
Abstract
Introduction
Inferior angle of scapula fractures (IAS) are rare injuries that result from the strong periscapular shoulder muscles avulsing the inferior scapula tip. The first case was published in 1981 by Hayes et al., 1 and since then only 11 further cases in seven articles have been published in the literature. Two of these cases did not contain details about the fracture mechanism and outcome. Chang et al. 2 published a review of the other 10 cases, and found that if displaced (n = 7), all fractures treated non-operatively showed no evidence of union, with persisting pain and scapula winging. All these fractures however, following open reduction internal fixation (ORIF), demonstrated resolution of symptoms and return of shoulder function. The undisplaced fractures (n = 3) had mixed outcomes reported, with one poor outcome reported in a fracture that later became displaced. From this review, treatment recommendations were made including surgical fixation of displaced fractures. Guidelines based on a collection of case reports however have the inherent issues of reporting bias, with only interesting cases being published and the results being non-representative of the actual injury. There are no published studies examining the epidemiology and natural history of IAS fractures, with only theses case reports available to guide treatment.
The goal of this study was to perform a retrospective review of IAS presenting to three major trauma centers, to investigate the epidemiology and natural history of this poorly understood injury.
Methods
Ethics approval was given from the research ethics committee of each participating hospital. The study period was 2012–2018. Patients were identified for this study using the hospitals’ computered tomography (CT) reporting systems. As no standard term for IAS exists, CT reports were searched to identify those that included the terms ‘scapula’ and ‘fracture’. The CT images of reports containing both terms were then manually reviewed to identify patients with an IAS. Inclusion criteria were the presence of an IAS. Exclusion criteria were presence of a concomitant scapula body fracture or other scapula fracture that extended to the inferior angle of the scapula. The case notes of included patients were then reviewed. Data collected included patient age, gender, mechanism of injury, fracture pattern, displacement, treatment received and outcome. Patients were also contacted via telephone a minimum of 1 year following their injury to collect data relating to pain and Quick-DASH score. Fractures were classified as ‘undisplaced’ if there was cortical contact between the fracture fragment and the scapula regardless of angulation. Fractures with no cortical contact were classified as ‘displaced’. Patients were excluded from the outcome analysis if they died prior to any follow-up being documented.
Results
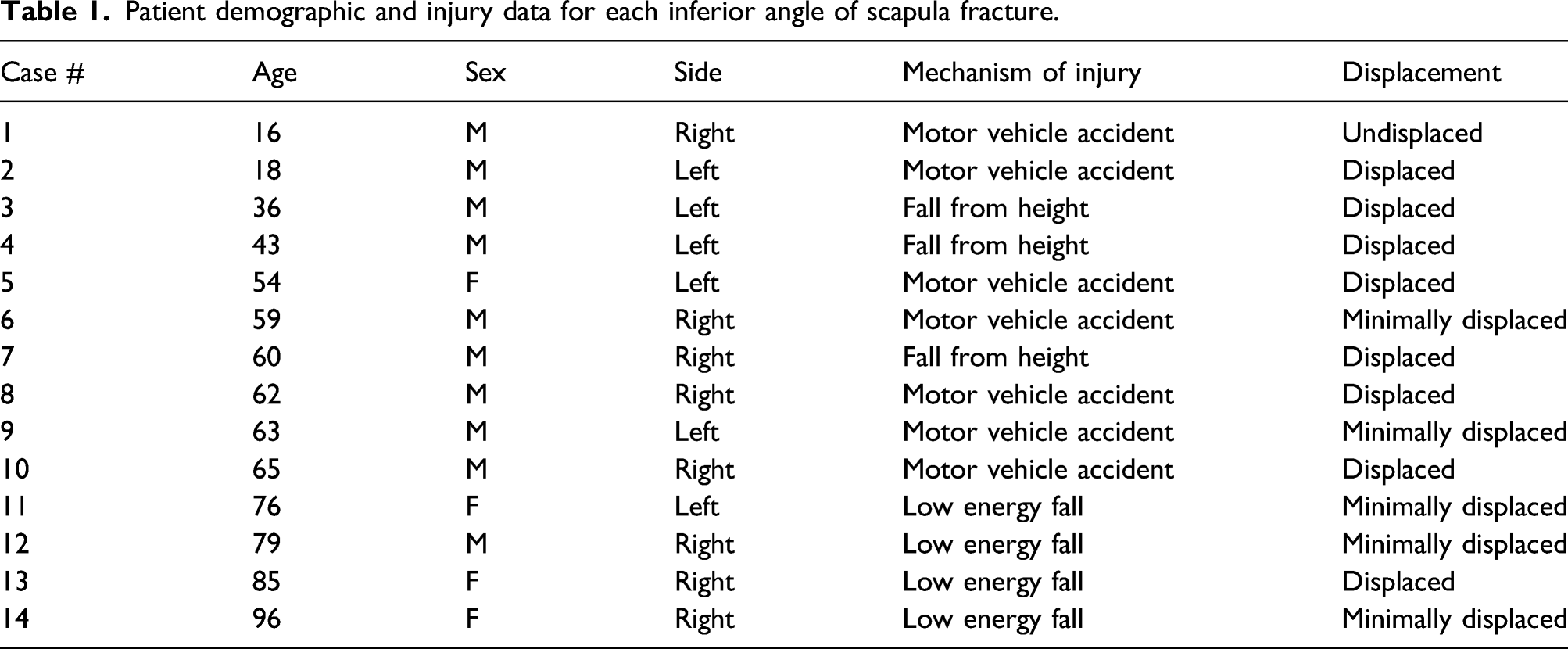
Patient demographic and injury data for each inferior angle of scapula fracture.
