
Abstract
Background
China has neither a nationwide joint replacement registry similar to Sweden and New Zealand nor a universal healthcare (medical insurance) registry similar to Hong Kong and Singapore to check. The purpose was to initially understand the distribution characteristics of gender, age and etiology of patients undergoing total hip replacement for non-traumatic reasons nationwide.
Methods
The clinical data of patients who underwent initial artificial total hip replacement due to non-traumatic reasons in joint surgery of 13 large general first-class hospitals at Grade 3 in northern, western, eastern, southern, and southwestern China were collected. After the classification of patients by gender, the etiological characteristics and age distribution of male and female patients were compared, as well as male to female ratio and disease composition ratio of patients of different ages, distribution of causes in different regions, composition ratio, and age distribution characteristics of patients of different ethnic groups.
Results
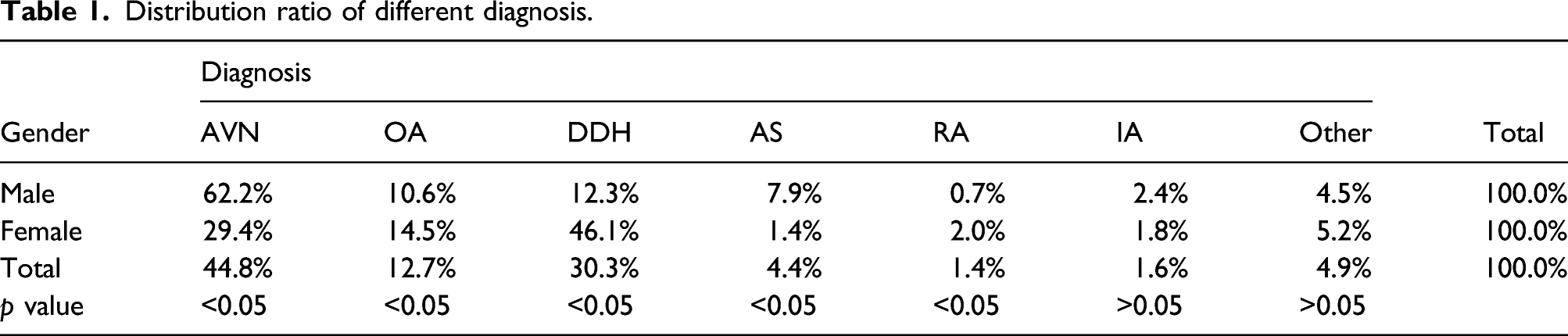
In this study, the data of a total of 7663 patients in joint surgery of 13 general first-class hospitals at Grade 3 from 2015 to 2017 were collected, and 7622 patients were finally included in the study after excluding missing age, gender and some foreign patients. The main causes of diagnosis in male patients were AVN, DDH, and OA, and top 3 causes in female patients were DDH, AVN, and OA.
Conclusions
This study initially understand the distribution characteristics of gender, age and etiology of patients undergoing total hip replacement for non-traumatic reasons nationwide, and further guide the clinical diagnosis, early prevention and treatment of the disease and provide data.
Introduction
Artificial total hip replacement is one of the important measures for the treatment of advanced hip joint disease. There are a number of causes of total hip replacement, including aseptic necrosis of femoral head, congenital dysplasia of hip, rheumatoid arthritis, and traumatic causes. 1 Affected by different epidemiological characteristics of the disease, the epidemiological characteristics of different causes are varied. Since China has neither a nationwide joint replacement registry similar to Sweden and New Zealand nor a universal healthcare (medical insurance) registry similar to Hong Kong and Singapore to check, therefore, the etiology study related to hip replacement is only the survey data of a single institution or a certain region. There is a vast territory and many ethnic groups in China, so it is necessary to expand the number and scope of collected data and conduct multi-regional and multi-center analysis in order to fully understand the etiology of total hip replacement. In this paper, the basic data and etiology of 7622 patients who underwent total hip replacement due to non-traumatic reasons in 13 large general hospitals in China were summarized and analyzed. The purpose was to initially understand the distribution characteristics of gender, age, and etiology of patients undergoing total hip replacement for non-traumatic reasons nationwide, so as to further guide the clinical diagnosis, early prevention and treatment of the disease and provide data.
