emphasize the importance of regional anesthesia as a measure to decrease postoperative opioid consumption.
We showed that omitting regional anesthesia is an independent predictor of higher pain scores following arthroscopic shoulder surgery. As a consequence, omitting ISB was also a predictor of increased opioid consumption following surgery. Omitting regional anesthesia also resulted in significantly more patients (up to 23%) still using opioids 1 month following surgery as compared to 9% of those who received an ISB, clearly predisposing patients to persistent postoperative pain. 15 Later during the postoperative period, stabilization surgery, and rotator cuff repair emerged as predictors of higher pain scores, whereas decompressive surgery was associated with lower pain scores and opioid consumption. In addition, presence of preoperative pain and NSAIDs consumption were predictive of higher pain scores and opioid consumption after surgery. Furthermore, stabilization surgery and rotator cuff repair were predictive of lower functionality after surgery.
Our study failed to identify patient-related independent predictors of the studied outcomes. We only found a significant association between female gender and lower functionality. Previous studies of post-surgical pain models identified female gender as a risk factor for increased postoperative pain. 5 The fact that almost two-thirds of our surgical population were males, could explain why this was only a weak finding in our study.
Previous studies have also found a strong correlation between preoperative anxiety and postoperative pain. 8 Dekker et al. noted that anxiety and depression had a negative correlation and a worse functional outcome in arthroscopic subacromial decompression. 7 Our study population had very low baseline anxiety scores (mean of 1.8) which explains the lack of correlation with post-surgical pain and opioid consumption. In addition, we only measured anxiety using the NRS which was previously found to correlate with the Preoperative State Trait Anxiety Inventory (STAI) scores. 8 However, we did not include in our study psychometric assessments or detailed psychosocial characteristics of patients which were found to be predictive of pain post arthroscopic rotator cuff repair. 16
None of the previous studies on predictors of postoperative pain included the type of anesthesia as an independent variable. The use of ISB was the most significant factor predicting less postoperative pain and opioid consumption in our study. Warrender et al. in their systematic review recommended ISB as the most effective analgesic for out-patient shoulder surgery. 17 A more recent systematic review showed similar results. 18 Chen et al. noted the reduced demand for PCA analgesics and decreased opioid-induced adverse events following shoulder surgery when ISB was performed. 19 However, despite a lower incidence of severe pain, a longer time to first analgesic request, and better functionality as measured by the QuickDASH scores at 1 week and 1 month follow-up in those patients who received ISB as compared to those who did not, ISB was not found to be an independent predictor of improved functionality at 1 week and 1 month follow-up. Similarly, Hofmann-Keifer found that continuous ISB compared with opioid-based patient-controlled analgesia improved analgesia but not function during early rehabilitation of the shoulder joint following surgery. 20 Furthermore, Stiglitz et al. showed the efficacy of ISB as an analgesic modality, but its effect on the long term was not demonstrated. 21 It is also worth mentioning that we did not observe any rebound pain when the effect of the ISB faded away on D1 and D2 as previously reported,21,22 and significantly more patients who did not receive ISB continued to use opioids at the 1 month follow-up as compared to those who received ISB.
Surgery-related factors, specifically rotator cuff and stabilization surgery emerged as independent predictors of pain at 24 and 72 h once the masking effect of the ISB subsided around 24 h following surgery. Rotator cuff repair and stabilization surgery were also associated with lower functionality at 1 month. Similar results were reported by Stiglitz et al. who found that rotator cuff repair was the most painful arthroscopic intervention in the immediate postoperative period requiring the highest morphine administration, followed by instability surgery, while the least painful was decompressive surgery. 21 In contrast, Menendez et al. observed that neither surgical duration nor procedure type were associated with postoperative pain intensity and that psychological and behavioral issues seem to have more influence. 5 Dunn et al. showed that the size, morphology, and structural factors of a tear play a limited role in predicting pain and function in patients with rotator cuff tears. 23 Similarly, Ravindra et al. and Cuff et al. confirmed that tear-specific structural factors were not predictive of postoperative pain.6,16 In addition to the type of surgery, in our study the presence of preoperative pain and NSAIDs consumption were independent predictors of pain and opioid consumption after shoulder surgery. In addition, preoperative pain predicted lower functionality during the follow-up period. Since opioid use for non-cancer chronic pain is restricted in our country, none of our patients was on opioids preoperatively. Kim et al. found that initial high visual analog scale (VAS) scores resulted in higher than average pain scores following arthroscopic rotator cuff repair. 24 Cuff et al. found that preoperative opioid use was a predictor of postoperative pain. 6 Both observations are in line with our results.
We observed that patient satisfaction was high in all patients and was not impacted by the pain management modality or by any of the studied variables. This agrees with a previous study by Stiglitz et al. where 84% of the patients were satisfied or very satisfied irrespective of the pain protocol used. 21 This might be explained by the fact that satisfaction could be influenced by other factors related to the patient’s overall surgical experience. 25
One limitation of our study is that it is an observational study where we did not control for any of the studied variables. We selected a mixed linear model of 5 variables that were found to be the most statistically and clinically meaningful. Another limitation could be a suboptimal pain management protocol in the patients who did not receive an ISB. Adding additional analgesics, adjuvants, or local anesthesia infiltration techniques could have yielded different results. A third limitation is that we did not follow-up on our patients beyond 1 month. Therefore, the correlation between persistent opioid use and the development of chronic pain could not be studied.
Future studies could account for long-term effects of analgesic regimens on functionality and chronic pain following minimally invasive shoulder surgery. The influence of type of surgery and anesthesia on long-term outcomes beyond 1 month remains to be defined.
Conclusions
Our study identified high-risk patients who would benefit from a patient-centered approach with customized pain protocols. Patients who had preoperative shoulder pain and NSAIDs consumption and did not receive regional anesthesia experience more pain and have higher opioid consumption during the first 24 h after surgery. Patients who underwent rotator cuff repair and stabilization surgery had higher pain scores and lower functionality beyond 24 h and up to 1 month. Future studies are needed to identify predictors beyond 1 month.
Supplemental Material
sj-pdf-1-osj-10.1177_10225536221094259 – Supplemental Material for Predictors of postoperative pain, opioid consumption, and functionality after arthroscopic shoulder surgery: A prospective observational study
Supplemental Material, sj-pdf-1-osj-10.1177_10225536221094259 for Predictors of postoperative pain, opioid consumption, and functionality after arthroscopic shoulder surgery: A prospective observational study by Carine Zeeni, Layal Abou Daher, Fadia M Shebbo, Naji Madi, Nada Sadek, Hasan Baydoun, Muhyeddine Al-Taki and Marie T Aouad in Journal of Orthopaedic Surgery
Footnotes
Authors contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The data related to this manuscript is available from the corresponding author upon the Journal’s request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.