Eleven patients had a shoulder X-ray performed prior to CT. The fracture was not identified in the X-ray report in 5 cases (45.5%). Additionally, one fracture not reported on X-ray was also not reported on CT. It was identified for inclusion in this study as a concomitant coracoid fracture was reported.
Eight (57.1%) fractures were displaced (Figure 1), all in an anterior direction. The remaining six fractures were undisplaced or minimally displaced. Figure 2 demonstrates the main fracture line for each of the 14 injuries. Larger fractures did not have a greater tendency to be displaced. All patients were initially treated non-operatively in a sling. Eight were discharged directly from the emergency department with no follow-up booked and six were followed-up in the Orthopaedic outpatient clinic. 3D CT reconstruction of an inferior angle of scapula fracture. Main fracture lines for all 14 inferior angle of scapula fractures.

Undisplaced fractures
There were six undisplaced fractures. One was excluded from the outcome analysis as the patient died from an unrelated cause. Four patients were able to be contacted by telephone 1 year or more following the injury. All reported a Quick-DASH score of zero, and pain score of zero or one out of 10. One patient was not contactable by telephone but attended a follow-up appointment 3 months post injury with documentation of no pain and satisfactory shoulder function, and was subsequently discharged. No patients with an undisplaced fracture have an unsatisfactory outcome.
Displaced fractures
Of the eight displaced fractures, six were contactable by telephone. Three (50%) reported a good outcome with non-operative treatment with no pain and a Quick-DASH score of zero. The other three reported an unsatisfactory outcome with non-operative treatment; two had undergone subsequent surgical fixation due to significant ongoing pain and scapula winging. One underwent ORIF of the displaced fragment 4 weeks post-injury with the fragment found to be attached to latissimus dorsi and serratus anterior. The second had excision of the fragment with reattachment of the rhomboid major musculature to the inferior angle of the scapula 5 years post-injury. Both reported good outcomes following surgery with no significant pain or functional limitation. The third patient with an unsatisfactory outcome reported a pain score of 7/10 with a Quick-DASH score of 75. This patient was never offered surgical treatment. Two patients were not contactable. One had died and one did not have contact details available. Outcomes of non-operative treatment are shown in Figure 3 Outcomes of non-operative treated displaced versus non-displaced fractures.
Discussion
Inferior angle of scapula fractures a rare injury with only 12 cases previously reported.1–7 This study demonstrates there appears to be a bimodal distribution of injury (although the case numbers are small), with high energy trauma accounting for injuries in younger males, and low energy trauma in older individuals. Males were found to be affected more commonly than females in a 5:2 ratio.
The anterior displacement or angulation seen in IAS fractures is due to the muscles attached to the inferior angle of the scapula. The inferior angle thoracic surface is attached to serratus anterior laterally and medially. The posterior surface is attached to teres major laterally and rhomboid major medially. Additionally, the inferior tip is attached to latissumis dorsi in 43% of people. 8 Four previously published cases included a description of the muscular attachments to the IAS fragment.1,2,4,6,7 The displaced fragment was attached to both serratus anterior and latissimus dorsi in two cases, and serratus anterior alone in two further cases. This series identified a case with rhomboid major attached to the avulsed fragment.
Non-operatively treated displaced fractures have previously been shown to all do poorly,1,2,4,6,7 however as the only published literature is in the form of case reports, this may be due to reporting bias. This retrospective series demonstrated half of the displaced fractures had a good outcome without an operation, and half did poorly, with ongoing pain and dysfunction. The available documentation and imaging did not provide a clear explanation as to why only some patients continued to be symptomatic. The authors postulate that ongoing disability may be related to scapula winging resulting from the inferior pole and attached musculature no longer stabilizing the scapula. Scapula winging has been consistently reported in those with symptomatic, displaced IAS fractures in the literature.1,2,4,6,7 The two patients in this series that underwent surgical reattachment of the avulsed musculature to the inferior angle of the scapula, had resolution of their symptoms and restoration of shoulder function, as did all patients in previous case reports. All undisplaced or minimally displaced fractures in this series had a good outcome with non-operative treatment, however mixed outcomes have previously been reported with an initially undisplaced fracture becoming displaced resulting in persisting pain.
This series has several limitations. Being an unusual condition, the number of patients recruited is too small to give any significant conclusion and impact daily practice. The retrospective nature of the study also has inherent difficulties including lack of consistency with documented outcomes measures. Cases for inclusion in this study were identified using CT reports as the authors had experienced IAS fractures being missed on plain radiographs. Is it likely however that only a portion of these injuries were identified? Others many have been seen on plain radiographs but no CT performed, undisplaced fractures may have not been identified or reported, and if minimal symptoms were present, some fractures may not have been imaged at all. As the only retrospective series examining IAS however, it still provides some useful insights into this poorly understood injury. Importantly, the previous recommendations around IAS fractures based on published case reports concluded that displaced fractures should undergo operative fixation, whereas this series showed that some displaced fractures will have a satisfactory outcome without surgery.
Conclusion
Inferior angle of scapula fractures are a rare injury with a bimodal distribution. Younger individuals sustain this injury from high energy trauma, and older individuals from low energy trauma. They are often missed on X-ray therefore if there is clinical suspicion of an IAS fracture including tenderness at the inferior angle or scapula winging, a CT scan should be performed. Identifying a displaced IAS fracture is important as they can do poorly when treated non-operatively and need to be followed-up appropriately. For displaced fractures with ongoing pain and shoulder dysfunction, surgical intervention to reattach of the avulsed musculature to the inferior angle with or without the bony fragment has been shown to result in resolution of symptoms. Further investigation is warranted into factors that contribute to a poor outcome in displaced fractures. Undisplaced and minimally displaced fracture in this series all had a satisfactory outcome when treated non-operatively and are unlikely to require surgical treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.