Methods
Data collection
The clinical data of a total of 7663 patients who underwent initial artificial total hip replacement due to non-traumatic reasons in joint surgery of 13 large general first-class hospitals at Grade 3 in northern, western, eastern, southern, and southwestern China were collected. Inclusion criteria: i. Patients who were hospitalized in the above 13 hospitals for initial artificial total hip replacement and those who underwent staged bilateral hip replacement due to the same diagnosis were included as one case; ii. Patients with complete medical records, preoperative imaging examinations and clear discharge diagnosis. Exclusion criteria: i. Patients undergoing artificial hip revision and hemi-hip replacement; ii. Patients undergoing total hip replacement in the late stage of femoral head necrosis and traumatic arthritis due to failure of internal fixation of femoral neck fractures caused by trauma; iii. Patients with preoperative diagnosis of fractures around the hip and those with nonunion. After screening, data of 7622 cases were retained.
Determination of diagnosis method
Patients were divided into 7 groups according to the International Classification of Diseases ICD-10 on the basis of the etiology of hip replacement in discharge diagnosis from the hospital, including aseptic necrosis of femoral head (AVN), primary osteoarthritis (OA), congenital dysplasia of hip (DDH), ankylosing spondylitis (AS), rheumatoid arthritis (RA), and infectious arthritis (IA). From under 20 years old to over 90 years old, every 10 years was an age group, divided into 9 age groups. All the collected imaging data were reviewed by two senior chief physicians of joint surgery. After the registration of discharge diagnosis unmatched with imaging examination, the patient’s complete medical records would be obtained and combined with the medical history, surgical record or pathological diagnosis for final diagnosis or classification. For diagnosed cases with multiple hip joint diseases, the first diagnosis took priority. The patient’s age and gender composition ratio were compared. After the classification of patients by gender, the etiological characteristics and age distribution of male and female patients were compared, as well as male to female ratio and disease composition ratio of patients of different ages, distribution of causes in different regions, composition ratio and age distribution characteristics of patients of different ethnic groups.
Statistical analysis
SPSS17.0 software was adopted for statistics, chi-square test was performed on the age, gender and disease diagnosis composition ratio between the data, and p < 0.05 indicated that the difference was significant.
Results
Basic patient information and total etiology diagnosis composition
In this study, the data of a total of 7663 patients in joint surgery of 13 general first-class hospitals at Grade 3 from 2015 to 2017 were collected, and 7622 patients were finally included in the study after excluding missing age, gender and some foreign patients. The average age of all patients at the time of surgery was 54.6 ± 14.0 years. There were 3575 male patients, accounting for 46.9%, 52.9 ± 13.9 years old at surgery, and 4047 female patients, accounting for 53.1%, with an average age of 56.0 ± 13.9 years at surgery. The proportion of AVN was the highest among all etiological diagnoses, followed by DDH and OA, as shown in Figure 1. Proportion of different etiology.
Comparison of disease composition and age of patients of different genders
Distribution ratio of different diagnosis.
Number, gender ratio, and etiological composition ratio of patients in different age groups
The age range of patients was 13–92 years. The total number of patients increased with age to reach the peak proportion (26.9%) in 50-year-old age group. The peak number of male patients appeared in 50-year-old age group, and that of female patients appeared in 60-year-old age group. The proportion of patients <40 years old and>80 years old decreased, as shown in Figure 2. With the increase of age, the proportion of patients with AVN and DDH gradually increased, and decreased significantly after reaching a peak in 50-year-old age group. The proportion of OA patients reached a peak in 60-year-old age group, and decreased significantly in 80-year-old age group. Patients with the etiological diagnosis of AS reached the highest proportion in 30-year-old age group. There was no statistical difference in the proportion of AVN and DDH in 60-year-old age group, as shown in Table 2. The number of patients by age and gender. Etiology distribution in different age groups.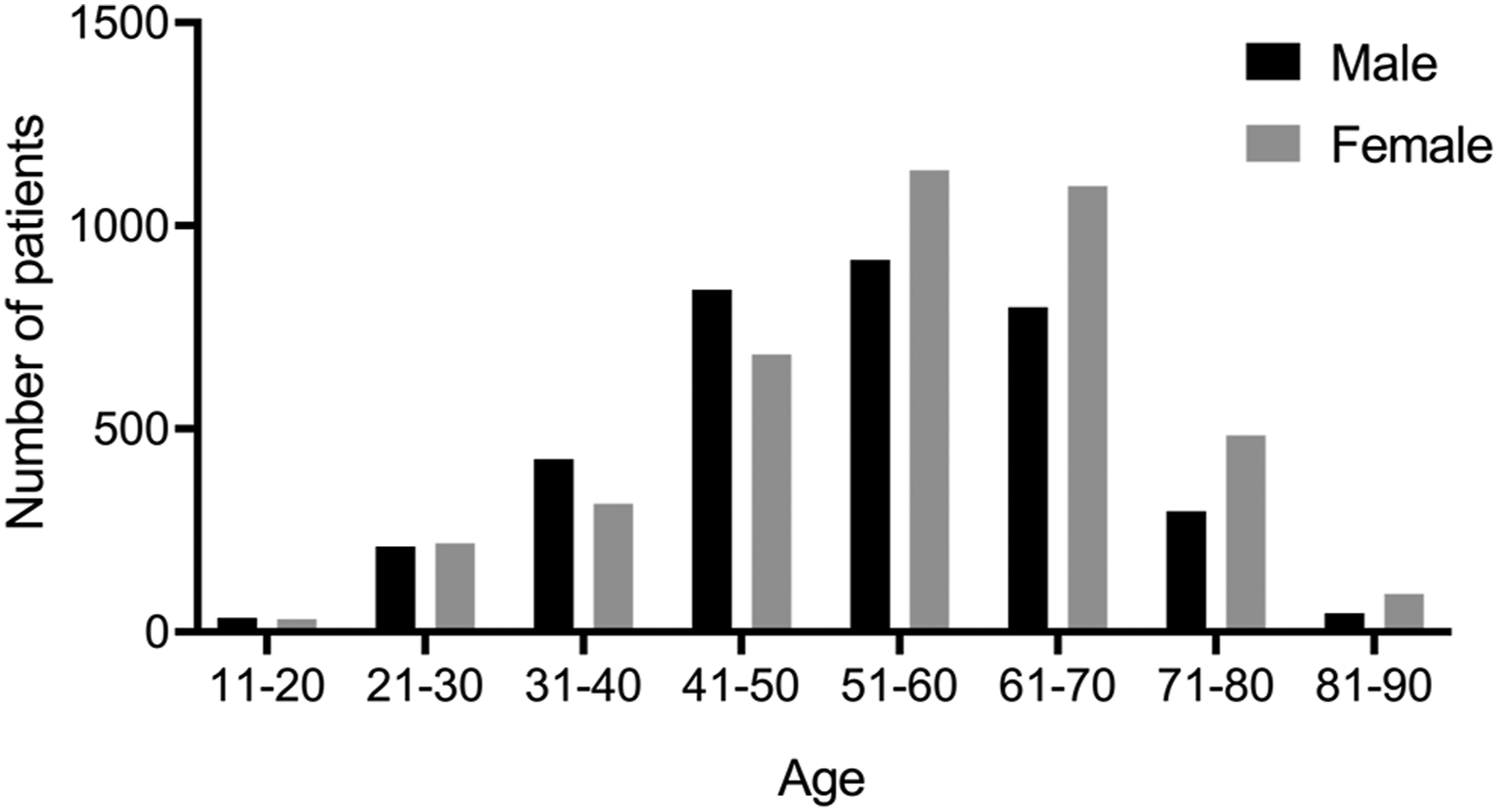

Differences in the etiology of surgery in different regions
Etiology distribution of patients in different regions.

Comparison of the etiological differences between minority patients in western China and Han patients at surgery
Etiology distribution of ethnic minority patients and Han nationality patients in Northwest China.

Discussion
In this paper, the basic data and etiology of patients who underwent artificial total hip replacement for non-traumatic reasons from 13 hospitals in different regions of China from January 2015 to January 2017 were summarized and analyzed, so as to initially understand the distribution characteristics of gender, age and etiology of patients undergoing total hip replacement for non-traumatic reasons nationwide, and further guide the clinical diagnosis, early prevention and treatment of the disease and provide data.
The epidemiological characteristics of aseptic necrosis of femoral head are mainly young and middle-aged, with more males than females. South Korean Kang et al. 2 reported that in 2006, about 100,000 cases of necrosis of femoral head were diagnosed and treated in South Korea each year, with an average of 14,000 new cases each year, accounting for 50%–60% of hip replacement. 3 Reports show that there are 20,000 new cases each year in the US, and surgical patients account for 5%–12% of all THA cases in the joint registry.4,5 In 2017, the proportion of AVN in the initial THA recorded by AJRR registry was 3.7%. West China Hospital, Sichuan University reported that from January 2010 to December 2012, AVN accounted for 31% of hip replacement during the same period. The previous research reported that among 974 patients, avascular necrosis of femoral head accounted for 53%. AVN was diagnosed in 44.8% of the data in this group. Fresh cases of femoral neck fractures were excluded in this study, as well as AVN caused by internal fixation failure and fracture nonunion. However, the proportion of AVN was still much higher than that reported in Europe, America and other countries, and was close to the proportion reported in China. Reasons: First, from the results of epidemiological investigation, the incidence of AVN in China is high. The research report on necrosis of femoral head in China shows that the incidence of AVN is higher than that of Asian countries such as Japan and South Korea and much higher than that of the United States. There are more female patients in China and more patients in north. 6 Second, patients often experience misdiagnosis and missed diagnosis due to low level of early diagnosis of AVN in China, which affects early treatment and prevention of femoral head collapse. Third, some patients in the early stage of treatment receive TCM, its role in early treatment needs to be further studied, and there is currently no drug that is clearly effective in the treatment of AVN. 7 Finally, the living and eating habits of Chinese people and European and American countries have obvious regional differences. 6
Hip osteoarthritis in the elderly is an important cause of hip pain and dysfunction. About 4% of people over 65 in the United Kingdom suffer from hip osteoarthritis. In the United States, hip osteoarthritis affects approximately 5% of the population over 60 years of age. 8 Osteoarthritis can be divided into primary and secondary. Hip dysplasia, avascular necrosis of femoral head, rheumatoid arthritis, infectious arthritis, and ankylosing spondylitis can all be secondary to osteoarthritis. In this study, the above diagnosis was used as the cause alone for analysis. The etiology of primary osteoarthritis is still not fully understood at present. Systemic factors include age, gender, race, genetic susceptibility, and other possible factors, such as osteoporosis, vitamin deficiency, and the lack of some growth factors. Local factors include the local injury of joints, body weight, weak muscle strength, and some congenital or developmental joint shape changes. 9 The British epidemiological survey showed that the prevalence of primary hip osteoarthritis was 7.0%, and the average rate in European countries was 4.0%. Research reports in Hong Kong showed that the local prevalence of primary hip osteoarthritis was 0.4%, 10 while the prevalence of primary hip osteoarthritis reported in South Korea and Beijing, China was close to 1%,11,12 much lower than that in European and American countries. In the past 20 years, primary hip osteoarthritis has been the leading cause of THA in Swedish registry, accounting for 83%. AJRR in 2017 reported that osteoarthritis accounted for 92.8% of all initial THA. Hoaglund et al. 13 reported earlier that primary hip osteoarthritis accounted for 11.72% of patients undergoing total hip replacement in 15 hospitals in the San Francisco, but the proportion of Chinese people was much lower than that of the white race, only 0.44%. A survey conducted by Oishi et al. 14 in 8 hospitals in Hawaii showed that in all cases of total hip replacement, the proportion of the white race with primary hip osteoarthritis was 3–20 times higher than that of Asians and Pacific Islanders. The proportion of primary hip osteoarthritis in this study was 12.6%, close to that reported in Hong Kong and Taiwan.15,16
The cause of DDH is unclear, and its epidemiological and demographic data vary greatly. There are epidemiological reports that the incidence of infant unilateral joints is 63.4%, and the incidence of left hip is slightly higher at 64.0%. The incidence of live births in the US ranges from 0.06‰ for Africans to 0.076% for Native Americans. The incidence of the same race also varies significantly with geographic locations from 0.4 for Africans to 61.7% for Caucasians in Poland. Risk factors for DDH include family history and female infants, premature birth, low birth weight or multiple births. 17 The etiology statistics of the Swedish joint replacement registry did not separately list DDH, but classified it as a childhood disease, accounting for 2%. 18 The US AJRR statistical results attributed patients with DDH in initial THA to other diagnoses, and the proportion was less than 2.6%. Statistics from Queen Mary Hospital in Hong Kong from 1998 to 2010 showed that DDH cases accounted for 6.4% of all THA. The etiological analysis of 105,688 THA patients in Taiwan from 1996 to 2004 showed that congenital diseases accounted for 0.5%. In this study, the proportion of patients diagnosed with DDH as the cause was significantly higher than the above reports at home and abroad. Reasons: First, there are complete neonatal congenital disease screening systems in developed regions such as Europe and the US, and early diagnosis can be achieved through early screening, so as to significantly increase the hip preserving rate, reduce the prevalence of adult DDH, and delay the age of joint replacement. Second, the prevalence of adult DDH will increase due to the tradition of infant swaddling in northern China, especially in minority areas such as Xinjiang. Third, although there is no tradition of swaddling in eastern and southern China, and the traditional morbidity rate is low, 19 DDH patients in economically developed regions especially in Shanghai and Guangzhou have higher requirements for quality of life, and the advanced local medical technology has a high diagnosis rate for adult DDH, which has also increased the proportion of DDH in THA cases in recent years. Finally, with the advancement of prosthesis design and the improvement of surgical technology, the life of hip prosthesis has been extended, which objectively promotes the treatment of THA in young DDH patients.
Global prevalence of RA is about 1.00%, and that in mainland China is about 0.36%–0.50%, with large regional differences. Studies have shown that 50–60 years of age is the peak age of onset, and RA is more common in females, with the total number being 3 times that of males, and females under 50 years of age are 5 times that of males. 20 Wolfe et al. 21 conducted a prospective cohort study on 1600 RA patients and showed that about 25% of RA patients received artificial joint replacement. A study by Louie et al. 22 showed that the proportion of RA patients undergoing surgical intervention gradually decreased since it had peaked in the 1990s. Among young RA patients aged 40–59 years, the hip surgery rates have decreased by 40%. In this study, RA accounted for 1.4% of all THA patients, which was lower than 6.3% in Hong Kong and some early domestic reports, but higher than 0.5%–0.6% in the US and Taiwan. The gender ratio of 2.9:1 was no different from previous reports. The prevalence of RA in southern areas is higher than that in northern areas. In addition to genetic factors and living habits, humid environment is an important environmental factor leading to the onset of RA.
AS is widely distributed all over the world, and the prevalence varies greatly among different races and regions. Genetic factors are generally considered to play a leading role in AS. The prevalence in European and American countries ranges from 0.1% to 1.6%. In Asia, a large retrospective survey in Japan showed that the prevalence was 0.01% from 1985 to 1996. There are different reports on the prevalence of AS in southern and northern China, but the overall prevalence is between 0.20% and 0.54%. In terms of demography, the prevalence in cities with more young adults is higher than that in aging cities. In this study, AS accounted for 4.4% of all THA causes, higher than 0.3% in Taiwan and lower than 10.4% in Hong Kong. There are more young and middle-aged male patients than females, and the ratio of male to female is 4.8:1 lower than that of Hong Kong and Taiwan. The 30-year-old is the age for multiple surgeries, and bilateral replacement is the main one.
The proportion of THA caused by infectious arthritis among THA patients decreases compared with previous studies, which is related to improvement of the quality of life, physical fitness and medical levels. However, the proportion of patients with sequelae of hip infection in Xinjiang is close to that in the southwest (Yunnan, Guizhou, Sichuan), and is significantly higher than that in other domestic regions. Moreover, the proportion of hip tuberculosis patients in this region is also significantly higher than that in other regions, and relevant epidemiological investigations need to be further improved.
Sarzi et al. 16 reported that in cases of hip osteoarthritis, males were more than 50 years old and females were more than 40 years old for onset. This study showed that the average age at surgery of hip osteoarthritis patients was 55.7, which was consistent with the change in average age of hip replacement by Huo et al. 17 The number of patients over 70 years old decreased significantly, mainly due to the increase in the proportion of hip replacement caused by trauma as age increased. Among patients over 70 years old, the proportion of OA patients due to non-traumatic causes of THA increased significantly, close to the ratio of AVN. The proportion of females in patients under the age of 70 was higher than that of males, which might be related to the higher proportion of DDH in females than in males. For those over 70 years old, the ratio of male to female patients tended to be balanced. Cases caused by trauma were not included in this paper. Relevant studies showed that after the inclusion of acute hip fracture cases, the proportion of females was still more than that of males, which might be related to the decrease in estrogen levels in females after menopause. The decrease in estrogen levels caused hip fractures as well as prevalence of THA in females. Jordan 18 reported that female OA was more common in the knee while it was more common in the hip for males. Juhakoski et al. 20 conducted a large-scale epidemiological survey on hip joint disease in the population and found that the incidence of hip osteoarthritis among heavy workers was higher than that of light workers. However, this group of data showed 10.6% of male patients with hip OA and 14.5% of females. The reason might be due to the low prevalence of primary OA in Asians, and some female patients with hip impingement syndrome and mild DDH suffered from OA due to unclear diagnosis in the early. Vincent et al. 19 reported that the average age of males among artificial total hip replacement cases in the US was lower than that of females, which was consistent with the average age ratio of males and females in this study. Statistics in this group showed that the proportion of male patients under the age of 50 increased, and there were mainly AVN patients, rather than OA, which might be caused by males who drank heavily in China.
China is a multi-ethnic country. The living habits of different ethnic groups in different regions are different, as well as ethnic genetic background. From China’s geographical division in the traditional sense, this group of data shows that the difference in etiological diagnosis between northern China, eastern China, northwestern and southwestern China is statistically different in the proportion of AVN patients in the southwestern region of the top three causes than in other regions. The proportion of THA due to OA in the northwestern and southwestern regions has dropped significantly. It is related to the inconsistent diagnosis criteria of OA in the local area. Many patients are attributed to AVN diagnosis. In addition, the high cost of THA restricts some patients from seeking surgery for minorities and economic less-developed regions. Even so, 419 minority cases in Xinjiang were still collected in this study, mainly Uyghur and Kazak, accounting for 95%. The proportion of AVN in minority patients receiving total hip replacement is obviously lower than Han patients in the same region, and the ratio of AVN is significantly higher than the average ratio of the same region and the whole country. In the past, only single-center studies showed that the positive rate of screening for hip dysplasia in minority newborns in Xinjiang was not significantly different from the domestic average, but related multi-center studies did not reported. Therefore, it is necessary to further carry out the epidemiological investigation and research on AVN of minorities in Xinjiang, meanwhile expanding the scope of epidemiological investigation of DDH in minority adults to clarify reasons for the increase in the rate of hip dysplasia in infants and young children.
Conclusion
In this study, although the causes were determined by multiple centers based on clinical, radiological, and intraoperative pathology, there are still some patients suffered with end-stage hip osteoarthritis and multiple hip diseases in the meanwhile, and it is difficult to determine the cause of surgery and will cause a certain degree of information bias. Affected by customs, medical levels and economic factors, the epidemiological characteristics of a disease itself cannot fully represent the etiology epidemiological characteristics of the surgery. In addition, due to the fact that a national joint replacement registry has not yet been established in mainland China, the data entered by the national medical insurance and hospital management systems are limited, resulting in the data source of this study being limited to joint surgery centers in several larger hospitals. It may not be accurate to extend the results of this study to the population of the whole country, but this is the etiological analysis study with the largest number of cases and the widest geographical coverage. Therefore, it is necessary to establish a national joint replacement registry and conduct a related larger-scale epidemiological survey.
Footnotes
Acknowledgments
We are indebted to the authors of the primary studies.
Author Contributions
Y. Ma and H. Zhang designed and performed research.
Y. Ma and X. Zhi analyzed data.
Y. Ma and H. Zhang: data interpretation.
Y. Ma and X. Zhi wrote the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Availability of data and material
The datasets are available from the corresponding authors on reasonable request.